

Understanding management practice for monitoring and discharging BPD patients
With a lack of national guidelines outlining specific management and discharge criteria, a retrospective analysis was undertaken for a bronchopulmonary dysplasia (BPD) clinic in a tertiary centre to determine the efficacy of its protocol. This concluded consistently positive outcomes, inferring that the criteria used are appropriate for management and discharge. A survey was subsequently undertaken to determine the degree of congruence nationally. It was found that there were many similarities in practice, particularly with respect to discharge criteria, suggesting an appropriate basis from which a protocol could be established.
Sinead CartonFoundation Doctor, University of Nottingham, Queen’s Medical Centre (QMC)
sinead.carton1@nhs.net
Theodore Dassios
Professor of Neonatology, King’s College Hospital NHS Foundation Trust, London
Ian Sinha
Consultant Respiratory Paediatrician and Professor of Child Health, Alder Hey Children’s Hospital, Liverpool
Stephen Wardle
Consultant Neonatologist, Nottingham Children’s Hospital, QMC
Jayesh Mahendra Bhatt
Consultant Respiratory Paediatrician, Nottingham Children’s Hospital, QMC
Carton S., Dassios T., Sinha I., Wardle S., Bhatt J.M. Understanding management practice for monitoring and discharging BPD patients. Infant 2024; 20(2): 64-67.
Background
Bronchopulmonary dysplasia (BPD) is a complex condition that has a significant impact on an individual’s respiratory system, growth and development. Management of this condition, including the use of long-term oxygen therapy (LTOT), has the principal focus of preventing complications and associated sequelae including hypoxia, pulmonary hypertension and neurodevelopmental delay.
BPD encompasses a spectrum of clinical states, however there is a consistent acknowledgement that it reflects a patient of preterm birth requiring supplemental oxygen beyond 36 weeks post-menstrual age.1 The most predominant phenotype arises from immature development of the respiratory system, though other factors including exposure to inflammation, genetics, epigenetics and placental vascular inadequacy can influence susceptibility and severity.2 National and international guidelines3-5 advise protocol driven care and a multidisciplinary approach for the management of babies with BPD to support weaning of LTOT and clinical stability. There is, however, a lack of consensus in guidelines regarding oxygen weaning strategies and no recommendations as to when infants can be discharged from routine follow up, giving rise to ambiguity, locally-derived protocols and the potential to prevent optimal care being consistently delivered. Decision making surrounding discharge may influence a child’s growth, lung development and potential for complications, including pulmonary hypertension.
We retrospectively analysed the clinical status of babies that were discharged from a tertiary BPD clinic to see if this can inform the criteria for how they are managed and discharged. A comprehensive analysis was subsequently undertaken and established the data presented in TABLE 1.
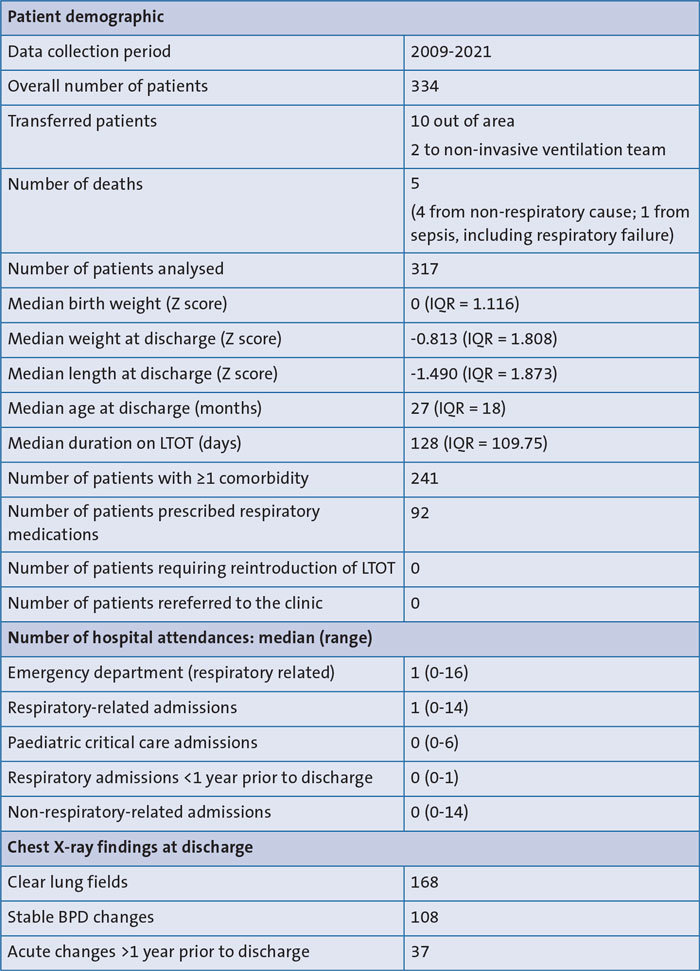
TABLE 1 Analysis of clinical outcomes for patients discharged from a tertiary BPD clinic. Key: LTOT=long-term oxygen therapy; Z score=the number of standard deviations from the mean; IQR=interquartile range; BPD=bronchopulmonary dysplasia.
Of those who had comorbidities, the most common was neurodevelopmental with 50% of the cohort having a diagnosis. The second most common was respiratory. Relatively few patients remained on any respiratory medications, there were very few hospital admissions and no paediatric intensive care admissions in the year prior to discharge. On imaging, most patients either had clear lung fields or stable BPD changes that included linear fibrosis, prominent bronchovascular markings and hyperinflation. Importantly, no graduate of the clinic required reintroduction of LTOT following oxygen removal from the household nor re-referral to a respiratory service, inferring that respiratory stability was consistently achieved and maintained following discharge. We therefore considered that the criteria used within this clinic were appropriate for the continued care and monitoring of future BPD patients.
From this, we wanted to determine if there was any correlation with practices nationally, with a view to potentially creating recommendations that may guide best practice.
Methods
An email survey was carried out with members of the British Paediatric Respiratory Society (BPRS) and the British Association of Perinatal Medicine (BAPM), which collectively have over 2,000 members. These societies have many members responsible for the care of BPD patients and responses were gathered from individuals on behalf of their trusts. Additionally, 106 hospitals within the neonatal network were contacted via telephone, 72 of which were available for response. In total, 45 were able to comment on management practices following hospital discharge. The survey sought to ascertain the monitoring practices of these services and the criteria that informed the decision for discharge. The email and telephone surveys asked the following questions:
- What’s your specialty (general paediatrician, neonatologist, paediatrician with specialist interest in respiratory, paediatrician with specialist interest in neonatology, other)?
- Which type of unit are your BPD patients graduates from (level 1, 2 or 3)?
- How frequently are BPD patients reviewed in clinic (3-monthly, 6-monthly, annually, other)?
- How often are oxygen studies carried out and oxygen weaned as appropriate (monthly, 3-monthly, 6-monthly, other)?
- At what age do you discharge babies (1 year, 2 years, time based on clinical stability, time following duration off oxygen, other)? Please elaborate.
- What criteria are used to inform your decision for patient discharge from follow up (clinical, radiological, current treatment, hospitalisations, other)? Please elaborate.
Results
The survey responses regarding management of BPD patients are summarised in TABLE 2.
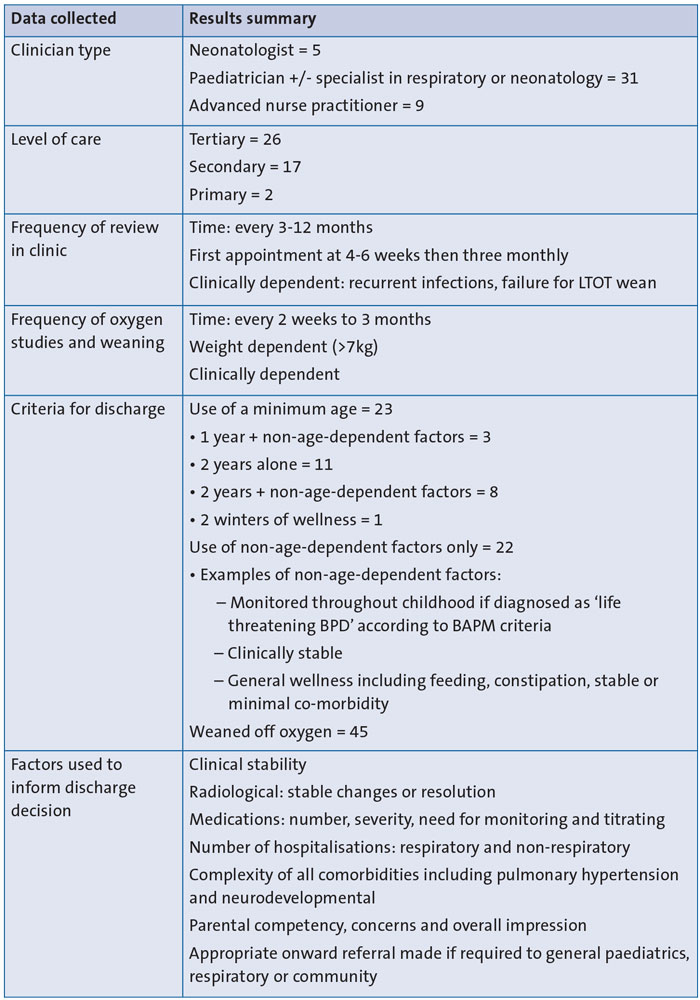
TABLE 2 Summary of survey responses (n=45) regarding management of BPD patients and discharge criteria.
In five trusts the management of these babies is neonatology-led until discharge or until one or two years of age, at which point their care is transferred to a paediatric respiratory team if required. All others are under the care of respiratory paediatricians or generalist paediatricians for the entirety of their BPD management following discharge from hospital, though most report ongoing additional input from neonatologists for overall management until one year of age.
Nearly half of the clinics review patients every three months, while 14 review 4-6 weekly for an initial period or over their first winter. Other responses report varying frequency depending on success of weaning of oxygen and clinical necessity. Two clinics do not review patients at all unless clinically indicated, relying on community and sleep service teams for weaning. While on oxygen, most commonly clinics carry out monthly assessment of oxygen and titrate accordingly, though others have frequency of assessment decided by an individual’s clinical progress. Discharge is predominantly either determined by age or dependent on clinical stability, with the majority supporting that decision for discharge is clinically driven alone. Three trusts review patients to one year and 14 continue until two years corrected gestational age in congruence with BAPM guidance, and then consider discharge based on stability and comorbid burden.
Following weaning of LTOT there is a consensus by all that an interval period of stability is required for confidence in remaining clinically well prior to discharge, although the duration of this varies greatly from 6-8 weeks to two winters. This disparity is somewhat accounted for in that the two trusts with the shortest duration have an open access policy following discharge. This decision was explained by reflecting on their patients’ clinical vulnerability and susceptibility to deterioration in view of respiratory history and comorbidities. On balance, although different strategies are undertaken, it can be concluded that most trusts find that a period of monitoring or access is indicated for a prolonged period to ensure respiratory clinical stability is maintained.
All responses support the use of multiple elements to inform the decision for discharge and do not consider LTOT weaning alone to be a sufficient indicator. Criteria most commonly include number of hospital admissions, degree of comorbidity and requirement for respiratory medications. Two trusts include the resolution of pulmonary hypertension and another reflected on parental confidence and ability as a crucial factor that could stand alone as rationale for ongoing input. Some disparity in timeframe for discharge may also be accounted for in the variable ability to refer to community and other outpatient teams for monitoring and ongoing input. There is disparity in frequency of monitoring during the oxygen weaning period and beyond, and some variability on the specific criteria that are used to decide on discharge. Responses indicate that while some trusts utilise locally-set criteria and protocol, others determine readiness by clinical impression and individual decision making alone.
Discussion
Overall, the responses suggest that there is a large degree of protocol correlation between trusts. Whether care is driven by the neonatology team or paediatric team, they all consider multiple factors to inform their decision to discharge; care is largely dictated by clinical stability and babies reaching a minimum of one or two years of age. Considering the variability in some areas such as oxygen monitoring and weaning, as well as the concept of having a minimum age, it would be important to further explore the evidence base and rationale behind these choices to establish consensus in the future. Areas lacking evidence to enable informed decision making require high quality randomised controlled trials for further protocol development. The responses also emphasise the key role of parents in making an informed decision for discharge. We consider it pertinent, therefore, that they are involved in the development of future guidelines. Their understanding of the child, confidence in meeting their needs and knowing what ongoing challenges they face is a fundamental part of determining if a patient is ready for discharge.
A limitation of this survey resides in the relatively small number of responses and uncertainty of how this number stands proportionally against all that are involved in the management of BPD patients. Of all those contacted, 72 participated but 27 were unable to provide information. This was mostly down to not having a person available who was aware of the local BPD management practices and so unable to complete the questionnaire fully. This highlights that the specialist care of these babies resides with a small number of clinicians even within the paediatric and neonatal community. This is however a crucial consideration when judging the degree to which we can consider that these responses reflect national practice.
Conclusion
To achieve best clinical practice and improve overall standard of care, we propose that a protocol/guideline to help manage these babies could be derived, based on the relative consensus achieved so far and from further exploration of clinical outcomes. Outstanding uncertainties should be investigated with randomised controlled trials.
Author contributions
SC: conceptualisation, data curation, formal analysis, project administration, methodology, validation, visualisation, writing original draft, writing review and editing. JMB: conceptualisation, data curation, project administration, methodology, resources, supervision, writing review and editing, validation, review and editing. TD: conceptualisation, validation, review and editing. IS: conceptualisation, validation, review and editing. SW: conceptualisation, validation, review and editing.
Or read this article in our
Tablet/iPad edition
- Retrospective analysis of discharge criteria used in a clinic found consistent clinical stability and positive clinical outcomes on discharge.
- A survey provided details of national BPD management practices and discharge criteria and found a large degree of congruence.
- The findings suggest a basis for development of guidelines to help manage these babies.
Also published in Infant:
