

Are babies with congenital heart disease born in the right place at the right time? Practice in a cardiac network
Antenatal diagnosis of congenital heart disease (CHD) and subsequent delivery of higher risk cases in the tertiary centre improves perioperative conditions and neurodevelopmental outcomes in neonates with CHD. In October 2021, the Yorkshire and Humber Congenital Heart Disease Network developed a guideline with the objective of providing guidance on the timing and location of delivery for babies with antenatal diagnosis of CHD. Our project aimed to assess compliance with the guideline and evaluate the extent of improvement in delivery practices that have been implemented in accordance with the guideline.
Muhammad Rehan AkhtarPaediatric ST5, Leadership Fellow, Y&HCHD Network, Leeds Teaching Hospitals
muhammad.akhtar3@nhs.net
Lawrence Miall
Neonatal Consultant, Neonatal Co-Lead for Y&HCHD Network, Leeds Teaching Hospitals
Fiona Willcoxson
Paediatric Cardiology Lead Clinician, Y&HCHD Network
Alison Conchie
Manager, Y&HCHD Network
Yorkshire and Humber Congenital Heart Disease (Y&HCHD) Network
Akhtar M.R., Miall L., Willcoxson F., Conchie A. Are babies with congenital heart disease born in the right place at the right time? Practice in a cardiac network. Infant 2024; 20(3): 94-98.
Background
Congenital heart disease (CHD) is the most prevalent type of congenital malformation, impacting around eight out of every 1,000 live births.1 Advances in ultrasonographic technologies and meticulous antenatal screening have significantly improved prenatal detection of CHD with overall, about 60% of lesions detected antenatally and up to 90% of hypoplastic left heart syndrome diagnosed antenatally.2 This leads to scheduled deliveries in tertiary centres equipped with specialised neonatal and cardiac care.3 In addition, antenatal detection of CHD is associated with:
- improved pre-operative survival rates4
- a decreased incidence of pre-operative brain injury5
- better neurodevelopmental outcomes in infants with critical CHD.6
Consequently, the choice of the delivery location becomes crucial when devising the perinatal management plan and it is important to recognise the lesions that may necessitate urgent postnatal intervention making delivery at a tertiary centre beneficial,7 particularly:
- duct-dependant lesions
- single ventricle lesions
- transposition of the great arteries
- total anomalous pulmonary venous connections (TAPVC).
The time of delivery is also of prime importance to achieve favourable neonatal outcomes. The adverse outcomes associated with late preterm (34+0 to 36+6) and early-term (37+0 to 38+6) deliveries are well documented in the literature.8,9 Late preterm babies experience approximately 4.5 times higher mortality due to congenital anomalies, which remain the leading cause of infant death, compared to term babies.10 Studies recommend delaying elective caesarean sections to at least 39 weeks to prevent complications of deliveries associated with deliveries at 37-38 weeks by 25% to 50%.11,12 A retrospective review of the time of delivery for babies with CHD demonstrated significantly increased mortality (2.5 times) and morbidity (1.2 times) in the neonates born at 37 and 38 weeks compared to those born at 39 and 40 weeks.13 It is strongly justified to plan deliveries for babies with CHD not before 39 weeks. In specific cases, such as transposition of the great arteries and hypoplastic left heart syndrome, it is unclear if delaying the delivery any further than 39 weeks comes at a neurological advantage.14 Of course this desire to improve outcomes by delivery as close to term as possible, has to be balanced against an increasing risk of spontaneous preterm labour in the local non-cardiac hospital as the pregnancy approaches 40 weeks’ gestation.
The Yorkshire and Humber congenital heart disease (Y&HCHD) network comprises 20 hospitals across the region and covers a population of 5.6 million people with approximately 60,000 births.15 Leeds Children’s Hospital is the tertiary paediatric cardiology centre in the network with the co-located tertiary neonatal unit. Outside the tertiary centre, paediatricians with expertise in cardiology (PECs) provide local outpatient care to children with CHD and their families.
Approximately 200 children are born with critical CHD requiring intervention each year in the Y&HCHD network, with approximately 50% of cases being diagnosed antenatally.16 Following a significant incident where a mother whose baby was antenatally diagnosed with transposition of the great arteries, delivered in the local non-cardiac referral hospital, the Y&HCHD network developed and disseminated a guideline in 2021 to reinforce guidance on the optimal place of delivery of babies with antenatal diagnosis of CHD and desired gestation at birth.
Aim
We conducted a review to assess the delivery practices of babies with known CHD in Yorkshire and Humber before and after implementing the Place of Delivery Guideline. Our aim was to evaluate the extent of improvement that occurred following the guideline's implementation.
Summary of the guideline
The Place of Delivery Guideline, published in October 2021 (www.networks.nhs.uk/groups/yorkshire-humber-congenital-heart-disease-operational-delivery-network), is aimed to ensure the delivery of babies with suspected or confirmed CHD at the most appropriate setting for optimal management while keeping the families close to their homes. This guidance was shared with the neonatal and maternity networks, the cardiology centre and the regional neonatal transport team. It emphasises that planned deliveries should not occur before 39+0 weeks’ gestation while acknowledging that certain maternal and fetal factors may necessitate delivery before this time. Exact timing is agreed at a weekly fetal medicine/cardiology multidisciplinary team meeting.
The guideline implements a traffic light system to indicate the appropriate delivery destination for different cases (FIGURE 1). Red lesions require delivery in a tertiary cardiac centre; amber lesions are subject to case-by-case discussions and may be delivered locally; green denotes expected local birth, and purple is designated for planned palliation.

FIGURE 1 The traffic light system to indicate appropriate delivery destination.
Methods
We conducted a retrospective audit analysing data for infants born between May 2021 and April 2022, specifically examining a period of six months before and six months after the guideline publication. This review was carried out in the cardiac centre using electronic patient records (PPM+ and BadgerNet) with additional local data provided by the local PECs.
Results
During the 12-month review period, a total of 216 pregnant women were referred to fetal cardiology. Among these referrals, 38% occurred in the first half of the study period (May to October 2021, before the guideline was published and 62% in the second six months November 2021 to April 2022). It is unclear why there was such a marked difference, although detection of CHD is known to have slightly decreased during the COVID-19 pandemic.16 Of the 216 women, 23% did not progress to a live birth (due to termination of pregnancy, intrauterine death or stillbirth), leaving 166 cases of live-born infants. The booking hospitals for all live births are depicted by the level of their associated neonatal units in FIGURE 2.
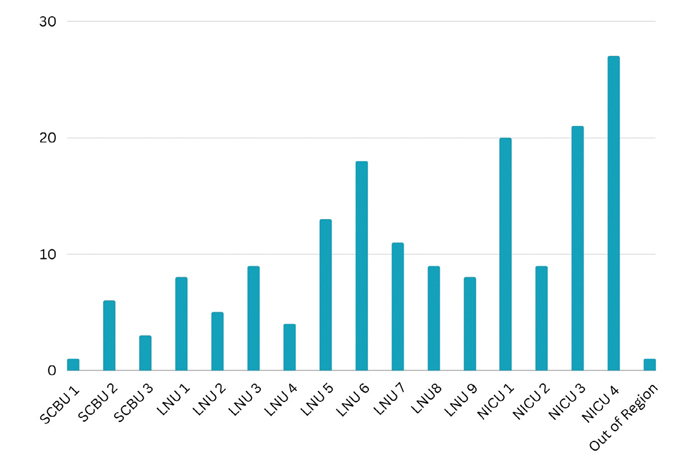
FIGURE 2 Booking hospitals of all live births represented by their associated neonatal units.
Pre-guideline period
Out of 82 referrals made to fetal cardiology in the first six months of the study period before the guideline was published, 60 (73%) resulted in live births. Among these live births:
- 30 (50%) were deemed suitable for delivery in the local hospital
- (43%) were planned for delivery in the tertiary centre
- (7%) were intended for palliative care.
8% of the babies were born outside their planned delivery destination (FIGURE 3). Two (7%) of the neonates initially deemed suitable for local hospital delivery were transferred to the tertiary centre postnatally, due to a different diagnosis made after birth. All of the planned palliative care cases were born in their local hospitals.
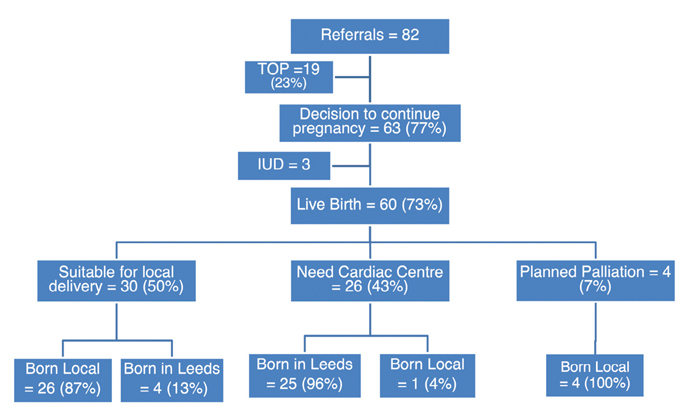
FIGURE 3 Delivery trends during the first half of the study period, pre-guideline. Key: TOP=termination of pregnancy; IUD=intrauterine death.
Post-guideline period
After the guideline was implemented, the cases were antenatally categorised using the traffic light system. Among the live births:
- 60 (56%) fell into the red category
- 35 (33%) green category
- 6 (6%) amber category
- 5 (5%) purple category.
Deliveries in their planned destination were achieved in 95% of cases (FIGURE 4). 5% of babies in the red category were born in local hospitals, while 3% belonging to the green category were born in the tertiary centre.
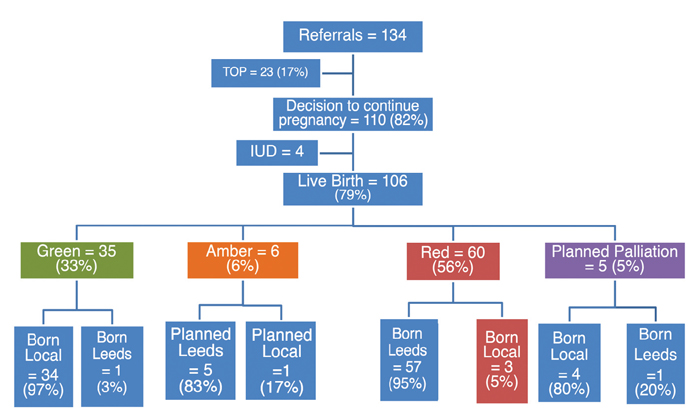
FIGURE 4 Delivery trends during the second half of the study period, post-guideline.
The demographic data and characteristics of babies born before and after the Place of Delivery Guideline’s implementation are provided in TABLE 1. During the study year, extracardiac diagnoses co-existed with cardiac diagnosis in 19% of cases (TABLE 2). Interestingly, this was found to be twice as common in babies born in local hospitals (28% and 12%, respectively), predominantly attributable to babies with trisomy 21.
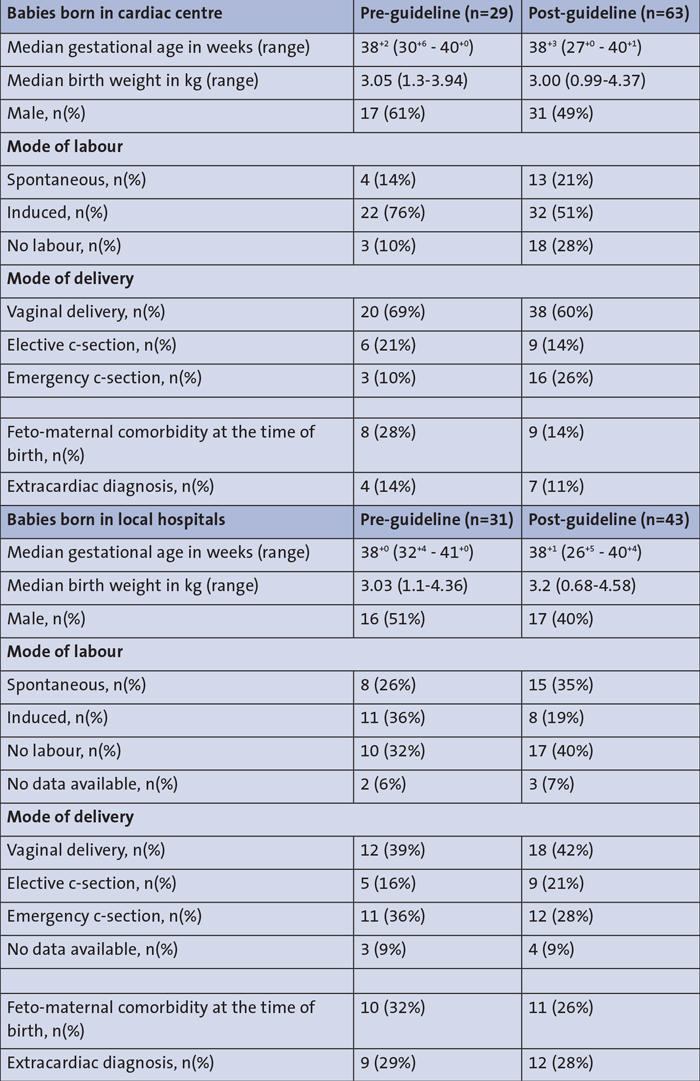
TABLE 1 Demographic data and characteristics of babies born before and after implementation of the Place of Delivery Guideline.
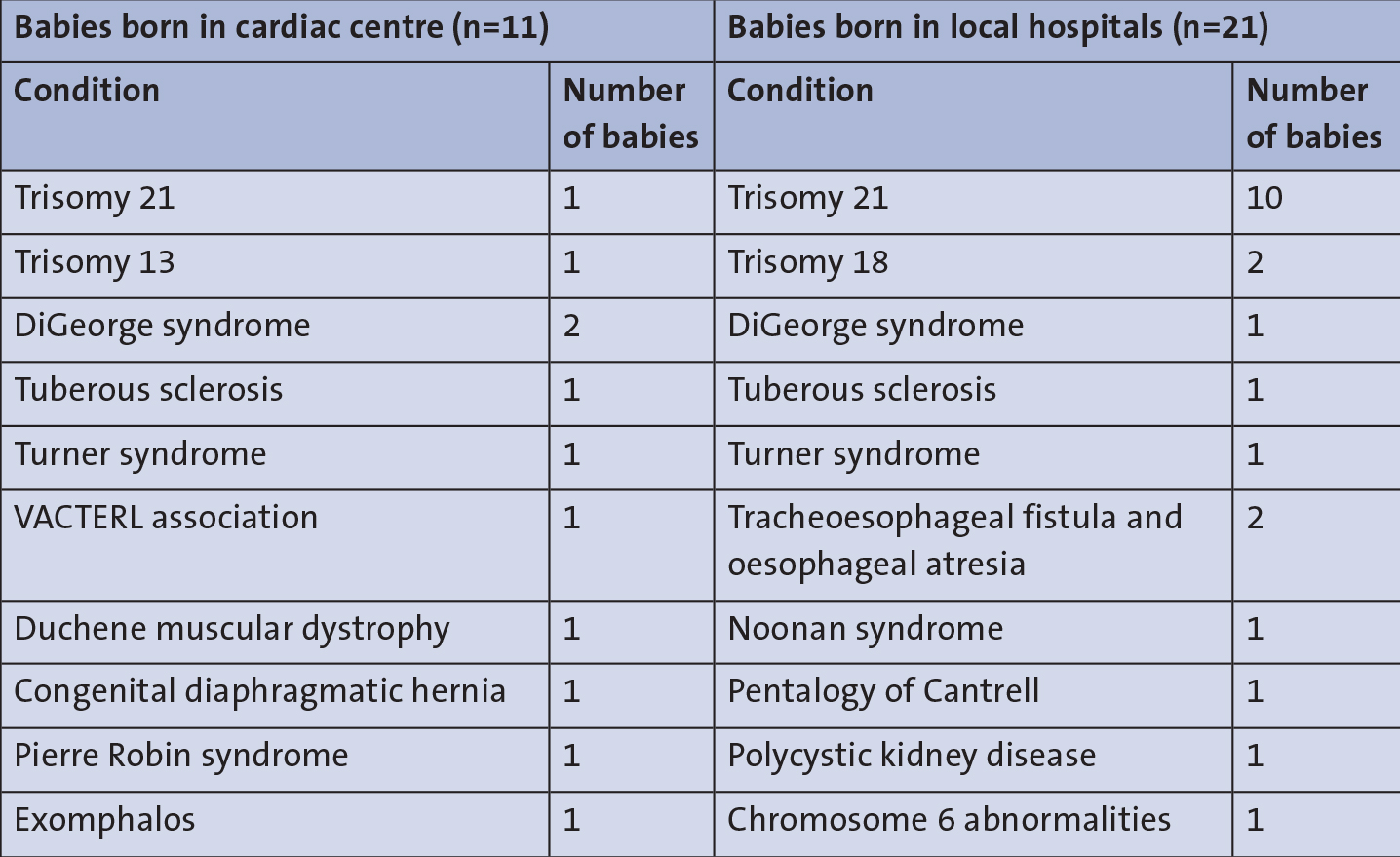
TABLE 2 Extracardiac diagnoses.
Discussion
In this study, we conducted a retrospective review of delivery practices for babies with CHD in Yorkshire and Humber before and after the publication of guidance on the place of delivery in 2021. The results indicate a 3% reduction in babies born off-pathway following the Place of Delivery Guideline and an overall increase of one day in gestational age for all babies born locally and in tertiary centre after the guideline's implementation. This is a small but clinically important improvement for the individual patients.
Antenatal diagnosis of CHD has been associated with higher rates of instrumental deliveries and caesarean sections17 and there is an increased likelihood of delivery occurring before 39 weeks.18,19 Our review further reinforces this finding. Infants in the cardiac centre were born at a median gestational age of 38+2, with high rates of labour induction. It appears that women were more likely to be induced early rather than waiting for spontaneous labour, although the specific indications for labour induction were not studied in this review. The local hospitals recorded a gestational age that was on average two days shorter, as compared to the cardiac centre during the first half of the review period with higher rates of spontaneous labour. In the latter half, the disparity in gestational age between infants born in the cardiac centre and those born locally remained consistent. However, there was an overall increase in gestational age by one day across all cases, which could be because of a drop in the number of inductions of labour by 25% and 13% for cardiac centre and local hospitals, respectively, following the guideline.
In their retrospective study, Trento et al observed significantly higher rates of planned deliveries among babies with antenatally diagnosed CHD in comparison to cases of spontaneous onset of labour.20 Our review yielded similar findings, where spontaneous labour accounted for only 14% of cases in the tertiary centre and 26% in local hospitals during the initial six months of the study period. Notably, following the publication of the guideline, we observed a subsequent increase in spontaneous labour, with a rise of 7% and 9% for the tertiary centre and local hospitals, respectively. The rates of elective caesarean sections were also reduced by 7% in Leeds, however, there was a 5% increase in planned caesarean sections in the local hospitals during the latter half of the study period. The rate of planned deliveries could be higher because of the unpredictability of spontaneous labour making it one of the main determinants of the place of delivery of babies with CHD.7 Throughout the study period, of the five babies that were delivered off-pathway locally, three were due to spontaneous premature labour.
It is not uncommon for cardiac abnormalities to be associated with other non-cardiac anomalies, including chromosomal disorders, genetic syndromes and other congenital malformations.21 The reported incidence of extracardiac lesions varies between 10% and 50% in the existing literature.22,23 In our review, we found that 19% of CHD cases were accompanied by an extracardiac diagnosis with trisomy 21 being the most prevalent (34%), followed by DiGeorge syndrome (10%). Interestingly, our study revealed that 28% of babies with CHD born in local hospitals had extracardiac diagnoses, in contrast to only 12% of babies born in the tertiary centre (odds ratio=1.59; 95% CI=1.02-2.57). This discrepancy may be attributed to certain types of CHDs being more commonly associated with extracardiac anomalies than others. Notably, a significant portion of atrioventricular septal defects (nine out of 12 cases) were determined to be suitable for delivery in local hospitals. Of these, 75% were linked to trisomy 21 during the study period.
Numerous initiatives and research endeavours are dedicated to amplifying the rate of prenatal CHD detection, however, a thorough investigation of the precision in prenatal CHD detection has not been extensively undertaken.24 Existing studies exhibit a notable range of diagnostic discrepancies between antenatal and postnatal cardiac diagnoses, spanning from 3% to 14%.24-26 Antenatal diagnostic accuracy of CHD in Yorkshire and Humber was beyond the scope of our review, however, it was noted that throughout the study year, 66 babies were deemed suitable for local delivery and 3% of these babies required urgent transfer to the tertiary centre postnatally due to diagnostic discrepancy.
Just over 5% of total live births were planned to have palliative (comfort) care following birth. 89% of these babies were delivered in a hospital closer to their homes for palliation and only one baby was delivered in the tertiary centre due to multisystemic anomalies, including congenital diaphragmatic hernia.
Conclusion and recommendations
In our cardiac network, there was an improvement in off-pathway deliveries as well as in the gestational age at birth following the implementation of the Place of Delivery Guideline. However, it remains important to acknowledge that certain deliveries will inevitably deviate from these recommended pathways due to parental preferences or unexpected obstetric emergencies where maternal health takes priority. Enhancing parental under-standing, providing reassurance and fostering effective communication between relevant departments and professionals holds the potential to ameliorate situations where deliveries stray from the intended course. We are planning to utilise the regional neonatal transport team to rigorously monitor and analyse all the instances of off-pathway deliveries to facilitate ongoing quality improvement in this pathway.
Acknowledgement and author contributions
We offer our gratitude to all the PECs in Yorkshire and Humber who have helped to gather the local data for this project.
MRA: idea for the article, design, data collection and analysis, writing. LM: idea for the project, design, data collection and analysis, writing. FW: idea for the project, manuscript review. AC: idea for the project, manuscript review.
Or read this article in our
Tablet/iPad edition
- Delivery practices for babies with antenatal diagnosis of CHD have improved since implementing the Place of Delivery Guideline.
- Parental wishes and emergency care are drivers for off-pathway deliveries.
- There is need to monitor off-pathway deliveries and provide targeted solutions for individual cases.
Also published in Infant:
