

Developmental dysplasia of the hips – what are we missing?
Developmental dysplasia of the hips (DDH) is one of the conditions screened for in the UK as part of the Newborn and Infant Physical Examination (NIPE) screening programme, however not all cases are detected. We reviewed the electronic records of 286 children attending the dedicated DDH clinic at a tertiary referral centre over a three-year period to identify the proportion of children diagnosed outside of NIPE screening and to compare these children to those diagnosed through screening. In addition, we explored the current literature pertaining to the practice of DDH screening.
Jake WrightPaediatric Trainee
jake.wright@nhs.net
Aoife Hurley
Neonatal GRID Trainee
Rachel Toone
Neonatal Consultant
Leeds Teaching Hospitals NHS Trust
Wright J., Hurley A., Toone R. Developmental dysplasia of the hips – what are we missing? Infant 2024; 20(2): 55-58.
Background
Developmental dysplasia of the hips (DDH), previously known as congenital dysplasia of the hip, is a musculoskeletal condition where there is abnormal development of the acetabulum with or without hip dislocation. It is a spectrum of disease that can range from mild dysplasia through to more severe dysplasia with instability. This is not always present from birth and therefore can be picked up at any time in childhood.1,2 The incidence of DDH varies but it is thought to be between 0.5-3 per 1,000 live births. 1,3 It is important to diagnose and treat as early as possible in an attempt to prevent long-term complications, which include persistent dislocation and early osteoarthritis.1,2 If DDH is detected early and treated, there is the opportunity for normal hip development and function by the time the infant is an adult, without the need for surgery.3,4 There is no agreed definition of a late diagnosis of DDH with variation in the cut off from six weeks to 20 months of life at the time of diagnosis.5,6
To facilitate early diagnosis in the UK, DDH is one of the conditions included in the Newborn and Infant Physical Examination (NIPE) screening programme. This consists of an examination and review of risk factors shortly after birth (the ‘newborn’ examination) and a similar physical examination at 6-8 weeks of age performed by the general practitioner (the ‘infant’ examination). Current NIPE-recognised risk factors for DDH include breech presentation from 36 weeks regardless of presentation at delivery, breech presentation at delivery from 28 weeks, or a first degree relative with DDH. Suggestive clinical findings include positive Ortolani or Barlow’s test, limited abduction and leg length discrepancy. An infant is deemed screen-positive if they have suggestive examination findings or risk factors and these infants should be referred on for further assessment with an ultrasound scan. ‘Clicky’ hips are not part of the NIPE risk factors and are reviewed at local level – at our centre, patients found to have clicky hips at the newborn examination are referred for further investigation based on previous local audit work. 7
Unfortunately, some infants with DDH are not identified by the NIPE screening programme. It is known that patients diagnosed late are more likely to require surgical intervention. This leads to a more arduous patient journey, due to more invasive treatment and hospital admission, as well as an increased financial cost of care. It proves difficult to accurately identify the exact cost of treating a patient diagnosed late due to several different factors including differing definition of late diagnosis and quantifying all of the costs involved in patient care, such as staff time. Some groups have estimated that it ranges between 1.3 and 3.5 times more than those diagnosed early. 8-10
Aims and methods
We set out to quantify and qualify the proportion of infants treated for DDH that were identified outside of the NIPE screening programme, as well as looking at how this group compares to those detected through screening.
We carried out a retrospective review of electronic patient records of all patients attending a clinic for DDH-related referrals at a single regional referral centre over a three-year period (01/08/2018 to 31/08/2021). Patients that ultimately did not require treatment for DDH or had other conditions that could potentially cause hip pathology, including neuromuscular disease, were excluded.
Data collected included the patient’s date of birth, the date of referral to clinic, the source of referral to clinic (categorised as newborn examination, infant examination or other), the date of diagnostic investigation, and the definitive treatment of the child (categorised as Pavlik harness, surgical treatment, or other). Surgical treatment was defined as any procedure requiring a general anaesthetic or theatre time. The age at diagnosis was calculated as the number of days from the date of birth to the date of clinic referral, if this was unavailable then the date of diagnostic investigation was used. Children diagnosed through either the newborn or infant examination were labelled as ‘screening diagnosed’ and those diagnosed through other routes were labelled as ‘non-screening diagnosed’.
The proportion of non-screening diagnosed infants was calculated from those born over a one-year period (August 2018 to August 2019). This period was selected as it predated the COVID-19 pandemic, which had a significant impact on the provision of DDH screening in the UK.
Results
Over the review period, 286 patients who underwent treatment for DDH attended the BABYHIP clinic. Of these patient records, 265 had data quality acceptable for use in our review. Of these patients, 206 (77.8%) were diagnosed through the NIPE screening programme with the remaining 59 (22.2%) being diagnosed through other routes. 72 infants included in the cohort were born between August 2018 and August 2019. In this group, 58 (80.6%) were diagnosed through screening and 14 (19.4%) were diagnosed outside of screening.
Patients identified through screening were diagnosed at a younger age than those diagnosed through other routes (screening diagnosed median age at diagnosis = 48 days, non-screening diagnosed median age at diagnosis = 369 days). Non-screening diagnosed patients presented over a broad age range (19-1,464 days); however, the majority (71%) presented within 18 months of life (FIGURE 1).
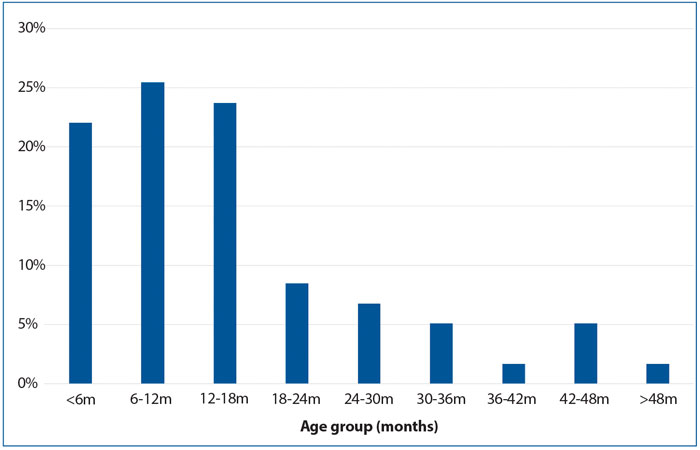
FIGURE 1 A graph to show the proportion of non-screening diagnosed children within each age group (n=59).
Of the screening diagnosed patients, 192 (93.2%) were identified at the newborn examination and 14 (6.8%) were identified at the infant examination. Of the non-screening diagnosed patients, the reason for presentation was unclear from the available records in 11 cases (18.6%). Where this information was available, many had an abnormal gait (38.9%) or limb length discrepancy (38.9%) at the time of presentation. In several cases children presented with both. Four (6.8%) cases were identified incidentally through investigations performed for other reasons, such as accidental or non-accidental injury (FIGURE 2).
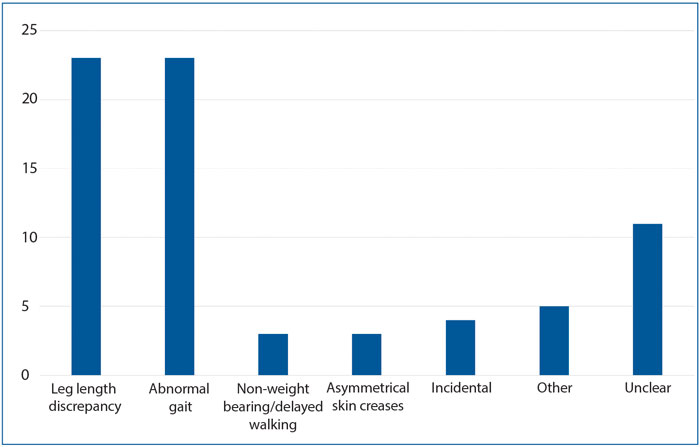
FIGURE 2 A graph to show the number of non-screening diagnosed children presenting with each clinical sign (n=59).
Screening diagnosed patients were more likely to be definitively managed with a Pavlik harness (87%) than surgically (12%). However, non-screening diagnosed patients were more likely to be definitively managed surgically (85%) than with a Pavlik harness (11%). The percentage of patients treated surgically increased with age at presentation, with the vast majority (93%) of children diagnosed over the age of approximately four months requiring surgical treatment (FIGURE 3). For two records the definitive treatment was unavailable and for two patients, further treatment was inappropriate due to
co-morbidities.
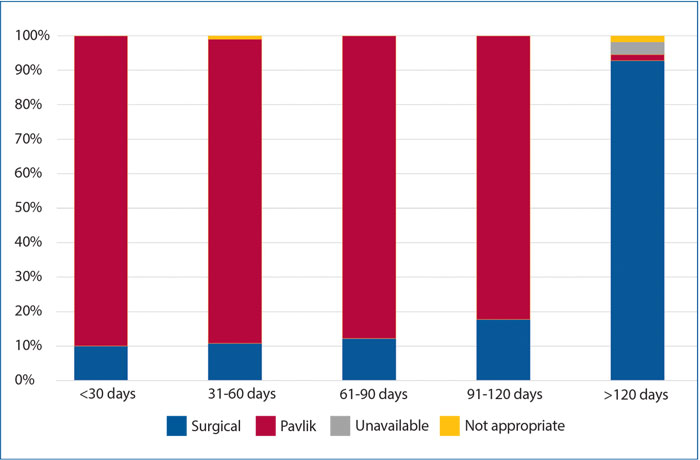
FIGURE 3 The effect of age at diagnosis on management across the whole cohort (n=265).
Discussion
Within this cohort we found that approximately one in five children requiring treatment for DDH were not diagnosed through the NIPE screening programme, as they did not have either a positive screening examination or risk factors warranting an ultrasound scan, and were diagnosed much later than those identified through screening.
We were unable to find other studies that specifically looked at the proportion of children identified outside of NIPE screening, but there have been a handful of studies looking at the incidence of late diagnosis of DDH. However, there is variation in the estimates, which may be in part due to different definitions of late presentation and what constitutes pathological hip development. A review of all children born in Northern Ireland over a two-year period found an incidence of DDH requiring treatment diagnosed after one year of age of 0.42 per 1,000 live births.4 However, a large database review of children in England diagnosed with DDH between 1990 and 2016 found an incidence of diagnosis after one year of age of 1.28 per 1,000 live births.11 Lastly, a review of children born over a 15-year period showed an incidence of irreducible hip dislocation diagnosed after the age of three months of 0.28 per 1,000 live births.5
Within our cohort, infants that were not identified through screening were much more likely (approximately seven times likely) to require surgical intervention than those who were, which is consistent with other studies.12 This is likely because those not diagnosed through screening are diagnosed at a later age (321 days, or approximately 10.7 months) and the need for surgical intervention is more likely with increasing age.13 The most clinically relevant definition of what constitutes a late diagnosis of DDH may well be one at an age beyond which non-surgical treatment is unlikely to be possible – based on our data this would appear to be at around four months of age.
We are limited in the conclusions we can draw from our cohort as this only represents the experience of a single centre and this may vary across the country. In addition, the data collected are subject to the quality of the medical records, which can be variable. However, we feel with such a high proportion of infants not being identified through screening and the importance of early diagnosis in reducing the need for surgery, this raises questions about the adequacy of current screening for DDH in the UK.
There is currently no international consensus regarding the optimum method of DDH screening as each option presents its own challenges. As previously described, the UK currently employs an approach of selective ultrasound scanning based on a combined assessment of clinical examination and risk factors – such a system is similarly utilised in the USA.14 The clinical examination performed at the newborn and infant examinations consists of the Ortolani and Barlow manoeuvres, which attempt to identify a dislocated and dislocatable hip, respectively; however, they are quoted to do so with only a sensitivity of 62-65%.15,16 This sensitivity may also vary based on the experience of the examiner, with more experienced examiners being more likely to detect abnormality. 6,17,18 In the UK, the newborn examination will often be completed by relatively junior members of the medical team that may have only limited experience in performing it. Lee et al19 found that having all newborn examinations performed by a smaller number of regular examiners, who had completed specific training, allowed for consolidation of experience and led to a marked improvement in detection (96% sensitivity compared to 74%).19 However, it is worth noting that regardless of experience, clinical examination alone is still likely to miss a significant proportion of cases.20 The examination finding of clicky hips deserves special mention as it is specifically discussed in the NIPE handbook, which acknowledges the debated significance of a clicky hip and that the finding could solely arise from examination technique. The NIPE handbook concludes that it should not necessitate referral for further investigation but may be considered.7 However, DDH has been shown to be as prevalent in those found to have clicky hips as in those who were in a breech presentation.1,3,19 Therefore, the routine investigation of infants with clicky hips may be a pragmatic approach to improve early detection given the variation in examination technique and experience among examiners in most UK hospitals.
The risk factors utilised in the NIPE screening programme have previously been listed, however infants presenting late with DDH have frequently shown an absence of these.6,7,21,22 Current recommendations in Canada are to not provide selective ultrasound scanning to infants based on risk factors alone; it is suggested that this group could be more frequently examined.18 The commonly utilised risk factors do not comprise an exclusive list of all features that have been shown to potentially put infants at risk of DDH. Other factors include female sex, talipes, Caucasian ethnicity, delivery via caesarean section, first born infants, oligohydramnios and higher birth weight.1,2,23,24 Perhaps the expansion of risk factors prompting referral for further investigation may present an avenue to reduce late presentation but this would require more evidence to identify those of most utility.
Universal ultrasound scan screening may appear to represent a promising alternative, which has been taken up in countries such as Germany and Austria, but evidence remains equivocal. While studies have shown a trend towards increased sensitivity when compared to selective ultrasound scan screening, it has not been shown to be statistically significant – although this may be difficult to do given the necessary power required to demonstrate an effect in such a rare disease.25,26 What has been consistently shown is that universal ultrasound scan screening does not eliminate late presenting DDH but does significantly increase the treatment rate, in some circumstances to 40-70 times the expected prevalence of DDH, potentially treating cases of mild deformity that would likely resolve spontaneously.16,25,27-29 Although treatment with a Pavlik harness carries significantly less risk than surgical intervention, it is not entirely benign and the risk of iatrogenic harm (such as avascular necrosis or femoral nerve palsy), in addition to the financial cost and labour requirement, must be taken into account if universal ultrasound screening is to be considered.
In summary, when considering what’s missing from DDH screening, further work is needed to learn more about why children present late or outside of screening. We should try to identify common themes or factors that could improve the sensitivity of screening without compromising specificity. One such factor that could be utilised is clicky hips, which appears to be frequently associated with DDH even if this may be due to the wide-ranging experience of examiners. Universal ultrasound screening may reduce the incidence of late DDH but is not without its risks to patients and also has financial implications.
Or read this article in our
Tablet/iPad edition
- One in five children treated at our centre for DDH were diagnosed outside of screening, with an average delay in diagnosis of 10.7 months.
- In our population, children diagnosed later than four months of age were much more likely to require surgical intervention.
- Selective ultrasound screening is limited by the sensitivity of the risk factors used and their detection by the examiner.
- Universal ultrasound screening may reduce the number of late presentations but does not eliminate them completely and may lead to increased financial and labour costs as well as over treatment and an increased risk of iatrogenic harm.
Also published in Infant:
