

Talking about lactation – the importance of shared decision making in antenatal anticipatory care planning
When discussing lactation management as part of an anticipatory care plan, healthcare professionals should impartially discuss the choices available to families without personal judgement or bias to support families to come to their own informed decisions. This article outlines how the Milk Bank at Chester has been working collaboratively with the Forget Me Not Children’s Hospice and loss families to co-develop a leaflet to educate and support families on their lactation choices following an antenatal diagnosis of a life-limiting condition with a shortened life expectancy.
Rowen Emmett-O’Toole
Milo’s Mummy and Advanced Clinical Practitioner
Laura Atherton
Bereavement Lead – Memory Milk Gift Initiative, Milk Bank at Chester,
Countess of Chester Hospital
laura.atherton4@nhs.net
Sara Balmforth
Perinatal Midwife, Forget Me Not
Children’s Hospice
Emmett-O’Toole R., Atherton L., Balmforth S. Talking about lactation – the importance of shared decision making in antenatal anticipatory care planning. Infant 2023; 19(4): 134-38.
‘Palliative care for babies with life-limiting conditions is an active and total approach to care, from the point of diagnosis or recognition, throughout the child’s life, death and beyond. It embraces physical, emotional, social, and spiritual elements and focuses on the enhancement of quality of life for the child… and support for the family. It includes the management of distressing symptoms, provision of short breaks and care through death and bereavement.’
Together for Short Lives.1
As diagnostic technology and fetal medicine advance, the prevalence of life-limiting fetal diagnoses made antenatally increases. This puts families in a position where they experience anticipatory grief and face the difficulty of navigating the next few weeks or even months, parallel planning while trying to make meaningful memories for the remainder of their pregnancy, during their birth and during the life of their child.2 Where families have received such a diagnosis, they require support in decision making; in these circumstances, perinatal palliative care and anticipatory care planning is considered best practice.3 Anticipatory care planning has been reported to be functional and therapeutic for families, allowing them to formally document and communicate their wishes with the multidisciplinary team (MDT). The creation of a palliative care birth plan goes beyond that of a conventional birth plan in that it offers families a sense of control, allowing them to discuss their plans and wishes while being compassionately supported to make informed choices to honour the life of their unborn child.4
Lactation management and milk donation after loss
It is at the point of anticipatory care that conversations around lactation management, including milk donation after loss, are appropriate. Working alongside families with lived experience of the information and support surrounding lactation management and milk donation, we have identified a UK-wide need for further discussions around lactation support and information on the choices available to them.
“I can understand why no one wants to talk about lactation after loss… the fear of upsetting us further… but how dare they play god by not discussing our choices that are available to us and our family.”
Rowen Emmett-O’Toole, bereaved mother, 2022.
Families report feelings of isolation and exclusion where they have received poor, or conflicting information from different members of the MDT.5 Consistent and accurate information supports families to feel engaged with their baby’s treatment and care, yet the topic of lactation and milk donation is still not widely discussed with families during the antenatal period where a life-limiting diagnosis has been given.
Caring for families should begin antenatally
The transformation of care for families and their babies is well supported and advocated for through national and international guidelines and organisations. The Baby Friendly standards provide services with a roadmap for transforming care for all babies, their mothers, and families, stating: ‘All parents should be supported to respond to their baby’s needs for love, care and comfort in a way which promotes close parent-infant relationship and supports the mental health of the mother and baby.’6 The British Association of Perinatal Medicine (BAPM) published guidelines in 2019 for the perinatal management of extreme preterm birth before 27 weeks’ gestation, stating that: ‘When neonatal problems are anticipated, communication with the parents should begin antenatally, involving face-to-face discussion with the neonatal team supplemented by written materials’.7
The relationship held between patient (in this case, mother and family) and clinician (whether this be a medical professional or healthcare professional), was traditionally perceived to be paternalistic, where clinicians made decisions on behalf of the patient.8 This has been assumed from clinicians believing that they are acting in the patient’s interest and patients believing that clinicians know best due to their levels and standards of professional training; however, the danger in this assumption by both parties can lead to aspects of importance to patients (families) not being revealed or touched upon during clinical encounters.9
In more recent years, and following the NHS reform, there has been a paradigm shift away from this paternalistic view, with greater emphasis placed on person-centred care, where patients and clinicians form mutualistic relationships working in partnership to empower patients to make informed decisions regarding their (and their babies’) treatment and care.10 This has been supported by the publication of National Institute for Health and Care Excellence (NICE) guidelines for shared decision making.3 Yet, despite this, we know that when it comes to antenatal and post-loss care, healthcare professionals (HCPs) are still failing mothers and families by not supporting them to make informed choices. Feedback received from a professional focus survey undertaken by the Memory Milk Gift Initiative, revealed that some HCPs are cautious of offering choices, including milk donation after loss, as they have pre-conceived thoughts about how introducing and discussing the options available to families would be received. One response from a HCP who participated in the survey stated that one of the barriers to offering choices when discussing lactation and loss was: ‘Knowing how that kind of conversation would be received… worrying that it would come across as insensitive and hurtful.’
Beauchamp and Childress1 define autonomy as: ‘Independent exercise of individual choice, free from controlling interference by others and personal limitations that prevent meaningful choice.’ How can we empower HCPs providing antenatal treatment and care to embed shared decision making into their every day, standard practice?
Giving the right information and choices to families
Following the launch of the Memory Milk Gift Initiative,12 the Milk Bank at Chester has seen a four-fold increase in the number of mothers wishing to donate their milk following loss. We are confident that this number could be higher if the right people were providing the right information and choices to families. Our aim was to work with loss families and HCPs working in the field, to co-develop a leaflet to educate families on their lactation choices following an antenatal diagnosis of a life-limiting condition with a shortened life expectancy. The Milk Bank at Chester works closely with neonatal units and children’s hospices across the country; the introduction of a leaflet for antenatal diagnosis is supported by the Forget Me Not Children’s Hospice, West Yorkshire. Anecdotally, they report an increased number of families wishing to donate their breast milk after loss, and they support us in enabling families to access trusted and informed sources and to help standardise choices, supporting health equalities nationally.
To support a holistic antenatal care pathway where a life-limiting diagnosis has been given, we must raise awareness of lactation choices and empower HCPs to fulfil their duty of care by sharing choices available to families and signposting them to the appropriate services. Families and caregivers are now being recognised as core members of the care team; family-integrated care (FICare) is a model of care that is implemented in the UK across neonatal units and networks, its aim to enable families to act as primary caregivers for their babies, working in partnership with clinical teams.13 Shared decision making is a joint process, where HCPs work in partnership with a person to reach a decision about their care, based on individual preferences, beliefs and values. Through information sharing, the person making the decision is supported to understand the risks, benefits, and any possible consequences of different options available to them.14 HCPs have professional standards to adhere to, including ensuring valid and informed consent is voluntarily obtained prior to the undertaking of any decision or treatment.15-17 Shared decision making underpins the basis of informed and valid consent; if HCPs are failing to provide the choices available, how are they obtaining valid consent?
Lactation information following an antenatal diagnosis
Working with families living with loss and HCPs in the field enabled us to identify a gap in the written literature that we give to our families. We currently provide written information to families post-loss; until now, there was an absence of supporting written information for families who have received an antenatal diagnosis of a life-limiting condition with a shortened life expectancy.
The Milk Bank at Chester has worked in partnership with the Forget Me Not Children’s Hospice to develop the leaflet on lactation information following an antenatal diagnosis (FIGURE 1), which includes information about:
- understanding the lactation process
- antenatal hand expression
- continuing to express milk
- deciding what to do with milk that you have already expressed
- stopping your body producing milk.
FIGURE 1 Lactation Information Following An Antenatal Diagnosis: the leaflet and associated QR code.
When discussing lactation management as part of an anticipatory care plan, HCPs should impartially discuss the choices available to families, without personal judgement or bias, to support families to come to their own informed decisions.18 Families participating in anticipatory care plan discussions might have a stress response to the topics being discussed, or they may have entered the discussion in a pre-heightened stress response state, due to the emotionally challenging experience of receiving an antenatal diagnosis with a shortened life expectancy. Research has shown that stress influences cognitive function and processing, including memory and decision making.19 It is therefore important for HCPs to recognise that this decision will need to be revisited and that it might change, families should be supported with this and reinformed of their choices. Families will ideally have a named HCP leading on their care; where this is not possible, all HCPs involved in the integrated MDT should have the same consistent approach when presenting the choices available.1 Information given to families should be provided in the most appropriate and accessible format, taking into consideration any communication needs, language barriers, and the health literacy status of the family.20 The information should also offer signposting to additional relevant evidence-based literature and appropriate support networks through registered charitable services or organisations.21
A natural starting point for this conversation with expectant families is lactation management, particularly as the female body can begin to produce colostrum from as early as 16 weeks of pregnancy. To support families with choices in the antenatal and postnatal periods, HCPs should have knowledge underpinned by the physiology of lactation (FIGURE 2).22 Families with an understanding of the physiological processes (eg mature milk production occurring due to hormonal changes that occur following the delivery of the placenta), can better prepare for the delivery of their baby. They may choose to start colostrum harvesting from 37 weeks, if medically cleared to do so, and they may choose to donate this first milk. This can aid in memory making.23
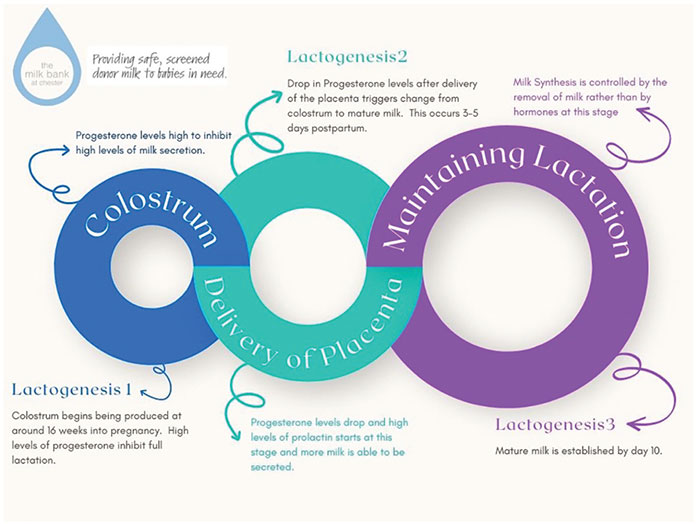
FIGURE 2 The stages of lactogenesis to support HCPs to educate families in the physiology of lactation.
The role of HCPs in educating and supporting families with lactation choices
The female body undergoes numerous physical and emotional changes in the immediate postpartum period and some mothers report feeling that milk production following their loss is their body playing tricks on them. This is also echoed by mothers whose baby is under feeding restrictions for medical purposes – where the mother feels taunted by her own body’s overproduction of milk. This milk is sometimes referred to as ‘white tears’ symbolising the emotional grief and burden this can bring.24 HCPs can empower families by educating and supporting them with open and honest conversations regarding lactation and lactation management choices. This can help decrease any stigma, preconceived ideas or associated perceived guilt that some mothers and families report.
A loss mother who vocalised her wishes to express and donate her milk to her antenatal care team (after being informed that her baby had a shortened life expectancy through antenatal diagnosis), reported that lactation suppressants were in the same tablet pot as her post-delivery analgesia. As an HCP herself, she reflected that she only felt empowered to ask what the additional tablets were due to her professional role and background. In doing so, she was able to decline the medication and pursue her choice of milk donation after loss as a way of honouring her baby and continuing memory making. This could have been a very different outcome had she not noticed the extra tablets and had she not had the courage to speak up while being in the traumatic, stressful, and vulnerable situation – the choice of donating after loss would have been taken away from her by the lactation suppressants.
Antenatal hand expression
Expressing milk antenatally from 37 weeks of pregnancy25 has many health benefits for the baby and the mother. Hand expression and colostrum harvesting can naturally induce labour due to the rise in oxytocin and this may reduce the requirement for medical interventions for the induction of labour.26 Colostrum is the first milk made by the breast; it is highly concentrated meaning babies only require a small amount for each feed.27 Colostrum contains immunological agents to help protect babies from infection and colonise their gut with ‘healthy bacteria’.28 For neonates in intensive care or those receiving palliative care shortly after birth, antenatally harvested colostrum can be used for oral mouth care to maintain a clean and comfortable mouth for the baby. This may also bring comfort to the mother, helping her to connect and have a ‘continuing bond’ with her baby.29 A continuing bond has been described as the emotional attachment that a bereaved person continues to maintain with the deceased, long after the death.30 This can be particularly important for loss mothers that have a strong desire to breastfeed their baby.
Antenatal hand expression can be an example of parallel care planning where the family works with their MDT care team to plan for the best outcome for their baby, while also planning realistically for the worst-case scenario.3 During such discussions, families can make plans to express antenatally for their baby with the hope that they are well enough to feed but take comfort from knowing that the colostrum can still be used for oral care if their baby is unable to feed. If this is their choice, families should be advised and educated on how to undertake antenatal hand expression and where possible, supplied with an expression kit including syringes, bonding cloths and instructions for the safe storage of the colostrum.
Continuing to express milk
Some families report that they take great comfort in donating their babies’ surplus milk. It supports their motivation to continue to express in the hope that their own baby will be able to utilise the milk, while offering comfort and reassurance knowing that ‘every drop counts’31 and any surplus milk will be utilised for other sick and premature babies or to support vital research. If a baby sadly dies, families have the choice to donate their milk in memory of their baby to the Memory Milk Gift Initiative.32 Bereaved families may seek ways to maintain bonds with their baby and this may take the form of mothers continuing to donate milk in their baby’s memory. This may be through lactation induction where their baby has been stillborn or died shortly after birth, or by the mother continuing to express her milk.22 The Memory Milk Gift Initiative can continue to provide support for families to donate for as long as they feel it is beneficial to do so.
By continuing to express their milk, loss families report feelings of maintaining and honouring their baby’s legacy. Where families have chosen to donate milk formally through a recognised milk bank, they are able to continue memory making posthumously through the Memory Milk Gift Initiative. The Milk Bank at Chester offers loss families who have donated their baby’s milk a wooden memory milk pebble with their baby’s name (FIGURE 3), and the option to add their baby’s name to the hand painted Memory Milk Gift tree at the Milk Bank at Chester. Memory making opportunities offer families continuing bonds with their babies, with families experiencing, processing and transitioning their grief through objects associated with their baby. The linking of objects has been found to support grieving families to feel connected to their baby, assisting in the mourning process and supporting the mother’s perinatal mental health.33
A Memory Milk Gift Garden is situated in the Countess of Chester Country Park – a quiet space for families to reflect and remember their baby (FIGURE 3).
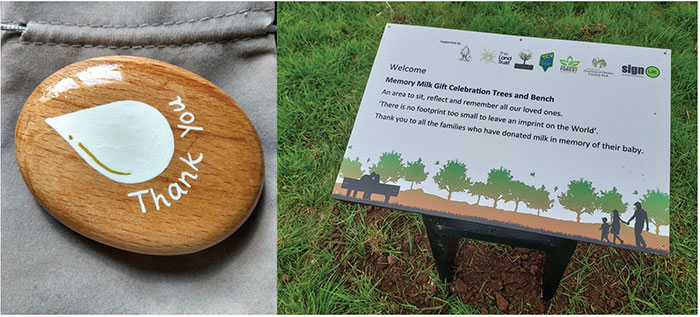
FIGURE 3 The Memory Milk Gift Initiative wooden memory pebble and the Memory Milk Gift Garden, situated in the Countess of Chester Country Park.
Summary
Forget Me Not Children’s Hospice has been at the forefront of pioneering changes in antenatal care where a life-limiting diagnosis has been given, being the first hospice in Europe to appoint a midwife. The team there have been working collaboratively with the Memory Milk Gift Initiative to ensure that the families under their care are being offered antenatal choices in lactation management. Through the introduction of expression kits and the development of the information leaflet, Lactation Information Following an Antenatal Diagnosis, families under the care of the hospice now have timely access to appropriate information and evidence-based literature to ensure that they are offered all the choices available to them and supported with whatever choice they make.
Working first hand with families living with loss, we have seen the detrimental impact that can occur when certain choices are not offered to families, or they are not honoured. Families report feelings of anger, regret, guilt, disappointment, and poor mental health consequently to their autonomy being ignored. It is our mission for every family in receipt of a life-limiting diagnosis with a potential shortened life expectancy to be supported in their antenatal care choices for lactation management and beyond, and for this to be embedded into the culture and stan-dards of care HCPs have a duty to deliver.
Or read this article in our
Tablet/iPad edition
- Loss families are being failed by not having all lactation choices offered to them, or not honoured.
- Some lactation choices can support families with memory making, which can assist in their grieving process and the mother’s perinatal mental health.
- There is a need for healthcare professionals to embody and embed the culture of shared decision making into their everyday practice.
Also published in Infant:
