

Home oxygen for infants leaving neonatal units: a nationwide survey
Home oxygen is widely prescribed for ex-preterm infants being discharged home with bronchopulmonary dysplasia. Anecdotally, practice was felt to vary widely between neonatal units (NNUs) across the UK, despite British Thoracic Society guidance on home oxygen prescription. This survey is the most comprehensive to date, looking at variations in both pre- and post-discharge practices across the UK. It found that practice does indeed vary widely between NNUs and suggests that updating guidelines may be useful to help unify practice.
Peter SchulgaMBChB, MRCPCH
Paediatric Trainee
peter.schulga@nhs.net
Peter Corley
MBChB, MRCPCH
Paediatric Trainee
Chikkanayakanahalli Manjunatha
MB BS, MRCPCH
Consultant Neonatologist
Palghat N. Gopalakrishnan
MB BS, MRCPCH
Consultant Neonatologist
Neonatal Unit, University Hospital Wishaw
Home oxygen therapy has been used in infants for over 40 years in the context of bronchopulmonary dysplasia (BPD).1 BPD is a common pathology seen in neonates and home oxygen use is widespread. The prevalence in England and Wales of home oxygen use in children is 0.33/1,000 population and 68% of these children have a diagnosis of BPD.2 Previous studies suggest that the use of home oxygen varies widely, both internationally and within the UK. British Thoracic Society (BTS) guidelines state a diagnosis of BPD can be made if an infant requires supplemental oxygen after both day 28 of life and 36 weeks’ corrected postmenstrual age.3 This guideline on the use of home oxygen in children states that home oxygen is aimed at primarily:3
- reducing or preventing pulmonary hypertension
- promoting growth
- reducing episodes of desaturation
- reducing airway resistance.
It also links home oxygen use to improvements in neurodevelopmental outcomes and reductions in sudden death in infancy.3 However this is primarily based on poor-quality evidence (C or D, based on the SIGN grading system), and the guidance has not been revised in a decade. These factors may contribute to a wide variation in practice as units choose not to adhere to these guidelines.
This study aims to investigate the use of home oxygen in NNUs across the UK. The survey was designed to assess the variation in practice, both before discharge and after discharge, of NNUs prescribing home oxygen for BPD. A literature review was also performed to assess practice globally and to identify features of good practice to adopt into management.
Literature review
A literature search was conducted using Embase, Ovid-Medline, Cinahl and the Cochrane Library using the key phrases: bronchopulmonary dysplasia, BPD, chronic lung disease, home oxygen, saturation study, and pulse oximetry.
No randomised controlled, quasi-randomised studies or case control studies could be found to evidence the use of home oxygen in BPD. However there were cohort studies and papers reporting clinician experience and these are discussed in the following sections.

The management of infants at home on oxygen varies widely between neonatal units.
A German study4 looked at the variation in practice in saturation thresholds before prescribing home oxygen. It found huge variation – the thresholds for prescribing home oxygen on discharge varied from <80% to <94%, mostly based on mean saturations from an overnight saturation study. However, 11% of units were making this decision on spot saturation measurements. A follow-up study 13 years later5 found this wide variation in practice persisted, with thresholds again varying from <80% to <94%. Similar variation of practice was identified in an American survey at the Vermont-Oxford Network conference. Thresholds for starting home oxygen varied between <84% and <98%, with target saturations varying from >84% to >98%.6
Post-discharge practice also varies, with one paper from the UK highlighting the differences in practice when considering withdrawal of home oxygen. Variations included assessing the presence of pulmonary hypertension, parental opinion and the onset of the winter season and inter-current respiratory illnesses.7 Another survey looked at weaning of home oxygen and the criteria for initiating the weaning process. Weaning was primarily based on overnight home oxygen saturations rather than a standardised protocol for weaning.8
Both the Thoracic Society of Australia and New Zealand9 and the Working Group in Perinatal Respiratory Diseases of the Spanish Society of Pediatric Pulmonology10 produced position statements regarding the use of home oxygen therapy in BPD. The Australian and New Zealand position statement sets out the guidance for use of home oxygen including minimum mean target range for SpO2, the recommendation for assessing oxygen requirement during sleep with continuous overnight oximetry and the use of clinical assessment and documentation of adequate oxygenation in room air before discontinuing home oxygen. It also accepted the limited objective evidence on which to base the recommendations.9 The Spanish statement also sets out guidance for clinicians in the use of home oxygen and targeting therapies to help manage BPD.
Methods
A questionnaire was designed to investigate practice both before and after discharge of infants with BPD requiring home oxygen (FIGURE 1.) This survey looked at the timing and interpretation of pulse oximetry studies, thresholds for prescribing home oxygen, and the intervals at which investigations were repeated after discharge. Additionally, management after discontinuing home oxygen was compared.
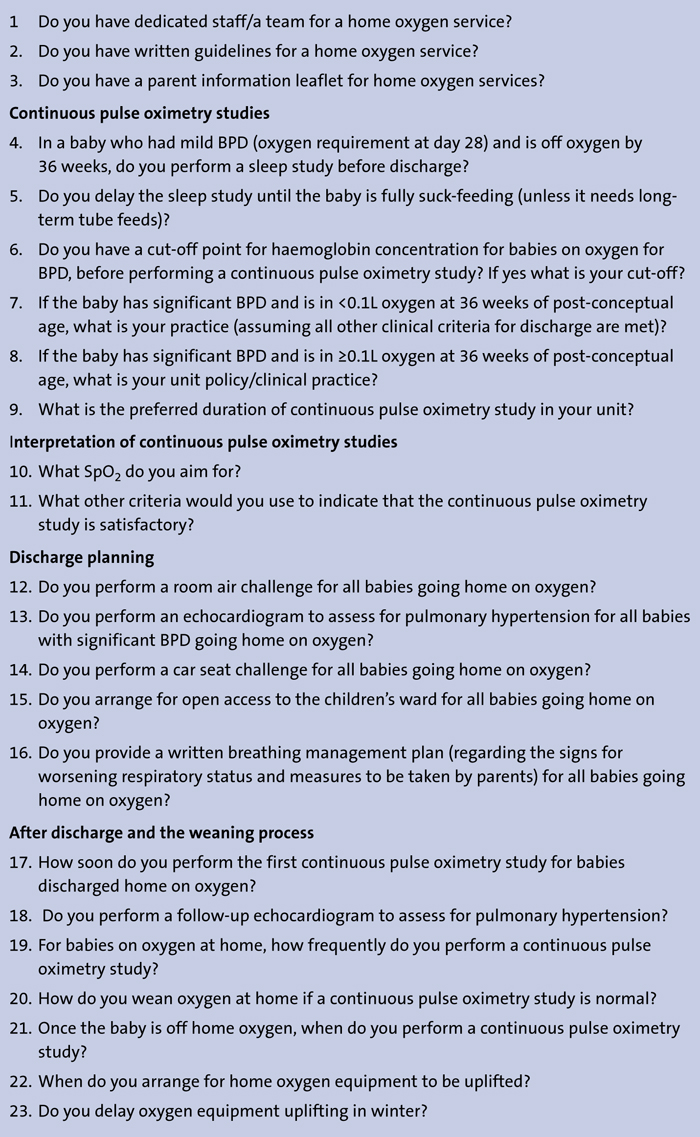
FIGURE 1 The questionnaire for home oxygen use.
Pre-discharge questions included the use of saturation studies to screen for BPD requiring home oxygen, the criteria for a normal saturation study, the use of room air challenges and screening for pulmonary hypertension using echocardiogram.
Post-discharge questions related to further echocardiogram in the community, timing of saturation studies and subse-quent weaning and then uplift of oxygen.
The survey was sent out to 191 NNUs as identified from the British Association of Perinatal Medicine (BAPM) national register of neonatal units and a stamped self-addressed envelope was attached for returning the survey. Two email addresses were also enclosed for those wishing to reply by attachment. All results were analysed together.
Results
There were a total of 62 responses from 191 surveys; a 32.4% response rate. Thirty-two level 3 (neonatal intensive care) units replied (52%), 19 level 2 (local neonatal) units (30%) and 11 level 1 (special care baby) units (18%).
Of the units that replied:
- 43 (69%) had a dedicated home oxygen service
- 41 (66%) had a written guideline for the home oxygen service
- 36 (58%) had a parent information leaflet on the home oxygen service.
Further results are divided into pre-discharge and post-discharge practices.
Pre-discharge
Twenty units (32%) performed saturation studies in mild BPD; those on oxygen at day 28 of life but off by 36 weeks’ corrected gestation. Another 20 units (32%) delayed saturation studies routinely until full suck feeds were established. Five units had a cut off for haemoglobin levels prior to performing saturation studies.
The duration of the saturation study varied, with one unit (1.5%) performing a 6h study, 31 units (50%) performing a 12h study, one unit (1.5%) performing an 18h study and 14 units (23%) performing a 24h study.
Ten units (16%) used a random duration and five units (8%) did not provide an answer. Target saturations (SpO2) varied between responding units, as documented in Table 1, with three units (5%) not providing data. There was no statistically significant difference between the type of unit and the target saturation used.
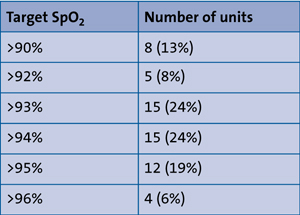
TABLE 1 Target mean oxygen saturations.
Criteria used to interpret saturation studies also varied widely between units. Six units (10%) use number of dips in SpO2, 11 units (18%) use depth of dips in SpO2, 24 units (39%) use both number and depth of dips in SpO2, 13 units (21%) use percentage of saturations 5% below target SpO2. Eight units (13%) did not provide a response.
Nine units (14.5%) performed a room air challenge (as described in Simoes et al11 or a variation thereof), prior to discharge as the evidence shows that saturations reach their nadir at 40 minutes after discontinuing oxygen. Twenty-four units (39%) performed a pre-discharge echocardiogram to screen for pulmonary hypertension.
A ‘car seat challenge’ was performed by 30 units (48%) as the American Academy of Pediatrics12 recommends for all infants born <37 weeks’ gestation. Forty-nine units (79%) arranged open access/self referral to paediatric wards and 34 units (55%) had a breathing management plan.
Post-discharge
The first saturation study in the community (BTS3 recommends within a week of discharge) and a frequency of saturation study in the community (3-4 weekly, as recommended by BTS) are outlined in TableS 2 and 3.
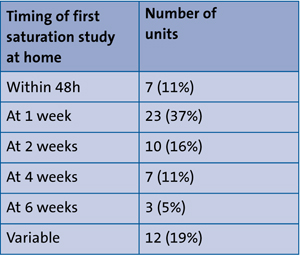
TABLE 2 Timing of post-discharge saturation studies.
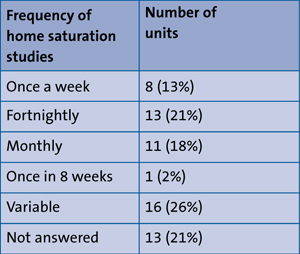
TABLE 3 Frequency of home saturation studies.
Thirteen units (21%) routinely screened for pulmonary hypertension in the community and a further two units (3%) would do so on a case-by-case basis.
The timing of performing saturation studies after discontinuing oxygen also varied. Eleven units (18%) did not repeat, 22 units (35%) repeat after one week and 20 units (32%) repeat after 2-4 weeks.
Uplift of home oxygen varied: eight units (13%) immediately remove oxygen, 22 units (36%) delay for one month, 21 units (34%) delay it for two to three months and 11 units (18%) have variable practice depending on the patient. Thirty-one units (50%) also delay the uplift of home oxygen during the winter season. BTS guidelines suggest that oxygen equipment should remain for three months after discon-tinuing, and suggest that it is prudent to delay until after the winter season.
Discussion
Although only one third of units responded to this survey, the results show wide variation in practice across the UK. This limitation is recognised but it can be used to map variability if not to change practice. While BTS guidance for the use of home oxygen in children does exist,3 many of these recommendations are not based on strong evidence and many units do not adhere to the guidance.
Most striking is the wide range of practice when interpreting saturation studies. Target saturations varied widely, ranging from 90% to 96%. While this range is significantly smaller than that described by previous German studies,4,5 it highlights the lack of concrete guidance for interpreting saturation studies. Additionally, the use of presence and depth of ‘dip’ when interpreting studies varies widely, with some units using both, one or neither. Again, this highlights the lack of national guidance with regards to the interpretation of saturation studies.
Pulmonary hypertension screening before discharge occurs in less than half of units. This may be limited by resources available at each unit (level 1 and 2 units may not have neonatal echocardiography available on site). Chronic hypoxaemia (SpO2 of 88-90%) is known to cause pulmonary hypertension in adults,13 and supplemental oxygen can reverse pulmonary hypertension in infants with BPD.13,14 Given that one of the primary aims of home oxygen is to reduce or prevent pulmonary hypertension,3 this may be an area that requires further study, and further highlights the need for comprehensive neonatal home oxygen therapy guidelines.
Practice also varied widely in the use of saturation studies in mild BPD. Routinely performing saturation studies in those requiring respiratory support for at least 28 days post-delivery, but not requiring support by 36 weeks post-menstrual age is likely to lead to babies who would otherwise not have been given oxygen being started on home oxygen. There were no good trial data found to suggest whether these babies would come to harm if they were discharged without home oxygen. Premature babies who are likely to require home oxygen are likely to still be clinically requiring oxygen at 36 weeks. It would therefore seem sensible to restrict pulse oximetry studies to those still clinically requiring supplemental oxygen at 36 weeks post-menstrual age, and not testing those who have weaned to room air by 36 weeks, even if they fulfil the diagnosis for mild BPD by having required respiratory support at 28 days of age. The financial impact of this is significant given the cost of home oxygen supply and ongoing follow-up.
Post-discharge practice also varied. Most notable is that 18% of units do not repeat saturation studies once oxygen is discontinued. Units were not asked to provide data on the percentage of infants ‘passing’ repeat studies after discontinuing home oxygen; it would be interesting to discover if repeat studies after stopping oxygen frequently result in restarting. The current home oxygen supplier, Dolby Vivisol, is now able to reinstall home oxygen concentrators and cylinders within four hours. Current practice of keeping oxygen cylinders at home long after it has been discontinued is therefore likely to be unnecessary.
Conclusion
This survey shows that the management of babies going home on oxygen varies widely between NNUs throughout the UK and internationally. Variations exist in identifying infants to investigate, time of performing the initial pulse oximetry study, the timing and duration of repeat studies and the interpretation of results. Additionally, the use of peripheral investigations such as echocardiography also varies widely.
Few units apply the BTS guidelines in their entirety. This may reflect the age of the current guidelines (nine years old), and the lack of evidence for some aspects of the guideline. There is a need for better implementation of the existing guideline or, preferably, to revisit the evidence base for home oxygen prescribing with a view to developing comprehensive guidance on home oxygen prescribing in neonates with BPD preparing for discharge.
Further work is needed to update current guidelines for the use of home oxygen in infants with BPD. As home oxygen therapy for BPD babies is an important part of long-term management, it should be given priority in neonatal conferences and educational events. Additionally, professional bodies should continue to develop evidence-based, consensus guidelines or position state-ments to guide NNUs to serve babies and families with home oxygen therapy.
Acknowledgement
The authors would like to thank consultant neonatologists Dr Jonathan Coutts, Dr Andrew Powls and Dr Joyce O’Shea for their help in formulating the survey questions.
Patient consent
The authors received consent to publish the photo from the patient’s parents.
Or read this article in our
Tablet/iPad edition
- Practice in home oxygen prescription for infants with BPD varies widely.
- Pre-discharge practice variations include identifying infants requiring a pulse oximetry study and interpretation of results.
- Post-discharge practice variations include repeat pulse oximetry studies and discontinuing home therapy.
