

Response of UK milk banks to ensure the safety and supply of donor human milk in the COVID-19 pandemic and beyond
The COVID-19 pandemic is presenting several challenges to human milk banks and has highlighted a number of vulnerabilities in service provision that have been long known by those who work in the sector. In recent weeks, milk banks across the UK have worked together to understand any risks posed to infants, milk bank staff and volunteers by COVID-19, and to put in place mitigation strategies to ensure the safeguarded provision and safety of donor human milk. The authors call on policymakers to better support these essential services for vulnerable neonates during the COVID-19 pandemic and minimise the impact of future challenges through greater investment in milk bank infrastructure, research and innovation.
Natalie Shenker1,2
natalie.shenker09@imperial.ac.uk
Jackie Hughes3,4
Debbie Barnett5
Gillian Weaver2
1Department of Surgery and Cancer, Imperial College London
2Human Milk Foundation, Rothamsted Institute, Hertfordshire
3Chair of Trustees, UK Association for Milk Banking, Chester
4Strategy Manager, North West Milk Bank
5Chair of the UKAMB Forum, Manager for the Scottish Milk Bank Service, Glasgow
If mother’s own milk (MOM) is not available for low birth weight or other-wise vulnerable infants, donor human milk (DHM) from a human milk bank (HMB) is recommended as the first alternative.1-6
In February 2020, the World Health Organization (WHO) issued specific advice for breastfeeding during the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; COVID-19) outbreak stating that women who become too unwell to breastfeed or express should have the option of DHM, depending on the cultural context and availability, with the option of re-lactation support for women when they recover.7
The UK’s HMBs
It is estimated that more than 800,000 babies annually receive donor milk in the 66 countries with active milk banks,8 including up to 6,000 in the UK. There are currently 14 active HMBs operating in the UK. Scotland has a single national service located in Glasgow that supports all 15 neonatal units (NNUs) in the country. Northern Ireland’s HMB provides milk to NNUs north and south of the border, making it a unique part of the health service. England has 12 HMBs ranging in size – two produce over 2,000 litres each year and support several NNUs (North West and Hearts), while some support only their own Trust’s NNU. There are currently no milk banks in Wales.
DHM provision
The primary role of HMBs is to protect, promote, and support breastfeeding. With appropriate use in the context of optimal support for lactation, a short period of DHM provision can support mothers to establish their milk supply without the need for supplementation with infant formula milk.
DHM is used primarily for premature and low birthweight babies being cared for in a hospital NNU; each unit has its own protocol. Several UK HMBs also supply DHM to families who meet specific clinical criteria in the community if surplus DHM is available. These include families where breastfeeding is not possible as a result of maternal ill-health (eg maternal cancer, anti-psychotic medication use) or maternal absence (eg death, fostering, adoption).
The COVID-19 response
The COVID-19 pandemic brings additional considerations and challenges for the mother-infant dyad, newborn nutrition and HMB operations. Increased separation of mothers and infants limiting access to maternal milk (as is happening in some settings despite WHO guidance),7 together with reduced availability of DHM could lead to an increase in morbidity and mortality related to prematurity and other health conditions.9-11
The potential for increased demand from NNUs raises questions as to which clinical situations should be prioritised, and the capacity of HMB infrastructures to respond. During this critical COVID-19 response period, UK HMBs are facing challenges in terms of maintaining adequate staffing, donor recruitment, safe handling/transportation of DHM, and increased demand. It is essential that systems that provide DHM for vulnerable infants are not inadvertently impacted by efforts to contain COVID-19.
As the COVID-19 pandemic has developed, some individual milk banks initially published their own guidance for the recruitment of donors. The first advice by the Hearts Milk Bank to donors was published online on 23 January 2020, under the guidance of Dr Jim Gray, Clinical Microbiologist and Lead Advisor for Screening. In the absence of global safety standards, HMB associations and individual HMB programmes have since developed their own specific guidance relating to DHM in the context of COVID-19.12,13 Additionally, the Human Milk Foundation has been instrumental in supporting the creation of a Global Alliance of Milk Banks and Associations, which will facilitate the development of globally appropriate minimum standards and regulatory recommendations.8
A virtual communication network for UK HMBs
On 16 March 2020, the Hearts Milk Bank initiated a virtual communication network (VCN) via WhatsApp for UK milk bank leads, which has rapidly facilitated the sharing of information, discussion of evidence, and development of consensus views of best practice related to local circumstances. The group now includes over 19 members from 12 of the UK milk banks. Furthermore, the authors developed a ‘preparedness tool’ that aimed to ensure milk banks had recognised potential challenges that may occur throughout the course of the COVID-19 pandemic. Critically, it asked group members to consider which milk banks would have sufficient capacity and suitable geographical location to maintain a continuous provision of donor milk to hospital NNUs in the event of staff shortages or other issue causing the temporary closure or cessation of pasteurisation within a milk bank (TABLE 1). Further collation of data, such as that reported in the preparedness tool, can highlight trends such as the efficiency of larger milk banks. This type of data collection, preparedness and facilitation of communication will be instrumental in supporting the development of a future national milk bank service.
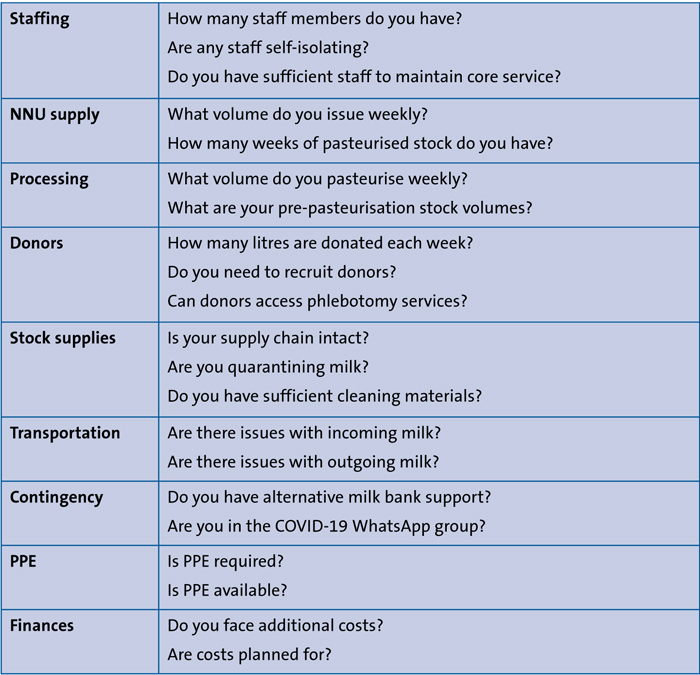
TABLE 1 Some of the questions addressed by the preparedness tool to assess UK milk banking during the COVID-19 pandemic. Key: PPE=personal protective equipment.
Challenges and mitigation strategies
In recent weeks, milk banks have worked together to understand the risk posed to infants, milk bank staff and volunteers by COVID-19. By group consensus a number of mitigation strategies have been put in place to overcome the challenges and ensure safe provision of DHM (TABLE 2).
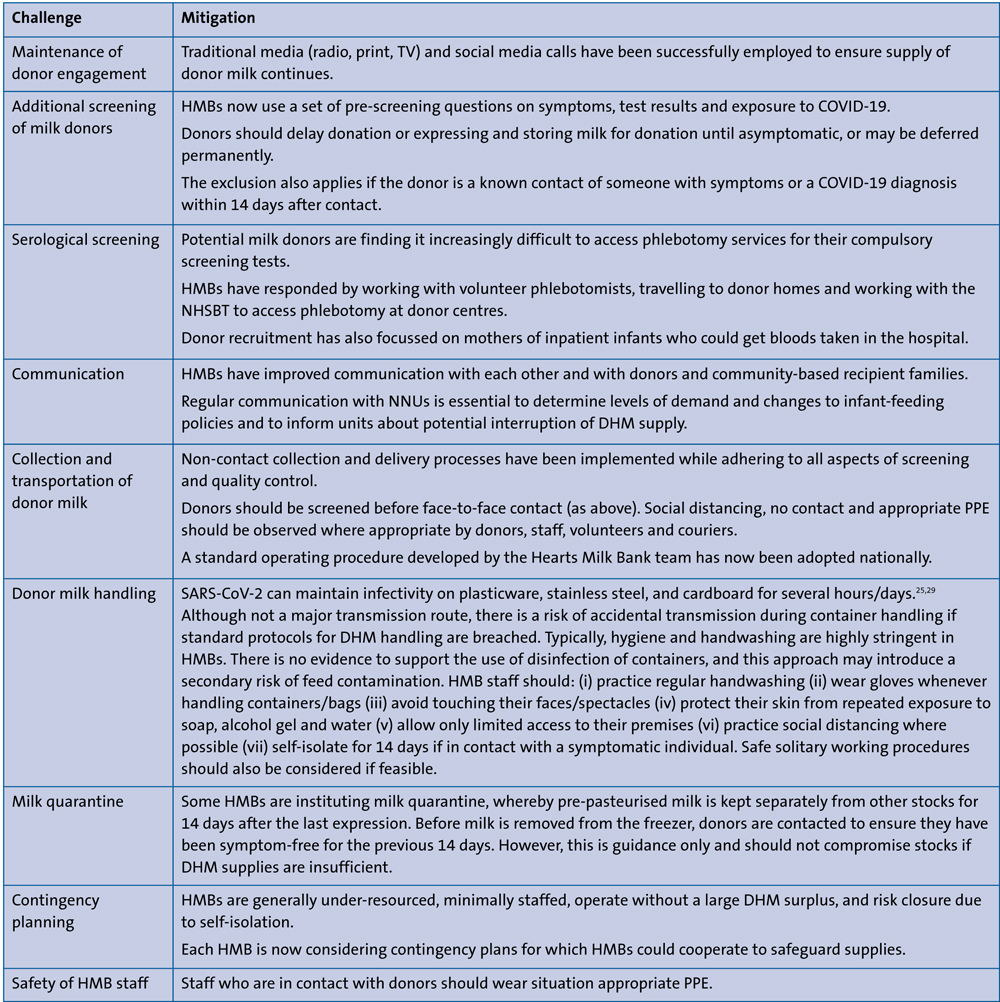
TABLE 2 Challenges and mitigations for the continuation of DHM provision. Key: NHSBT= NHS Blood and Transplant.
Ensuring safety between mother and infant during suspected or confirmed COVID-19 infection is complex and has resulted in mixed messages and confusion. Currently, global policy leaders now agree that mothers and infants should remain together and safe breastfeeding and access to human milk should be supported. The virtual group unanimously supports the WHO’s recommendations not to separate the mother and infant and to support breastfeeding, thereby decreasing the demand for DHM and improving outcomes for the mother and her infant. However, in the context of separation of a symptomatic mother and infant, DHM use may be a critical bridge for the infant, assuming that systems will simultaneously provide lactation support to ensure the mother can initiate and maintain lactation during separation.
Reduced access to MOM through reduced availability of face-to-face breastfeeding support and, in some areas, problems with the supply of infant formula, initially led to increased demand for DHM from hospitals as well as from families in the community. Increased demand placed further pressure on DHM supply and current HMB infrastructure, particularly in March during the earliest phase of the pandemic when there was greater uncertainty about the continuation of transportation and other logistics.
The consensus from the VCN is that a comprehensive approach should be implemented to maintain contact between mothers and babies, with skin-to-skin and breastfeeding support. If DHM is provided during separation, this should be for as short a time as possible as a bridge to receiving MOM. This approach increases the chances that these infants will leave the NNU exclusively breastfeeding, which is critical for the longer-term health of mother and baby.
SARS-CoV-2 transmission through human milk
Based on best available evidence, there is a high probability that SARS-CoV-2 is not transmitted through human milk. Viral transmission through breast milk has been described for a range of viruses, including HIV and cytomegalovirus.4,15 Coronaviruses (CoV) are enveloped, single-stranded RNA viruses that are primarily spread via droplet and contact transmission. CoVs have not been detected in breast milk, and transmission of CoVs via breast milk has not been reported, although it is likely that mothers could infect infants via the respiratory route while breastfeeding.16
No peer-reviewed published studies have found the presence of SARS-CoV-2 in milk samples from COVID-19 positive mothers. It is highly unusual for a CoV or other respiratory virus to cross into breast milk.17 Neither direct breastfeeding nor feeding of expressed human milk has been shown to be a route to vertical transmission. For the limited data available, where breast milk has been analysed from mothers infected in the third trimester of pregnancy, evidence of viral particles in samples of expressed milk is lacking (though little information has been given regarding sample collection).18
To date, vertical transmission has been reported in utero in two infants, with IgM and IgG antibodies present two hours after birth,19 and in one single infant at three months of age exposed to their COVID-19 positive grandmother.20 Typically, serum antibodies appear several days after symptom development, with specific IgM antibodies appearing at 10 days and IgG antibodies developing by 14 days.21 Profiling of human milk for IgG or IgM antibodies against SARS-CoV-2 is ongoing in several centres worldwide, and in the UK the Hearts Milk Bank, established among other reasons to facilitate wide-ranging research into human milk composition, is now actively recruiting mothers who have recovered from COVID-19 as part of an Imperial College-led research study that seeks to determine the presence and functionality of anti-SARS-CoV-2 antibodies. Batches of donor milk with antibodies could be clinically useful in the care of infants of symptomatic mothers unable to express their own milk.
The persistence of antibodies after SARS-CoV-2 infection is not known. A case report from the SARS outbreak in 2003 showed that a pregnant woman infected at seven days of gestation was antibody-positive at 28 days and 64 days post-illness, and at birth at 36 weeks, but milk samples were negative for SARS-CoV antibodies. Another woman who developed symptoms at 19 weeks of gestation and delivered at 36 weeks had SARS-CoV antibodies detected in serum, umbilical-cord blood, and breast milk by enzyme immunoassays and indirect immunofluorescence assays 130 days after infection.22-24 Research is urgently needed to understand true viral presence in breast milk across gestation and lactation during COVID-19 infection in order to inform guidelines for infant feeding worldwide for the general population, as well as hospital settings.
HMB practices to mitigate the risk of SARS-CoV-2 transmission
Practices that are common to HMB services are likely to mitigate the risk of SARS-CoV-2 transmission. HMB services operate according to guidelines set by national bodies or local organisations. Donors are screened using interviews and questionnaires based on health and life-style. These aim to reduce the risk of microbial or other contamination of donated milk and are usually employed in addition to serological screening for common blood-borne infections. Human milk is collected and pasteurised via Holder pasteurisation (milk heated to 62.5°C for 30 min). Recent work has shown that SARS-CoV-2 is inactivated by heating in a dose-dependent manner, with viral inactivation at 10-30 min at 56°C, or 5 min at 70°C,25 although no specific studies have yet investigated viral inactivation in human milk under Holder pasteurisation conditions. Research on similar corona-viruses, SARS-CoV and MERS-CoV has shown complete heat inactivation by treatment at 60°C for 15-30 min.26-28
Conclusions
Many milk banks initially struggled to respond to the COVID-19 pandemic, with issues deepened by the lack of agreed safety guidelines on HMBs, no mechanism for rapid communications among HMBs, and limited data gathering and infrastructure to ensure responsiveness during a crisis. With increased communication and strategic planning, the system has already strengthened.
Milk banks offer a unique opportunity to support research into human milk, and a number of studies have started during the course of the pandemic. Other work is starting in terms of disaster-preparedness, including the provision of freeze-dried milk that can offer longer storage durations and simplified postal delivery, without the need for couriering. Further investment is required into innovation, research, training and infrastructure to ensure that provision of safe DHM remains an essential component of routine early newborn care, as well as emergency situations.
Or read this article in our
Tablet/iPad edition
- This article outlines the challenges facing provision of DHM during the COVID-19 pandemic.
- Mitigation strategies to ensure safety and provision of DHM have been developed by group consensus.
- There is a high probability that SARS-CoV-2 is not transmitted through human milk – the latest data are reported.
Also published in Infant:
