

Enhancing the endogenous nutrient levels of DHM to help support the needs of extremely and very preterm infants
Mother’s own milk (MOM) is the first choice for feeding preterm infants; however, if MOM is limited or unavailable, donor human milk (DHM) is the recommended alternative. Exclusively MOM or DHM diets do not provide sufficient levels of key nutrients required by extremely or very preterm infants. This article explores how modifications to donor nutrient intake and milk banking practices can potentially be used to enhance the endogenous nutrient levels of DHM.
Coralie FalizePhD student
falizec@roehampton.ac.uk
Yvonne M. Jeanes
Associate Professor
Simon C. Dyall
Senior Lecturer
School of Life and Health Sciences, University of Roehampton, London
Falize C., Jeanes Y.M., Dyall S.C. Enhancing the endogenous nutrient levels of DHM to help support the needs of extremely and very preterm infants. Infant 2024; 20(3): 84-89.
Appropriate nutrition is fundamental for newborns; especially preterm infants, where their materno-fetal nutrient supply has been prematurely terminated.1 Breast milk provides nutrients, hormones, enzymes and immunological factors that are essential for infant development. The nutritional composition of human milk varies widely, not only over the course of lactation, but also between individuals and populations.2-4 Factors that have been shown to affect nutritional composition include, maternal lifestyle and dietary habits.5
Maternal breast milk is the first choice for feeding neonates;6 however, an inadequate milk supply is nearly three times more likely in preterm mothers than in term mothers.7 Underlying reasons can be physiological, such as incomplete development of the mammary glands, or poor hormonal response, as well as psychological.8 Furthermore, in some cases, maternal breast milk might not be appropriate, due to illness or medication. In these instances, DHM from a human milk bank (HMB) is the recommended alternative.9 In the UK, the British Association of Perinatal Medicine (BAPM) has set out a framework for practice, The Use of Donor Human Milk in Neonates,7 whereby, ‘DHM may be considered in babies born at <32 weeks’ gestation and/or <1,500g to establish enteral feeding when MOM is unavailable or insufficient to meet the baby’s requirements.’ However, it’s noted, ‘There is insufficient evidence to make specific recommendations about duration of DHM use, fortification of DHM and use of DHM in moderate/late preterm and term babies.’
Nutritional needs of extremely and very preterm infants
The nutritional needs of extremely and very preterm infants are not currently met by exclusive diets of maternal or donor milk. For example, a recent study identified that extremely preterm infants fed an entirely human milk diet receive significantly less than the recommended daily vitamin K intake and are consequently at increased risk of vitamin K-dependent bleeding.10 Similarly, we have shown that extremely preterm infants receiving standard care with maternal and DHM receive very low levels of the long-chain polyunsaturated fatty acids (PUFAs), arachidonic acid (ARA, 20:4n-6), and docosahexaenoic acid (DHA, 22:6n-3).1 DHA and ARA are essential for optimal brain, visual and immune system func-tion,11 and during the last trimester, the brain weight increases approximately five-times and at the same time around 80% of the brain DHA and ARA are accumulated.1 Furthermore, we have shown that both donor milk and milk expressed from mothers of preterm infants provide protein levels significantly below the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) recommendations, and an exclusive DHM diet would provide levels of linoleic acid (LA; 18:2n-6), ɑ-linolenic acid (ALA; 18:3n-3), ARA, and DHA significantly below ESPGHAN recommendations.12
The recent position paper of the ESPGHAN Committee on Nutrition and Invited Experts, sets out revised guidelines for the enteral nutrition of preterm infants,13 where it’s noted: ‘In general, there is a lack of strong evidence for most nutrients and topics’ and, ‘We strongly support the use of human milk and recognise that the variation in nutrient density and absorption make precise recommendations for supplements or fortifiers challenging.’ The question therefore arises as to how best enhance and/or preserve the endogenous levels of these nutrients in DHM to support the needs of extremely or very premature infants.
Modification of endogenous nutrient levels of DHM
Breast milk is a highly dynamic fluid and the nutritional content appears to be affected by a wide range of factors, including maternal nutritional intake.4 We therefore suggest, that there are two areas where endogenous nutrient levels of DHM may be modified:
- At the level of maternal nutrient intake, and/or
- After expression when the milk is stored and processed by the HMB.
DHM typically undergoes prolonged cold storage, freeze-thaw cycles and processing before it is given to infants.14 We have reviewed the evidence for the negative effects of these practices on the levels of long-chain PUFAs, lipid mediators and antioxidants in DHM, and have proposed a series of recommendations to mitigate some of these negative effects.14 We suggest that DHM should be protected from light exposure and storage at 4°C minimised, to prevent decreases in vitamin C and endocannabinoids and increases in free fatty acids and lipid peroxidation products. Storage at -20°C prior to pasteurisation should also be minimised, to prevent free fatty acid increase and total fat and endocannabinoid decrease. Storage ≤-70°C is preferable wherever possible, although post-pasteurisation storage at -20°C for three months appears safe for free fatty acids, lipid peroxidation products and total fat content.
A mixed-methods survey
In terms of modifying maternal diet, we reviewed the dietary guidance and advice currently available to donors by the HMBs. Previously (November 2016 to February 2018), we undertook a mixed-methods survey to investigate not-for-profit HMB practices in the UK related to donor selection, nutritional information, and donor milk transport and storage.15 There was an overall response rate of 93% (14 of 15). With regards to nutritional aspects:
- five HMBs reported asking potential donors about their dietary habits (besides alcohol consumption) before the first milk donation; one asked both before and during the time of milk donation; five did not ask at all
- two HMBs excluded mothers from donating if they followed a restricted diet, whereas 11 did not exclude
- only three HMBs had general leaflets or information available to donors about a healthy diet for breastfeeding mothers
- one had a registered dietitian at the HMB, five had registered dietitians at the hospital who could be consulted, and four had no one available
- following donation, nutritional assessment of the DHM for energy, PUFAs, minerals, or peroxidation products was not performed by any of the HMBs, four assessed macronutrients (fat, protein and carbohydrates), one assessed other nutritional factors. Nine did not do any nutritional assessments
- only one HMB recorded fortifying donated milk at the milk bank, and this was on very rare occasions.
A structured semi-quantitative survey
Between July 2021 and November 2022, we conducted a structured semi-quantitative survey with milk bank managers in the UK through phone interviews. The aim of this survey was to investigate in further detail how HMBs were managing the nutritional aspects of donors’ milk. We first contacted the 15 HMBs present in the UK by email; eight agreed to answer the survey.
With regards to nutritional restriction or specific requirements:
- two HMBs confirmed they applied the NICE guidelines, three mentioned they had developed their own questionnaire
- all the HMBs confirmed selecting exclusively smoke and recreational drug-free donors; three requested caffeine-free donors; two requested total alcohol-free donors; four requested donors not to take any medication or were postponing milk collection over the treatment
- two HMBs requested donors to take supplements in case of restricted diets, either vitamin B12 or postnatal multivitamin and mineral supplements
- most HMBs confirmed not classifying the donors in any sort; two did classify the donors depending on whether they had had preterm or full-term babies
- out of the eight HMBs, six said they did not provide any nutritional information to donors; two did ask donors to take supplements, eat healthy fats or asked the donors to compress their breast to get some more fat content in milk
- regarding where they believe there is a need for further research, five HMBs mentioned they wanted more guidance around vegan and vegetarian donors to better understand the implications. One HMB mentioned they had issues with low protein content milk and could not advise donors how to improve. One wanted better understanding of maternal diet on milk organoleptic properties and infant preferences.
Regarding how to make nutritional resources easier to adopt by HMBs:
- two mentioned that having standardised nutritional advice across the country would be helpful
- two mentioned that using easy language, translatable into practice, relevant to donors and cost-free would be critical
- from a donor perspective, four HMBs said that any nutritional information given to donors would have to be carefully communicated so they do not see it as an additional constraint or think their milk is not good enough.
A systematic review
These findings are consistent with a recent online European Milk Bank Association survey to European HMBs exploring practices relating to donors who were following vegan or vegetarian diets.16 The survey identified extremely variable approaches between HMBs, which could result in exclusion of potential donors and nutritional deficiencies. There is therefore a need to develop nutritional resources and guidance for donors, which can be provided through the HMBs. To support the development of these resources we recently undertook a systematic review and narrative synthesis to identify the responsivity of milk nutrient content to changes in maternal nutrient intake.17 In total, 88 articles were included in this review, 54 were experimental studies and 34 were observational, comprising a total of 6,577 participants:
- 29 articles examined fatty acids
- 31 examined vitamins
- 23 examined minerals, amino acids and proteins
- five examined contaminants (heavy metals: arsenic, boron, lead and mercury) and polychlorinated biphenyls (PCBs).
TABLES 1-4 provide a summary of the results along with ratings of the overall quality of the evidence using the GRADE system for each nutrient and contaminant. The tables also summarise the doses of supplementation provided in the experimental studies. Where relevant, European Food Safety Authority (EFSA) recommended intake levels are provided for comparison, as well as toxicity information on contaminant levels.
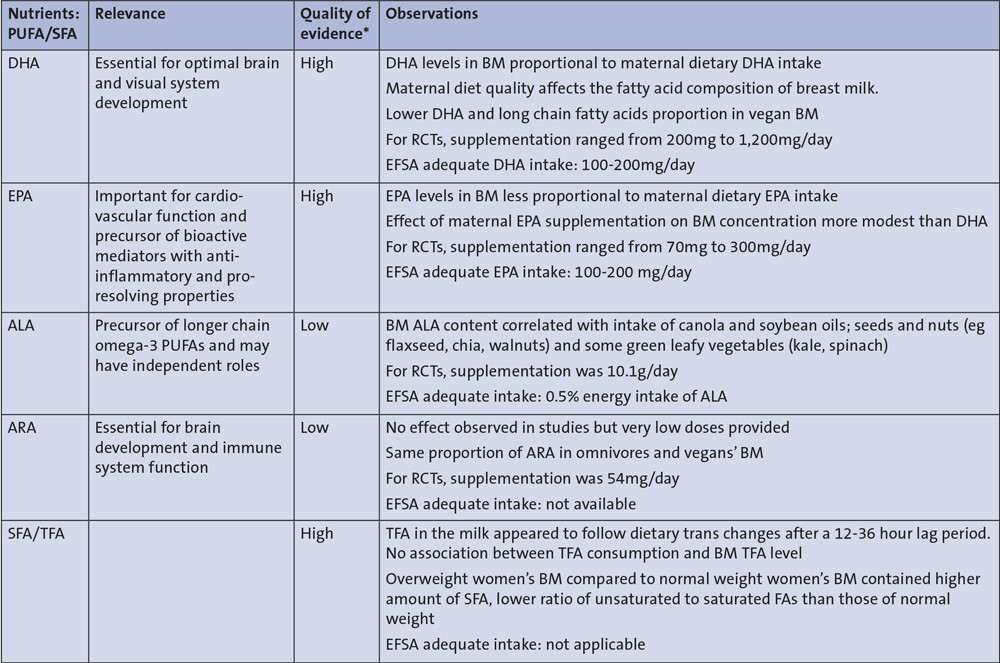
TABLE 1 PUFA/SFA nutrients in breast milk responsive to maternal diet, based on 29 articles (15 experimental studies and 14 observational studies). Key: PUFA= polyunsaturated fatty acids; BM=breast milk; SFA=saturated fatty acids; TFA=trans fatty acids; EFSA=European Food Safety Authority; ALA=ɑ-linolenic acid; ARA=arachidonic acid; DHA=docosahexaenoic acid; EPA=eicosapentaenoic acid; RCT=randomised controlled trial. *Based on GRADE rating system.
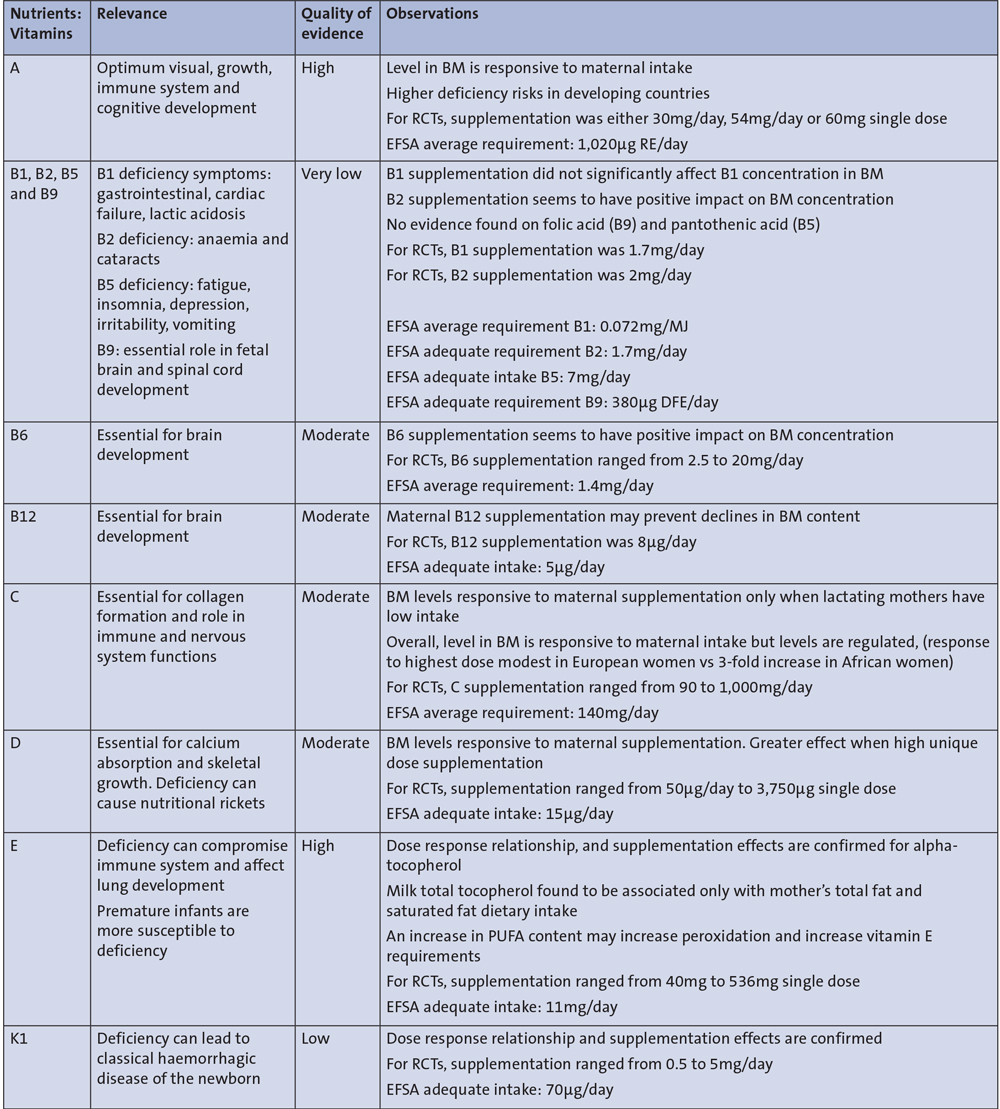
TABLE 2 Vitamins in breast milk responsive to maternal diet (vitamin A based on 8 experimental studies; B vitamins based on 5 experimental and 1 observational study; vitamin C based on 3 experimental studies; vitamin D based on 5 experimental studies; vitamin E based on 5 experimental and 1 observational study; vitamin K1 based on 3 experimental studies). Key: RE=retinol equivalents; DFE=dietary folate equivalent.
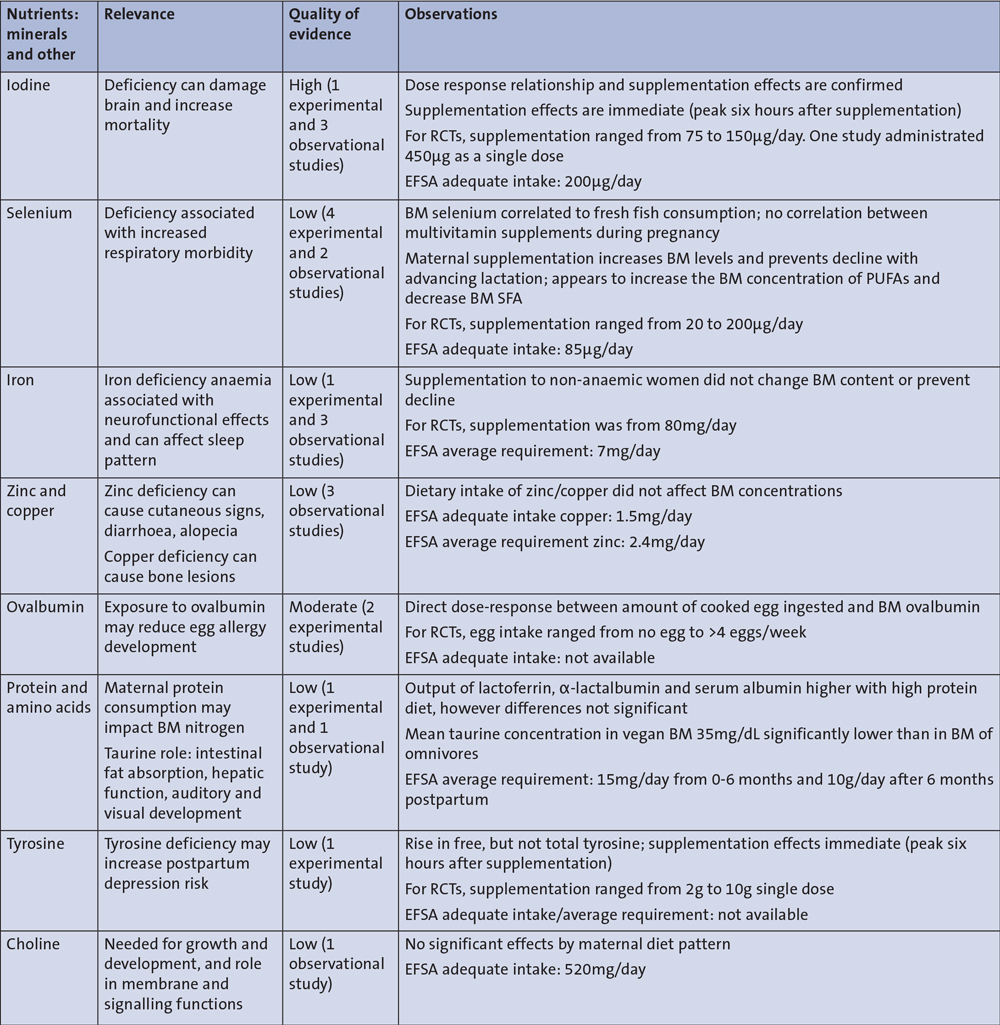
TABLE 3 Minerals (and other) in breast milk responsive to maternal diet.
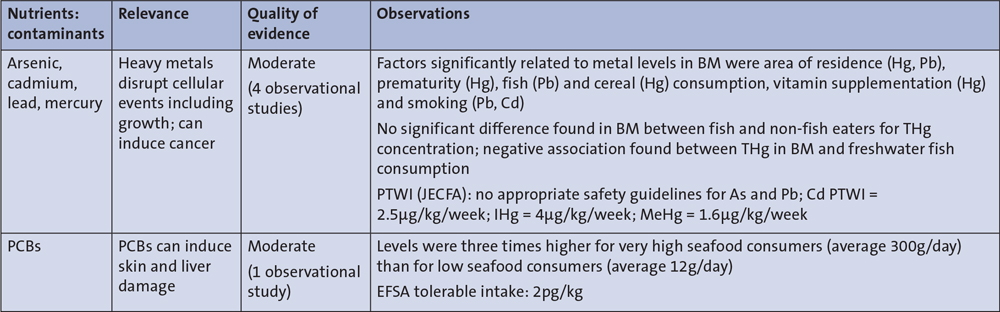
TABLE 4 Contaminants in breast milk responsive to maternal diet. Key: PCBs=polychlorinated biphenyls; As=arsenic; Cd=cadmium; Pb=lead; Hg=mercury; THg=total mercury; IHg=inorganic mercury; MeHg=methylmercury; PTWI=provisional tolerable monthly intake; JECFA=joint FAO/WHO (Food and Agriculture Organization/World Health Organization) Expert Committee on Food Additives.
The main findings are:
- there is strong evidence of response to maternal intakes of DHA, eicosapentaenoic acid (EPA), vitamins A, E and K, iodine and selenium in breast milk composition
- there is some evidence of response for ALA, B vitamins, vitamins C and D, ovalbumin, tyrosine and some contaminants
- there is insufficient evidence to determine the effects of ARA, copper, iron, zinc and choline.
It should be noted that only a high dose of vitamin C was shown to produce an increase in breast milk vitamin C content, and although ARA intake was not found to affect breast milk ARA content, the supplemental dose used was too low to allow definitive conclusions.
Although maternal intake of iron, copper, zinc and total choline levels was not shown to affect their levels in breast milk, these findings are based on a limited number of studies and so there remains uncertainty for these nutrients, consistent with previous systematic reviews.5,18-20
The most researched nutrients were DHA and EPA, where supplementation was consistently shown to increase their respective milk levels and this was in a dose-dependent manner. ALA maternal intake was similarly shown to increase breast milk ALA levels. A significant positive correlation between maternal consumption of fatty fish intake and breast milk DHA, EPA and ALA was also reported. DHA levels were either significantly lower in vegans than omnivores or vegetarians, or low across all groups. For ARA, only one study was identified and in this experimental study participants were supplemented with 54mg ARA per day for two weeks and no relationship was identified between maternal intake and breast milk levels. Trans fatty acids, saturated fatty acids and hydrogenated fats consumption and their content in breast milk were investigated in four studies.
It is important to highlight that in most of the reviewed experimental publications, the nutrient doses were higher than the EFSA adequate intake or average requirements.21 For instance, in all nine reviewed experimental studies, DHA and EPA supplementation was shown to increase breast milk DHA and EPA levels in a dose-dependent manner. The highest dose of DHA provided was 1.2g for 14 days. The levels of supplementation provided were also higher than EFSA recommendations for vitamins A, B6, B12, E and K.21 It may therefore be that dietary supplementation is needed to produce the greatest levels of nutrients.
Vegan and vegetarian diets
When considering specific restrictive diets such a vegan or vegetarian, breast milk from vegan mothers was consistently shown to contain low DHA levels. The choline content was also shown to be lower in breast milk from mothers following a vegan diet. In terms of protein, taurine was lower in vegan mothers’ breast milk. Our review did not identify any studies that specifically compared the vitamin B12 content of breast milk from mothers following vegan, vegetarian and non-vegetarian diets, although vitamin B12 content was shown to be responsive to maternal intake. Therefore, our results support the previous recommendations that mothers following a vegan diet should take supplementation with preformed DHA and vitamin B12, as maternal levels of intake of these nutrients may be low.18 Furthermore, as vegan and vegetarian diets become more popular, there is an urgent need to conduct further high-quality studies in this area, so lactating mothers and milk bank donors can be provided with specific nutritional recommendations. HMBs should identify if donors are following these types of restricted diets.
There is often a concern around the possible negative effects of increasing dietary fish intake, which may theoretically increase the milk levels of contaminants such as heavy metals and PCBs. Our review identified that the number of studies published in this area is limited, with very few publications focusing on dietary sources. However, the overall presence of contaminants in breast milk was below toxicity levels, and based on these observations, fish intake was not identified as a potential source of elevated mercury in breast milk, or as an area of concern with other contaminants.
Conclusion
In conclusion, we have proposed two areas where it may be possible to enhance and/or preserve the nutrient content of DHM. The first area concerns the practices employed by HMBs, looking at storage, transport and processing techniques used, where we have proposed recommendations for practice (protect donor milk from light, minimise storage times, store at the lowest possible temperature).14
The second involves developing nutritional resources for healthcare professionals (such as dietitians and lactation consultants), and for the donors and HMBs. Our systematic review provides the foundation for the development of these nutritional resources. Maternal intake, particularly DHA, EPA, ALA, and vitamins A, D, E, B6, B12 and K, ovalbumin and tyrosine were found to be responsive to maternal diet, whereas there is insufficient evidence to ascertain the effects of intake on breast milk ARA, vitamin C, iron, zinc, copper and choline.17
These results support the recommendation that donors should adopt a healthy and diversified diet, such as the Mediterranean diet, and consider dietary supplementation with nutrients such as DHA, vitamins B12, K and D when their diets are restricted or limited by external factors. Future work will explore how to implement these changes and whether they produce the expected effects on the nutritional content of DHM.
Author contributions
SCD: Conceptualisation, methodology, resources, visualisation, writing - original draft, review and editing, project administration. CF: Data curation, methodology, formal analysis, investigation, resources, writing – original draft, review and editing. YJ: Resources, writing – review and editing.
All data are available upon request from the corresponding author.
Or read this article in our
Tablet/iPad edition
- Current milk banking practices (eg storage, freeze-thawing, processing) negatively affect the nutritional quality of DHM. We provide recommendations to mitigate some of these effects.
- Milk banks do not currently provide specific dietary advice for donors. We highlight how donor diet influences the nutritional content of DHM and provide recommendations for donor nutrient intake.
- Through a combination of these approaches, it may be possible to enhance the endogenous nutrient levels of DHM to better support the needs of extremely and very preterm infants.
Also published in Infant:
