

Practice on timing of first chest radiographs in preterm neonates: a survey of UK neonatal units
Practice regarding routine chest radiography in the assessment of preterm infants admitted to neonatal units (NNUs) with respiratory illness is undetermined. Our study uses a digital survey to evaluate current practices regarding first chest radiograph in preterm infants admitted to NNUs in the UK, which demonstrates a tendency to delay the chest radiograph in infants who make good clinical progress. We review the likely impact of chest radiograph timing on subsequent management and clinical course of preterm neonates with respiratory distress.
Mark RobertsonPaediatric Registrar
Rosemary Abara
Consultant Paediatrician and Neonatologist
rosemary.abara@lanarkshire.scot.nhs.uk
University Hospital Wishaw, Scotland
Robertson M., Abara R. Practice on timing of first chest radiographs in preterm neonates: a survey of UK neonatal units. Infant 2024; 20(2): 41-45.
Respiratory illness is a major reason for admission of newborn babies to NNUs. Assessment of respiratory distress is predominantly clinical, supported by imaging using chest X-rays (CXR). Although respiratory distress syndrome (RDS), is the most common respiratory illness among the preterm population, the prevalence and severity reduce with advancing gestation.1,2 In the late-preterm and term population, the most common causes of respiratory illness are: RDS, transient tachypnoea of the newborn (TTN) and congenital infection. However, other less common causes of respiratory distress include pneumothorax, persistent pulmonary hypertension (PPHN), meconium aspiration syndrome, cardiac failure (secondary to congenital heart disease), trachea-oesophageal fistula (TOF), diaphragmatic hernia and congenital pulmonary airway malformation (CPAM), although this list is by no means exhaustive.3
A plain CXR is a simple and non-invasive investigation that can be beneficial in the assessment of respiratory illness in late preterm and term infants. It can differentiate RDS, TTN and infection based on radiological findings, assisting clinicians to refine their diagnosis and support clinical assessment. Moreover, it can help detect less common pathology, which may not be apparent despite comprehensive assessment of antenatal and intrapartum history, detailed antenatal ultrasound and physical assessment of the infant.4
At present, there is not much medical literature regarding optimum timing and indications for a CXR in preterm neonates admitted to NNUs with respiratory distress. Early screening CXRs have been supported by previous research, suggesting routine screening of neonates with respiratory distress is advantageous for the identification of potential problems before they clinically manifest, although the results did not reach statistical significance.5 However, RDS remains the most likely cause of respiratory distress in a neonate and current practice has evolved such that there is less emphasis on radiograph assessment of RDS and instead, management is determined by degree of work of breathing and the fraction of inspired oxygen (FiO2).6 Similarly, the management of TTN is not significantly influenced by radiological findings.
In this study, we examine the practice of UK NNUs regarding indication and timing of a first plain radiograph in the preterm neonate admitted to an NNU. We consider whether early CXRs are required as routine admission screening or if it is acceptable to delay imaging and perform later if the patient does not progress as clinically anticipated.
Methods
We conducted a digital survey to evaluate current practices of NNUs throughout the UK regarding CXR utilisation for preterm neonates admitted to their facilities. The survey was developed by a consultant neonatologist and paediatric registrar and underwent review by several consultant neonatologists. A copy of the survey can be obtained from the authors on request.
The survey covered domains including:
- NNU demographics
existence of unit guidelines regarding the use of admission CXRs
current practice regarding timing of CXRs in preterm neonates
indicators for urgent CXR
use of lung ultrasound.
Initially, the survey was distributed to all NNUs across the UK by email cascaded though the perinatal networks. Subsequently, we emailed individual unit lead consultants and sent two or three email reminders, to encourage maximum participation. In the event of multiple responses from a unit, only the first response was accepted and subsequent responses from that unit were excluded. In the event we received one response representing the practice of two related units, the response was duplicated, and one response attributed to each of the related units. Several responses had contradictory answers relating to radiograph timing and in such cases, we considered the longest possible wait the unit would permit in our analysis.
Results
Demographics
The overall response rate was 75%, with a total of 133 eligible survey responses received, representing 137 of the 181 NNUs across the UK. Four survey responses each pertained to the practice of two related units. Multiple responses were received from 15 units, but only the first response was considered valid and subsequent responses were excluded. Our analysis is therefore based on the practice of 137 NNUs in the UK.
Out of the 137 eligible responses, 97% (n=133) were completed by consultants. The remaining 3% were completed by a mixture of senior nurses, doctors in training or advanced neonatal nurse practitioners. We received responses from NNUs of all levels, as illustrated in FIGURE 1.
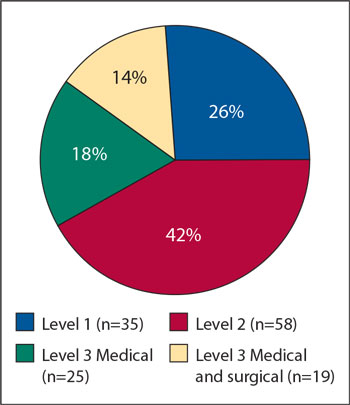
FIGURE 1 Designation of responding NNUs. Level 1=special care baby unit (SCBU); level 2=local neonatal unit (LNU); level 3=neonatal intensive care unit (NICU).
A minority of NNUs (32%, n=44) have a written guideline relating to timing of an initial plain CXR in preterm neonates admitted to the unit. Consequently, we examined ‘typical practice’ followed by NNUs in the absence of explicit guidelines. 89% (n=122) of respondents would expect a nasogastric or orogastric tube to be sited prior to X-ray.
Timing
The timing of the first CXR varies significantly among NNUs (FIGURE 2). Although clinical features will dictate X-ray timing for a specific neonate, we sought to identify common tendencies and preferences in unit practice. Approximately a third (35%, n=47) will perform a CXR within four hours of admission while two thirds (65%, n=90) are willing to hold off for more than four hours from admission, provided the neonate is on minimal respiratory support, weaning steadily with reassuring respiratory parameters. A CXR may not be required if the neonate is on minimal respiratory support with good progress at 29% of NNUs. Therefore 71% of NNUs will, at some stage, perform a CXR for all admitted neonates.
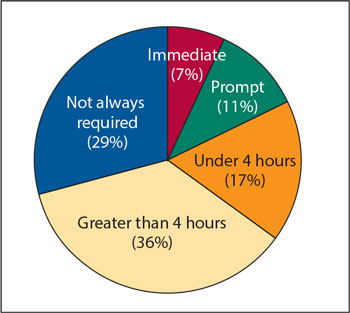
FIGURE 2 Timing of first plain CXRs of neonates admitted to NNUs, based on latest permitted timing. 7% routinely X-ray all preterm neonates immediately upon admission (within the first hour). Nearly a fifth (18%) typically perform CXR promptly (though not necessarily within the first hour). Approximately a third (35%) will perform a CXR within four hours of admission.
Clinical indicators
We additionally sought to compare specific indicators for an early CXR, focusing primarily on objective indicators (FIGURE 3). Our analysis again revealed consider-able variation in practice among NNUs. The most observed indicator for an early CXR in preterm neonates is a deterioration in the baby's clinical condition and a requirement for invasive respiratory support; 86% of NNUs would expect to perform an early X-ray if invasive ventilation is required (FIGURE 3). The FiO2 serves as a ‘hard trigger’ for an early CXR in 48% of NNUs, though thresholds vary (FIGURE 4).
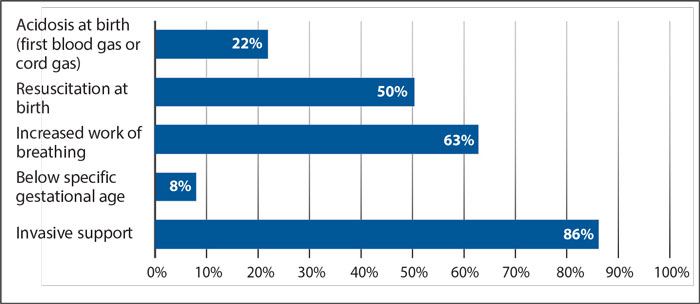
FIGURE 3 Percentage of NNUs arranging an immediate CXR based on specific clinical indicators.
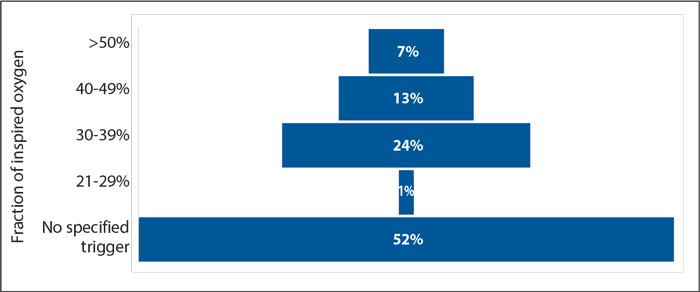
FIGURE 4 Percentage of NNUs arranging an immediate CXR based on specified FiO2. The FiO2 serves as a ‘hard trigger’ in 48% of NNUs (not answered = 3%).
Based on comments and feedback from the survey, there are numerous other possible triggers for performing an early CXR. These indicators typically involve complex clinical judgements accounting for multiple factors including pregnancy and birth history, gestational age, degree of resuscitation required, degree of work of breathing and oxygen requirement.
A rapid change in clinical state or deterioration was frequently mentioned as a trigger for an early radiograph. Other factors include suspicion of congenital defects, suspicion of pneumothorax or diagnostic uncertainty. Finally, a plain CXR would usually be requested if umbilical lines were inserted, however imaging may be delayed until after line insertion, if deemed appropriate based on overall clinical assessment.
Use of lung ultrasound
The preferred modality for initial assessment imaging of preterm neonates overwhelmingly remains the plain CXR. A lung ultrasound scan (LUSS) may be used as a component of the initial assessment in just 15% of units. LUSS is only common practice in 3%; a further 12% of units may use LUSS at the clinicians’ discretion. Despite the increasing utilisation of LUSS, the majority (95%) will either rely solely on plain CXRs or require one, even where LUSS has been performed.
Discussion
Our findings highlight the considerable variability in approach among NNUs, with only a third of units utilising written guidelines. This is perhaps reflective of the significant inter-patient differences observed within the preterm neonatal population. This population is highly heterogenous, encompassing infants as early as 22 weeks’ gestation and weighing under 500g, to infants born at 36+5 weeks’ gestation and weighing more than 3,000g. Furthermore, the reasons for an infant’s admission to an NNU are diverse and may not be due to signs of respiratory distress. Considering these factors, it becomes challenging to develop an effective and sufficiently detailed guideline that can accommodate the wide range of possibilities in clinical practice. Any guidelines produced must have a narrow scope of application. Consequently, reliance is placed on clinical experience and judgement rather than protocol.
The most notable finding in our results is the willingness of many NNUs (two thirds) to delay performing a CXR for up to or over four hours, provided the neonate is on minimal respiratory support and making good progress. Clearly, such decisions are made on an individualised basis and account for factors such as antenatal history, mode of delivery, oxygen requirement, degree of respiratory distress and clinical course. For any given neonate, the clinician must consider the working diagnosis and likely differentials to determine a safe and effective individual-ised management plan. Ultimately, the questions clinicians must ask themselves include:
- What diagnosis am I most worried about and how will a CXR alter management?
- What are the likely differential diagnoses? Will a CXR help differentiate them?
- If I delay a plain CXR, what are the principal risks to the neonate?
RDS
RDS is the most common cause of respiratory distress in preterm neonates and can be identified on a plain CXR.7 However, European consensus guidelines state that treatment is determined based on specific clinical indicators and these guidelines do not include CXRs as a necessary component of assessment.6 Considering that the prevalence and severity of RDS is inversely proportionate to gestational age,1 RDS can be a reasonable working diagnosis in very preterm and extreme preterm infants presenting with signs of respiratory distress. In such cases, early imaging is unlikely to significantly alter the initial management approach. Therefore, there is no specific requirement for an early CXR for the purpose of diagnosing RDS, though our findings suggest between 33% and 41% of units would arrange a plain CXR. This figure is, however, confounded by contributing indications for imaging such as assessment of line and endotracheal tube (ETT) position or exclusion of pneumothorax. In cases requiring intubation for ventilation prior to surfac-tant administration, it is advantageous to perform a CXR to ensure proper ETT placement and reduce the risk of unilateral/asymmetrical surfactant administration.
In contrast, the probability of RDS in a late preterm infant is comparatively lower and an early CXR may be beneficial to address diagnostic uncertainty. It is worth noting that while radiographic identifi-cation of RDS in the late-preterm population may provide a diagnosis, it may not necessarily lead to altered treatment as the safety and efficacy of surfactant administration in late-preterm babies remains unclear.8 These multiple competing considerations are illustrated in our findings, with 38% of units commenting that decisions on timing of first CXR are complex and based on an interplay of various clinical factors, including the need to address diagnostic uncertainty.
TTN
TTN is another major differential diagnosis for infants with respiratory distress and can be diagnosed based on a plain radiograph,7 although correlation between neonatologist and radiologist image analysis is limited, with only 48% concordance demonstrated in one study.9 TTN is usually apparent within the first two hours of life and is most prevalent in late-preterm and term neonates. The natural history of TTN involves resolution with time and supportive care, although this can frequently take up to 72 hours. TTN is a variation of ‘delayed transition’, which persists beyond the typical 4-6 hour resolution time. Significantly, management of TTN is not directly altered based on radiographic findings and indication for respiratory support is based predominantly on clinical assessment, including work of breathing and oxygenation. Therefore, delaying initial radiographs by around four hours may reduce unnecessary imaging of babies with simple delayed transition. Imaging could be fully avoided if respiratory distress makes significant improvements or fully resolves, as is the practice in 29% of UK NNUs. If respiratory distress persists beyond the window of ‘delayed transition’, then a radiograph may confirm TTN and exclude other important differentials.
Congenital infection and pneumonia
Although slightly less common, congenital infection and pneumonia, should not be overlooked. Serious infection in a preterm neonate often presents with non-specific or subtle signs, and respiratory distress is a relatively frequent manifestation.10 Therefore, early identification and treatment and a low index of suspicion is crucial for ensuring the wellbeing of all neonates. Distinguishing between infection/pneumonia from delayed transition based solely on clinical findings alone is challenging. In an otherwise healthy late-preterm baby, it may be reasonable to wait around four hours to see if symptoms resolve, indicating delayed transition. If symptoms persist, then it would be prudent to proceed with imaging and blood investigation with empirical antibiotic cover. Very preterm and extremely preterm babies are, however, very vulnerable to infection, which further increases the risk of chronic lung disease and, in this population, it would be advisable to commence antibiotics without delay. Some units perform an immediate or prompt CXR (FIGURE 2), which may facilitate antibiotic initiation a few hours earlier, though this is unlikely to have a significant impact on the clinical course of an otherwise well neonate.
Congenital anomalies
CXRs are particularly useful for identification of congenital anomalies, including TOF, congenital diaphragmatic hernia (CDH) and CPAM. Of these, the most time sensitive is probably CDH. Around half of cases are diagnosed antenatally, and an early confirmatory CXR is beneficial.11 Non-invasive ventilation (NIV), a mainstay of supportive management of respiratory distress in most preterm babies, should be avoided in cases of CDH due to the risk of inflation of herniated bowel contents, thus further reducing ventilatory effectiveness.12 Intubation is instead indicated if respiratory support is required. More severe cases are likely to be diagnosed antenatally, whereas milder cases may not be identified until after birth based on symptoms of respiratory distress with asymmetric chest auscultation findings. Delaying a CXR in a neonate with respiratory distress may lead to initiation of NIV in a neonate with CDH, potentially resulting in bowel inflation.
Postnatally identified CPAM will usually be picked up due to clinical signs of respiratory distress and is readily identifiable on a plain CXR. If the neonate is symptomatic, then surgical resection may be indicated, with urgency determined by clinical severity. Therefore, while a CXR may be important to obtaining the diagnosis, the urgency of the CXR is determined by the severity of respiratory distress, which in turn determines urgency of intervention. In an unwell neonate, an early radiograph is clinically warranted to reach a diagnosis to ensure treatment is appropriate. In a relatively well neonate, imaging could be delayed for several hours without altering the overall clinical course.
TOF is relatively rare with an incidence of around 1 in 3,500 births.13 Approximately a third of cases are diagnosed antenatally and the remainder are diagnosed postnatally.14 Presenting signs include respiratory distress, excessive secretions and choking when feeding. Absence of a gastric bubble on a CXR in a neonate with appropriate symptoms increases suspicion, though is not diagnostic as a gastric bubble may be present due to a distal fistula. The most useful test for initial assessment is therefore a plain radiograph with a nasogastric (NG) or orogastric (OG) tube in situ. The NG/OG tube will be unable to pass to the stomach and will instead curl in the oesophageal pouch. The authors consequently support the practice of routinely placing an NG/OG tube in any preterm neonate with signs of respiratory distress prior to performing the first CXR, as this is an effective method of excluding or identifying TOF. Using an NG tube has the additional bonus of excluding complete choanal atresia which, while not identifiable on a plain CXR, can cause signs of respiratory distress. Our findings reassuringly demonstrate that placing an NG/OG tube prior to CXR is standard practice in 89% of NNUs.
LUSS
Although the primary aim of this research was to understand practice regarding timing and indication for plain CXRs for preterm neonates, we also briefly examined lung ultrasound practice. LUSS is increasingly recognised as a useful tool in the rapid bedside assessment of neonates with respiratory distress.15 Our findings demonstrate that LUSS is still infrequently used in this population. It is only used in 15% of NNUs and is routine practice in just 3%. Of those utilising LUSS, 65% would still expect to perform a CXR to confirm findings. These results demonstrate that while there is interest in using lung ultrasound, CXRs remain the major imaging modality for preterm neonates. Our research did not investigate the reasons for the limited use of LUSS.
Limitations
We acknowledge that a digital survey is a relatively blunt tool to examine the breadth of possible scenarios in a NNU, however we feel it adequately identified the key components to decision making regarding the performance of admission CXRs. Question design unfortunately created the possibility for conflicting answers (ie a unit stating they usually perform a radiograph promptly, but also could be willing to delay >4 hours). We addressed this by considering the longest a unit is willing to wait, as a clinician will always be justified in performing imaging early due to clinical concerns. Individualised care requires nuanced decision, which is less accurately captured using such a survey. However, we believe the general approaches used by NNUs have been identified. We also acknowledge that by asking for one response per unit, we may capture an individual clinician’s opinion rather than that of the unit as a whole, even though we did request responses to be representative of the unit and the survey was directed to lead consultants who shape unit practice.
In summary
There is considerable variation in practice between UK NNUs in terms of timing and indication for admission CXRs in preterm neonates. The major theme through our results was the importance of complex clinical judgements encompassing factors including gestation, birth, history, degree of respiratory distress, FiO2, diagnostic uncertainty and to assess line/tube position. This study demonstrates for the first time that it is common practice in UK NNUs to delay CXRs beyond four hours after admission in preterm neonates who are on minimal respiratory support and making good progress. However, earlier radiographs may be clinically indicated. It also demonstrates that nearly a third of NNUs will in some cases avoid performing a CXR in preterm neonates that make good clinical progress. This practice reduces unnecessary imaging of preterm neonates but does risk delayed diagnosis of less common conditions and congenital anomalies in particular. However, it is not likely to expose neonates to significant avoidable harm as radiographs should still be performed earlier if clinically indicated and in those demonstrating persisting respiratory distress.
Author contributions
RA was responsible for the study concept and study design, with contribution to the editing of this manuscript. MR contributed to the study design and was responsible for implementation, data analysis and writing this manuscript.
Or read this article in our
Tablet/iPad edition
- There is considerable variation in practice regarding timing of a first chest radiograph in preterm neonates.
- 65% of NNUs consider it acceptable to delay a chest radiograph by over four hours, if clinically appropriate.
- 29% of NNUs will consider discharging a preterm neonate with resolved respiratory distress without having a chest radiograph.
- Just 32% of NNUs have a written guideline on timing of a first chest radiograph.
Also published in Infant:
