

Non-attendance of patients to the BCG vaccination clinic: a multifactorial conundrum
Historically, if a newborn baby was considered to be at high risk of coming into contact with tuberculosis (TB), the neonatal Bacillus Calmette-Guérin (BCG) vaccination was offered prior to discharge home. This process was halted with national effect in September 2021. Instead, those babies identified as eligible are now given the vaccine at about 28 days of life, thus necessitating care providers to instate new methods for recalling patients and administering the BCG. We have conducted a service review of the Leeds BCG clinic to expose barriers to patient attendance and bolster the poor recall rates seen within this vulnerable population group.
Kate Parmenter
ST4 Paediatric Trainee
kate.parmenter@nhs.net
Rachel Toone
Consultant Neonatologist
Leeds Neonatal Service, Leeds General Infirmary
Parmenter K., Toone R. Non-attendance of patients to the BCG vaccination clinic: a multifactorial conundrum Infant 2023; 19(2): 63-67.
Background
Prior to 1 September 2021, the neonatal Bacillus Calmette-Guérin (BCG) vaccination was offered to all patients before discharge from hospital, if they were considered to be at high risk of coming into contact with tuberculosis (TB). Those neonates designated at high risk were categorised by one of three requirements:
- Babies whose parents or grandparents were born in a country where the annual incidence of TB is ≥40 per 100,000
- Newborn babies living in areas of the UK where annual incidence of TB is ≥40 per 100,000
- Babies that are in close contact with someone with infectious TB.1
The BCG vaccine is not part of the routine childhood immunisation schedule and thus opt-in by nature. This live attenuated vaccine provides up to 80% protection against the most severe forms of disseminated TB infections, such as meningitis, for up to 15 years. Mortality from TB meningitis exceeds 30% of cases with catastrophically life-changing neurological or sensory sequelae in over half of those patients that survive.2,3
In 2020, the World Health Organization (WHO) cited eight countries whose cumulative burden equated to two thirds of the global total. Primary of these was India, followed by China, Indonesia, the Philippines, Pakistan, Nigeria, Bangladesh and South Africa.4 The UK Health Security Agency (UKHSA) is committed to meeting the WHO TB elimination targets by 2035.5 Leeds and its surrounding neighbourhoods offer a large and fantastically diverse cultural and ethnical population, meaning a high proportion of our babies are eligible for the BCG.
In September 2021, the process of giving the BCG vaccination prior to discharge was halted with national effect, while six areas of the UK (Manchester, Birmingham, Sheffield, Newcastle, London Great Ormond Street Hospital and London Southeast Thames) evaluated the addition of screening for severe combined immunodeficiency (SCID) to the routine newborn bloodspot screening test at five days of age. The effect of this decision was to move giving the BCG vaccination prior to discharge from hospital, to when a SCID screening outcome would be available, namely by 28 days of life. Thus, prompting the need for care providers to instate new methods of recalling and administering the BCG to eligible neonates.
Objectives
To ascertain the factors affecting non-attendance rates of families invited to the BCG clinic by the Leeds Neonatal Service, with attention to socioeconomic determinants of health, parental voices and priorities, and potentially modifiable institutional barriers to executing the care requirements of our population.
There is scope to improve the experience of our families not only when attending the BCG clinic specifically, but also to learn valuable lessons that can influence attendance rates to wider paediatric outpatient clinic settings.
Methods
We collected retrospective data for all BCG eligible patients born into the Leeds Neonatal Service between 1 November 2021 and 31 December 2021. Babies were excluded if they lived in other regions not covered by the Leeds screening team. Six babies were excluded for the following reasons:
- two babies could not attend the clinic due to significant maternal health issues in the postnatal period
- three babies were not suitable for receiving the BCG vaccine due to poor health/prematurity and requiring care on the neonatal intensive care unit
- one baby was excluded because of maternal HIV viral load at the point of delivery (requiring investigation into transmission of the retrovirus).
We recovered 378 eligible patients over the specified three-month period that required a BCG vaccine after the 28th day of life using a combination of databases namely, the Newborn and Infant Physical Examination (NIPE) IT system, SMaRT4NIPE (S4N), and BadgerNet.
The cohort was then examined to find out which of these patients failed to attend their outpatient appointment by the third attempt. We categorised those that did not attend the first or second appointment but did attend the third appointment, as a successful interaction with the service. For these patients, we collated information on ethnographic, socioeconomic and demographic determinants of health as well as parental contact details to use when attempting to contact families.
Using the trust-approved telephone interpretation service when required, parents were contacted to complete and discuss a questionnaire exploring factors influencing clinic non-attendance. Trends were then identified on analysis of these responses. We also checked to see whether parents had been approached while still an inpatient and informed about the indication to attend the BCG clinic, whether information was provided in the most accessible language, and whether they received a reminder text prior to their designated appointment.
Results
378 babies were eligible for a BCG vaccination and 317 were offered an appointment. Of the 378 babies eligible for a BCG, 115 (30.4%) did not receive the BCG. We looked at the processes that led to these patients not receiving a BCG vaccine and discovered several mechanisms of action. Of the 115 patients that did not receive the vaccine, 61 were ‘missed’ at the NIPE screening stage (TABLE 1).
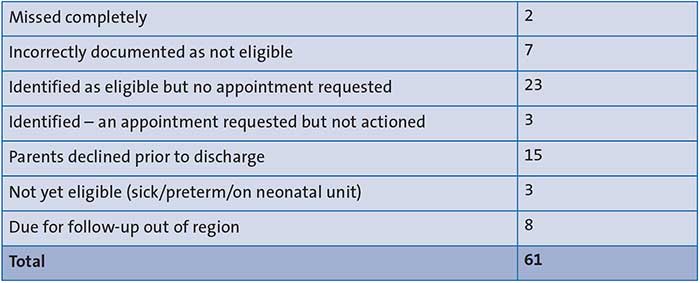
TABLE 1 Examination of the cohort in non-receipt of BCG: BCG screening at the time of the Newborn and Infant Physical Examination (NIPE) screen.
Of the 115 that did not receive a BCG, in 35 (30%) cases this was simply because the parents did not know their child needed one due to a failure in categorisation of patients or administrative processes in booking the required appointment. We have since looked into these avenues and have rectified processes accordingly.
Of the 263 patients that attended for a BCG vaccine (TABLE 2), only 89 patients (34%) attended their initial designated appointment. Over half (56%) did not attend until their final appointment invitation, even after a text reminder. If the family did not attend the clinic for the third appointment, a letter was issued to the family and their GP explaining that no BCG had been given and, if this is required in due course, they should contact their family practitioner.
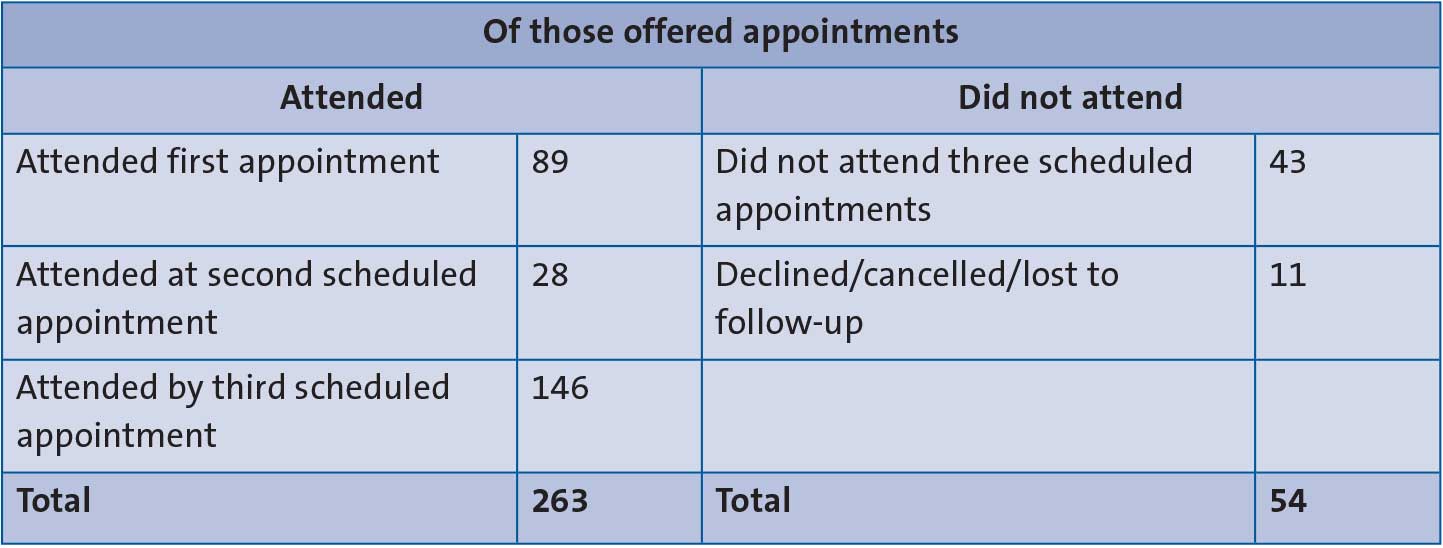
TABLE 2 Examination of the cohort offered an appointment (n=317).
Of the 317 that were offered an appointment for BCG vaccination, 54 did not attend any of the three scheduled appointments (TABLE 2). Eleven of these declined their appointments or were lost to follow-up. We collated information on ethnographic, socioeconomic and demographic determinants of health for the 43 eligible babies and attempted to contact their families. The demographics for the cohort can be seen in TABLE 3. Two parents declined to be questioned and 12 could not be contacted for the following reasons:
- one family had returned to the country of origin
- seven did not answer on three separate attempts
- four telephone lines were no longer in use and no other contact details were available.
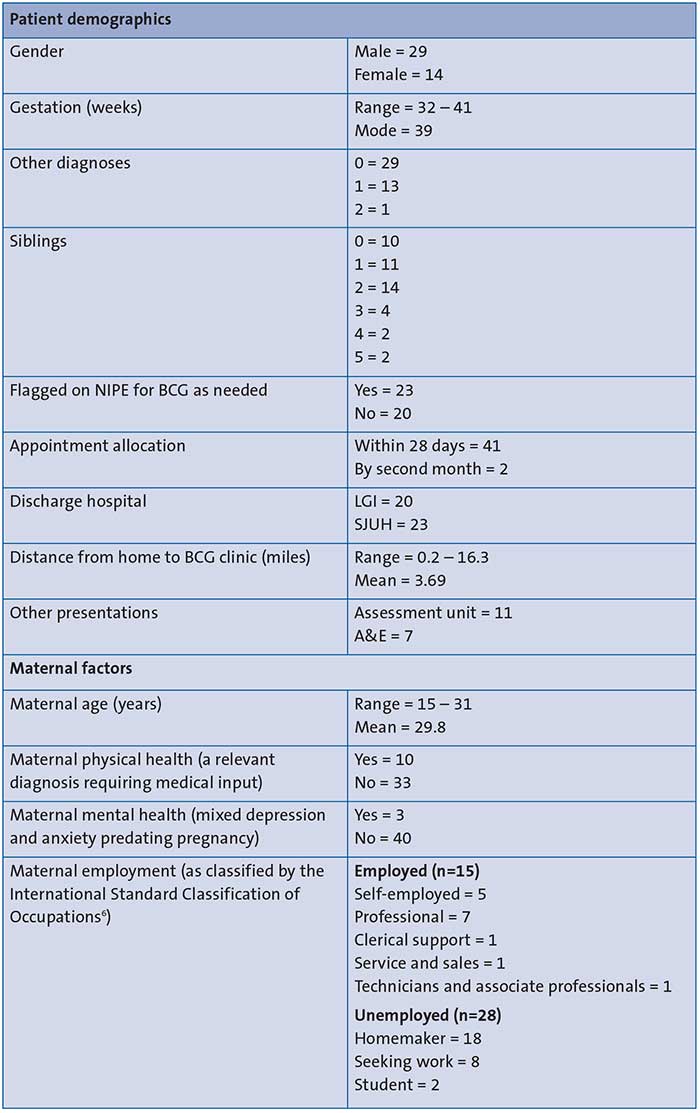
TABLE 3 Baby and mother characteristics informing the social and ethnographic context of the cohort (n=43). Key: LGI=Leeds General Infirmary; SJUH=St James University Hospital.
Therefore, we were able to collect qualitative data for 29 patients that qualified for this study.
Postcode as a proxy for deprivation index
England’s ministry of housing produces a deprivation index for every area in Britain. Ranking occurs using a postcode to produce a relative deprivation index. A deprivation score of 1 means the area is among the 10% most deprived areas in England; a score of 10 means the area is among the 10% least deprived areas in England. The index includes data such as: average income of the area, crime rates, educational attainment, disability rates, housing conditions, access to public services and more.7 Using the NHS West Yorkshire Health Care Partnership post-code evaluation tool, we identified the deprivation decile of our patients (FIGURE 1).8 Staggeringly, 58% of our study population lived in the top two most deprived deciles.
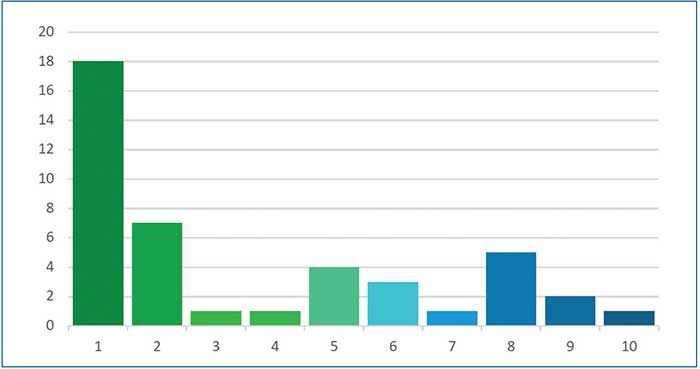
FIGURE 1 Postcode deprivation decile distribution on a scale of 1-10, where 1 = most deprived and 10 = least deprived (n=43).
Distance from the clinic
Twenty-three of those that did not attend the BCG clinic lived within three miles of the facility. Of this number, 11 lived within a mile radius, 10 within two miles and two up to a boundary of three miles surround-ing the clinic location.
Language and ethnicity
The evaluation encountered 12 languages (FIGURE 2). Surprisingly over half of the mothers were denoted as English speaking, however, only four mothers (out of 29) had an ethnicity identifying them as British.
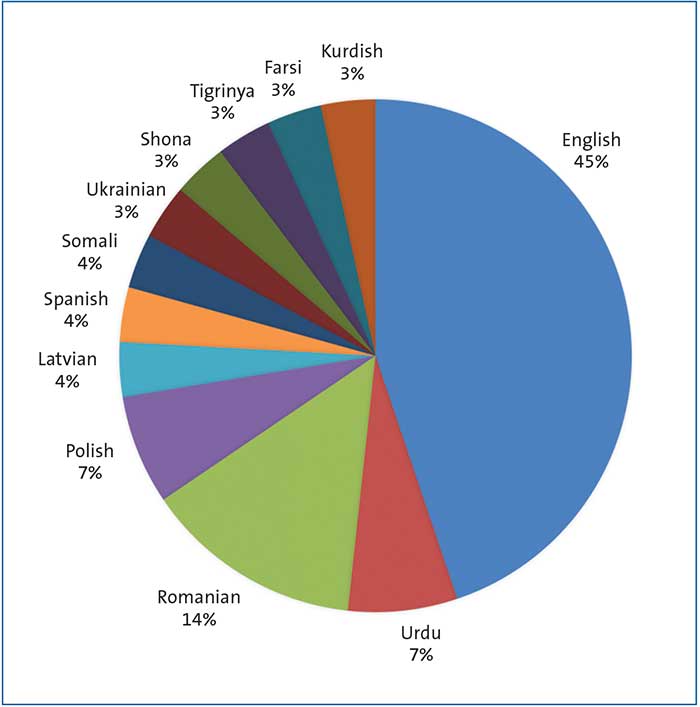
FIGURE 2 A breakdown of the primary maternal languages represented in the parent telephone interviews (n=29).
Of the 13 mothers listed with English as their first language, on contact by telephone:
- four mums needed no assistance
- two managed to converse without an interpreter but did struggle to convey some themes
- seven needed interpreter services.
In the 16 mothers where English was not listed as a first language, 13 needed an interpreter.
All four Romanian mothers needed an interpreter and the interpreting service often struggled to communicate with them and relay information between parties.
We had two refugee/asylum seeking families in our cohort (Somalian and Ukrainian).
Mode of transport non-attenders would have utilised
In the telephone interviews, we discussed the mode of transport that clinic non-attenders would have used had they attended:
- 13 families reported they would have travelled by car
- 1 would have walked
- 5 would have used a taxi
- 10 would have taken a bus (or buses).
Of the 13 families that would have used a car as their mode of transport, only three mothers would confidently drive themselves to the clinic 28 days after birth. Two could drive but would have preferred someone else to take them due to anxiety (parking/traffic/too much pressure with a newborn baby). Eight could not drive and were dependent on the availability of others for their journey to the clinic. Eleven of the non-attending families interviewed commented that parking arrangements posed a barrier to them deciding to come to the clinic. Most families opted to park on off-site parking as they did not know about the on-site multi-storey car park. All families mentioned cost of parking as a negative factor and the lack of mother and baby spaces.
Ten families would have to have come by bus. Of these, six required two or more buses to make it to the clinic, which is understandably challenging with a newborn baby. Eight said that poor weather would negatively impact on them travelling to the clinic with a newborn. Seven mothers commented that bus fares are getting more expensive and need to be weighed up against other childcare considerations. All would have ideally chosen to come by taxi or car if this mode had been accessible.
The parental perspective
It is clear that we need to listen to our parents if we want to improve the clinic attendance rates (FIGURE 3). We have gained a wealth of insight into what our families need from us so they can bring in their babies safely and without compromise. They have, rightfully so, a set of realistic expectations for us, the service providers.

FIGURE 3 Insight generated from parent telephone interviews.
There are a few quick fixes such as updating our information sheets so details of where to find our car parks are much clearer, and providing all information in an appropriate language and format (FIGURE 4). We can fine tune our health informatic and administrative systems and we must restructure the clinic times so we provide more accessible opportunities.
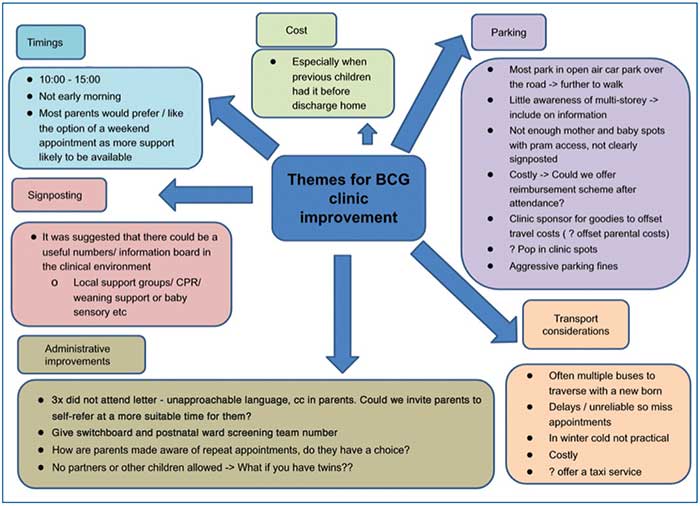
FIGURE 4 The themes raised by this study for improving the BCG clinic.
These families are debating much more than just getting to the clinic. With escalating heating and food costs there are priorities to be met and extra transport costs and suboptimal parking facilities weigh heavy on these decisions. We need to think about what we are asking of our new mums and their young babies; travelling on multiple buses in winter is not feasible.
Some parents expressed concerns about COVID-19 in a potentially more high-risk area and this deterred them from presenting to the clinic due to perceived harm for their child.
We need to consider a rapid system of reimbursement for travel. This will incentivise families but will also ensure that the extra costs associated with moving the timing of the BCG to 28 days of life will not impact negatively on family budgets.
Conclusion
Attendance rates to outpatient BCG clinics across Leeds are suboptimal following the government incentive to move vaccination to after the 28th day of life, as opposed to the previous model of offering a vaccination prior to discharge. While we have clear areas to address in order to improve the new administrative processes, we are currently trailing in getting patients to the BCG clinic – we will act on the patient voices we have heard here.
We expect the Leeds experience to be generalisable to the situation experienced nationally and this is a cause for concern. We have seen an incremental rise in the rates of TB in recent times, indeed a rise of 2.9% was presented in the Tuberculosis in England report in 2021.5 The effects of this policy change will no doubt become clearer over coming years. The discussions generated here are generalisable to the wider paediatric outpatient clinic environment with the patient voice telling us what we need to do to facilitate their attendance.
We hope this small-scale service evaluation will allow other centres to appreciate the importance of a robust system of getting patients into the BCG clinic.
Or read this article in our
Tablet/iPad edition
- Attendance rates to outpatient BCG clinics across Leeds are suboptimal.
- We collected retrospective data for eligible patients to find those that failed to attend their appointment. For these patients we collected ethnographic, socioeconomic and demographic determinants of health. The parents were contacted to discuss factors influencing clinic non-attendance.
- We expect the Leeds experience will be generalisable nationally and this is a cause for concern.
Also published in Infant:
