

Management of lactation following the death of a baby
The death of an infant is a profound, emotionally complex time in a new mother’s life. She grieves for the baby she has lost, the life she imagined and her role as a mother. Compounding this emotional distress is the physical pain associated with engorgement and milk secretion. This article discusses the physiology of lactation and practical advice to give to bereaved mothers to help them through this time. Ways to suppress lactation are discussed as well as the concept that continuation may be the right pathway for some mothers.
Abby ParishMB BCh, MRCPCH
Neonatal GRID Trainee
abbyjaneparish@doctors.org.uk
Cora Doherty
MB BCh, BAO, MD, DCH, FRCPCH, FRCPI
Consultant Neonatologist
University Hospital of Wales, Cardiff
The death of a baby and subsequent grief is complex. In addition to grieving for their baby’s life, parents grieve for the loss of the life they had imagined with their child alongside grieving at the loss of the roles they expected to play as parents. For new mothers, the emotional pain they experience may be compounded by physical pain related to continued lactation when there is no longer a need to provide nutrition for a baby. In our experience, guidance for advising mothers regarding cessation of lactation following bereavement is not always readily available in the neonatal unit or hospice setting. With multiple tasks needing completion alongside support provision for the family and team members, speaking to a grieving mother about lactation is often overlooked despite the considerable effect this has on her emotional and physical wellbeing.
Providing education and guidance for teams on cessation of lactation is important and is underpinned by knowledge of the physiology of lactation. The aim of this article is to review lactation physiology and to utilise this knowledge to guide support for mothers and their partners to make the best choices to suit their individual circumstances. This includes options around both cessation and continuation of lactation following the death of a baby.
Physiology of lactation
Understanding the physiology of lactation is important for enabling healthcare staff to help women establish breastfeeding and also to support bereaved mothers.
Mammary glands are organised in lobes containing alveoli, blood vessels and lactiferous ducts. During pregnancy, the high progesterone to oestrogen ratio causes significant hypertrophy of the breast tissue (mammogenesis). The alveolar cells are capable of milk production from mid-gestation; this is lactogenesis I or secretory initiation. However, milk secretion is inhibited by high circulating levels of progesterone and oestrogen.
When the placenta is delivered, serum progesterone levels decrease suddenly. The abrupt withdrawal of progesterone in the presence of raised circulating prolactin initiates lactogenesis II (secretory activation) and milk production occurs 30-40 hours after birth.1 This phase of lactation is hormonally driven and milk removal is not needed for initiation of lactogenesis II. After lactogenesis II there is a switch from endocrine control to autocrine control, with milk removal acting as the stimulus for milk synthesis; this is lactogenesis III.
When an infant suckles at the breast, there is contraction of myoepithelial cells and feedback to the hypothalamus via the afferent pathway to stimulate oxytocin release from the posterior pituitary gland (FIGURE 1).
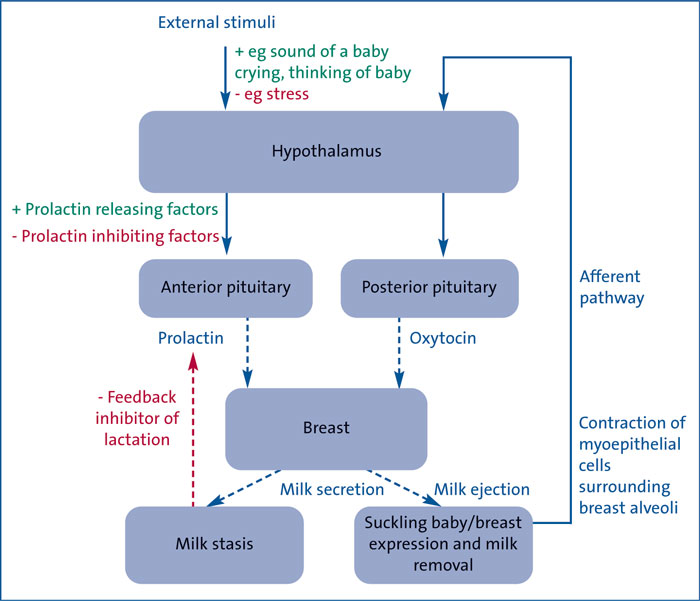
FIGURE 1 Hypothalamic feedback loops during lactation. Prolactin stimulates milk synthesis within the breast. Oxytocin stimulates contraction of myoepithelial cells causing milk to be ejected into the milk ducts. When the breast is stimulated prolactin levels in the blood rise, which triggers the breast cells to make milk. When an infant suckles at the breast, there is contraction of myoepithelial cells and feedback to the hypothalamus to stimulate oxytocin release from the posterior pituitary gland. The positive feedback loop ensures continued milk production as long as the infant continues to breastfeed. If milk is not removed, feedback inhibitor of lactation accumulates and inhibits milk production via a negative feedback loop.
However, if the breasts are not stimulated to produce milk after birth – if the mother chooses not to breastfeed or if feeding/expression has not taken place because the baby died shortly after delivery or was stillborn – a build-up of milk in the breasts distends the alveoli and leads to accumulation in the mammary glands of a protein called feedback inhibitor of lactation (FIL). This reduces capillary blood flow and causes involution of the milk secreting glands, downregulating milk production through a negative feedback loop.2 This process can take a number of weeks to resolve and the engorgement can be uncomfortable. Painful engorgement can occur and one of the aims of suppressing lactation is to avoid this.
White tears
Grieving mothers often experience a distressing physical consequence following the loss of a baby; the milk referred to as ‘white tears’.3 This is a descriptive term demonstrating the emotional weight of this physiological phenomenon. The milk produced is inextricably linked with the mother’s grief. The continuing bonds theory of grief proposes that grief is a fluid concept and that rather than the bereaved moving on from their grief, instead the memory of the deceased continues through their life and is incorporated into the ongoing narrative of their life.4 The bereaved often look for ways to maintain bonds that have been broken by their bereavement. The ongoing production of milk is a very real reminder of the loss they have experienced and for some mothers it may represent a continuing bond as the mother moves along her bereavement journey.
Lactation suppression
Lactation suppression is a choice for the bereaved mother to make. Some women may want to suppress the milk that reminds them of their loss; others may wish to continue to express milk as suppression is not their preferred journey. These choices should be discussed openly and supported.
The stage of lactogenesis in bereaved women will vary depending on whether the baby died shortly following delivery or whether the mother had already established breastfeeding. If the infant was stillborn or died shortly after delivery and the mother’s breasts were not stimulated by a suckling baby or expression, she would be at lactogenesis II. If the infant died later and/or breast milk expression/breastfeeding had already taken place, the process of lactation is under autocrine control with breast milk removal stimulating further production (lactogenesis III).
When an infant has been breastfeeding before its death and/or admitted to a neonatal unit following delivery, the mother may have been successfully breastfeeding and/or regularly expressing; she may have an established milk supply. Suppression of lactation in such cases is different to those who have not breastfed or expressed breast milk and suppression is more likely to be protracted.
Various pharmacologic and non-pharmacologic interventions have been used to suppress lactation following birth and these will be discussed in the following sections.
Non-pharmacological methods
Historically, many non-pharmacological approaches to lactation suppression have been recommended, the majority of which make little difference and have no beneficial effect, These include breast binding,5 the use of ice, fluid restriction and forced fluids.6 During such a stressful and emotional time, giving poor advice can complicate the situation.
There is some weak evidence that homeopathy7 and acupuncture8 may have a beneficial effect although there is not sufficient evidence to justify recommendation.9 Sleeping in a supine position may take pressure off the breasts to aid a more restful sleep; pillows can be used to support the breasts if side lying. Some ‘traditional’ treatments, such as cabbage leaves, may help although this may be due to the gentle massage that is involved rather than the treatment per se.10,11 Similarly gel packs and therapeutic ultrasound have shown benefit by the same suspected mechanism.10,11
It is worth noting that although the evidence shows breast binding is not an effective intervention, it is the cultural norm in some areas9 and one study found mothers reported the process as positive as it gives rise to conversation about grief and a physical reminder of the loss as being real.12 If mothers choose to perform breast binding, they should be supported to do so, however, there is an increased risk of mastitis and mothers should be warned to be vigilant to this.9
Gradual reduction in expressing is preferred
It is important to explain to the mother that breast engorgement and subsequent negative feedback mechanisms work to suppress lactation. The aim when suppressing lactation is to avoid painful engorgement. For women with an established milk supply, abrupt withdrawal is not advised as it can lead to severe engorgement and intense pain.6 There are different reported methods of pumping designed to reduce the production of breast milk. Essentially the frequency and duration of pumping will vary depending upon multiple factors, eg how much milk a woman produces.6 She should continue to express using a good quality breast pump and one should be supplied, unless she is experienced in manual expression.13 Removing just enough milk to reduce the discomfort, but not emptying the breast will gradually reduce lactation.6,14 The plan, therefore, is a fluid process that is discussed between the multidisciplinary team and the mother. Some mothers will appreciate a plan that is simply responsive to her symptoms; for example, express when your breasts are very uncomfortable and stop before they are fully empty with the aim of increasing the interval between and reducing the duration of expression. This would give the mother some control of the situation in a time where she is likely to feel like she has none.15 If the mother has an established schedule for expressing, she may prefer to have a timetable to follow to reduce her supply. Some examples include:
- drop one session per day and alter the interval between sessions accordingly14,15
- reduce the time of each expression by five minutes every day.
When undertaking steps to gradually wean breast milk supply, engorgement and milk trapping can occur. Plugged ducts or trapping would be described as a tender spot or lump in the breast. Suitable advice to give would include massaging before, during and after pumping to assist with removal and stroking towards the nipple to encourage milk to flow.16 Heat applied prior to expressing may be of aid.14 Mothers should be advised that if things worsen by becoming larger, hardening and involving the entire breast, then this is engorgement and unaddressed this will lead to mastitis. Mastitis presents as sore, engorged breasts that are erythematous and warm to touch. Flu-like symptoms such as fever, chills and myalgia may be present.14 Women with mastitis should be referred to their own physician for treatment. It is important to inform mothers that leaking milk may be experienced for weeks to months after lactation is suppressed.14Advice that could be given to mothers is summarised in FIGURE 2.
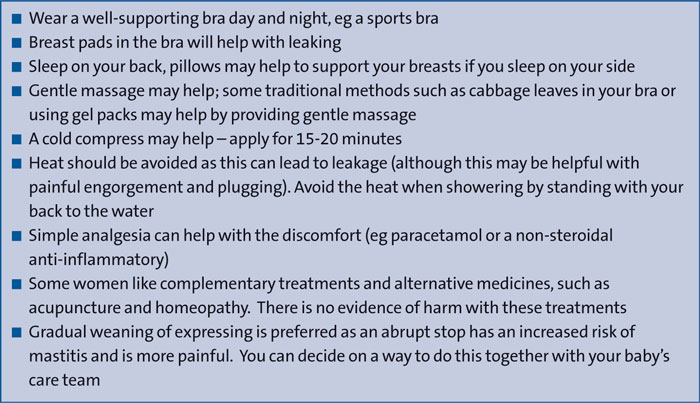
FIGURE 2 Advice to give to bereaved mothers who are undergoing suppression of lactation.
Pharmacological methods
Historically, many medications have been purported to induce or aid lactation suppression. Some, including oestrogen, testosterone and bromocriptine,9 are no longer used due to cardiovascular side effects.17-19 Cabergoline is a stimulant of dopamine receptors in the brain that inhi-bits the release of prolactin by the pituitary. It has been used to treat hyperprolactinaemia, has been shown to successfully suppress lactation in a high proportion of women and is well tolerated.20 Dopamine agonists are recommended by the Royal College of Obstetrics and Gynaecology for lactation suppression for women who experience a stillbirth21 and cabergoline is simpler to use and has less adverse effects than bromocriptine.20 Cabergoline has two treatment regimes, depending upon whether the mother is within the first 24 hours of delivery or beyond.22 FIGURE 3 gives the treatment regime and other pharmacological information. This medication is not without potential side effects and mothers must be counselled accordingly prior to its prescription.
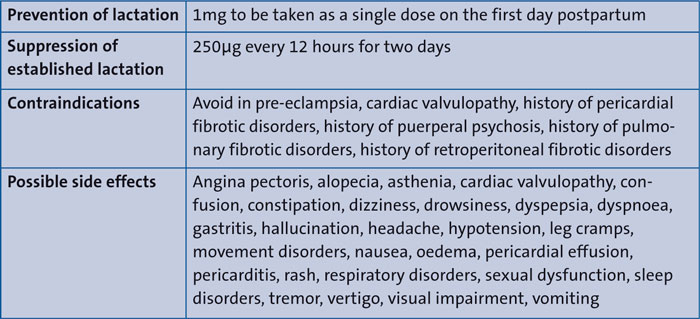
FIGURE 3 Cabergoline: prescription regime, contraindications and side effects.22
Lactation continuation and memory making
For neonates who are in the end stages of their life, a mother’s expressed breast milk can be used for oral mouth cares and she may put some milk on the baby’s lips.14 As a symbolic act, this may bring comfort for the mother and help to connect the mother with her baby. Some dying babies may be able to suckle at the breast and again this option could be offered to the mother, if appropriate.6
A reminder that lactation suppression is a choice for bereaved mothers. Some mothers will choose to express as part of gradual weaning to suppress lactation. Other mothers may want to initiate or continue lactation as part of the narrative around their baby’s death. They may choose to continue to express milk in the longer term after their baby has died. The sharing of maternal milk is steeped in history with cross feeding and wet nursing.23 The first formal milk bank was opened in Vienna in 190924 and now there are over 600 milk banks operating in over 60 countries25 – non-profit organisations that collect, pasteurise and distribute donor expressed breast milk to those who need it (FIGURE 4). Milk is donated for many reasons, one of which will be bereavement.

FIGURE 4 Pasteurised donor breast milk. Bereaved mothers may like to continue to express and donate their breast milk.
Many others are comforted knowing the milk they have produced can help a baby in need;26 taking comfort in the ‘legacy’ left by their child.23 Welborn explored the experience of 21 bereaved mothers who chose to continue to express and donate their breast milk.27 The data revealed four themes, the first of which was that it allowed the mothers to identify themselves as a mother – a way to feel like a mother in the absence of their baby. Expressing milk gave mothers a sense of meaning associated with the act, a physical connec-tion with their baby and a way of acknow-ledging the baby’s life. The third theme centred on finding meaning in the perinatal loss; the act of donating milk for other infants gave mothers a deeper meaning beyond the intense grief, allowing other infants to benefit in honour of their baby, bringing comfort to the mother. The fourth theme concerned the support that mothers received regarding lactation after their bereavement, with many feeling that they did not receive enough support and that the option to donate milk should be more accessible. All 21 mothers inter-viewed in this study reported positive emotions regarding their experience of donating milk, thus it is an option that should be sensitively offered and compassionately supported if this option feels right to the mother.
If a mother has expressed milk prior to death, after death or as part of lactation suppression, they are likely to have a supply of frozen or refrigerated expressed breast milk. Milk can be donated formally though milk banks and the UK has 14 of these, information can be found via the UK Association for Milk Banking (UKAMB), a charitable organisation that supports milk donation and milk banks.28 It would be best practice to contact the milk bank prior to discussing this option with a mother as there are eligibility criteria and at times banks are unable to accept donations. This would avoid further upset by suggesting it as an option and then giving the mother a sense of failure or disappointment if she was unable to donate.15,26 Donation to a milk bank is the safest way to donate milk but it is worth noting that there are other informal ways to donate milk in the local community.9
For women who have milk stored but are unable to donate, advise them to discard the milk with the general waste. Some women will wish to keep a container of milk as a memento.14 Women can be advised that there are also companies that turn breast milk into mementos for a fee, such as beads or pendants.
Summary
The loss of a baby is a profound experience for parents associated with complex grief. Mothers who are breastfeeding not only have to deal with losing the bond associated with breastfeeding but also have to cope with the physical effects of the acute cessation of lactation. This can be an additional challenge which may be overlooked in some instances and may lead to discomfort, pain, further feelings of loss and confusion for mothers about how to manage both breast milk expression and any milk they have already stored. Understanding lactation science is essential in order to best help mothers during this difficult time and this article outlines the physiology of breastfeeding and reviews non-pharmacological and pharmacological methods purported to aid lactation suppression. Furthermore, the roles of lactation continuation and donation, and memory making with expressed breast milk are examined.
Or read this article in our
Tablet/iPad edition
- Bereaved mothers who were breastfeeding have to cope with the physical effects of acute cessation of lactation while grieving for the loss of their baby.
- Understanding lactation science is essential in order to best help mothers during this difficult time.
- Non-pharmacological and pharmacological methods to aid lactation suppression are reviewed alongside the role of lactation continuation and donation of expressed breast milk.
