

Nursing management of neonates undergoing screening for retinopathy of prematurity
Eye examinations can be unpleasant for newborn infants and sometimes they may cry or show signs of discomfort. Neonatal nurses can make this experience less distressing for the baby and its parents by careful preparation and evidence-based best practice. This article describes an audit of current practice and a quality improvement project that set out to standardise the nursing care given to infants undergoing retinopathy of prematurity screening, including the development of a unit protocol to promote a care bundle.
Beatrice Ramunno
Neonatal Staff Nurse
Trevor Mann Baby Unit, University Hospitals Sussex NHS Foundation Trust, Brighton
b.ramunno@nhs.net
Retinopathy of prematurity (ROP) is a disorder affecting the development of retinal blood vessels in preterm and low birthweight infants.1 Eye screening examinations are conducted routinely in neonatal units and are paramount in the early detection and treatment of ROP to prevent loss of vision and blindness.
However, several studies have found an association between the screening examinations and pain response, as well as a physiological negative response.1,2 Evidence-based research has found that the clinical application of developmental care/comfort measures combined with pain-relieving interventions, can be optimal in the reduction of stress and pain experienced by an infant during the screening examination for ROP.1 In this context, the role of the neonatal nurse is paramount in advocating for the infant.
Methodology
This study is a pre- and post-interventional clinical audit carried out in the neonatal intensive care unit (NICU) at the Trevor Mann Baby Unit (TMBU) in Brighton. It focuses on the nursing interventions of neonatal nurses looking after infants undergoing screening for ROP under the national guidance of the Royal College of Paediatrics and Child Health.3
All data were collected through direct observation of caregivers; the privacy of the participants was protected in accordance with the Data Protection Act (2018).4
A primary set of data involving nine cases was collected prior to the implementation of a checklist to guide nursing staff. A comparative set of data for 10 cases was audited following the intervention. The checklist (FIGURE 1) was designed to guide and educate nursing staff in the best practice management of the neonate undergoing screening for ROP. The checklist was made available in all the nurseries of the neonatal unit following the pre-intervention audit. Each nursery has a folder in which useful information, including protocols and procedures, are stored. A checklist was put into each folder. There is also a ‘communication book’ to share messages for the whole team; a note and copy of the checklist was left here. Lastly, information about the audit and the checklist was posted on an informal group chat, which was an easy way to access everyone.
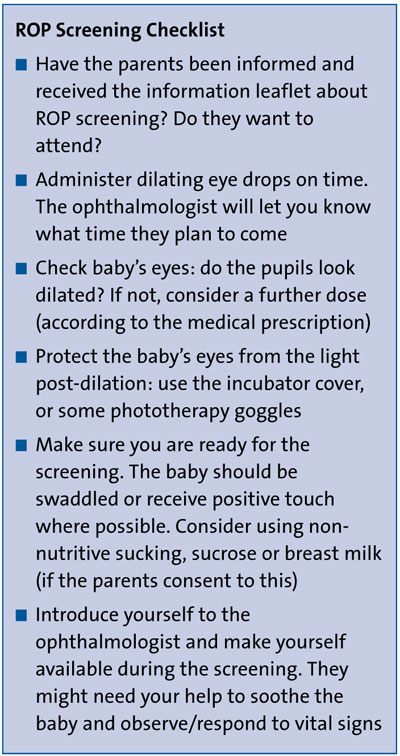
FIGURE 1 The checklist for nursing management of the neonate undergoing ROP screening.
The selected audit criteria included the following:
1. Involvement of parents
The infant’s parents should be informed of the day and time of the screening and invited to be involved during the screening examination. An information leaflet about screening for ROP should be given to them.
2. Timely administration of eye drops
Mydriatic eye drops should be administered to the patient by the neonatal nurse in order to obtain adequate pharmacological dilation of the pupils in preparation for the screening. The local unit protocol recommends administering phenylephrine 2.5% and tropicamide 0.5% (one drop of each drug in each eye, in three sets 30 minutes apart) prior to the examination.
3. Nurse examination of infant’s eyes
The neonatal nurse should assess the pupils of the infant after dilation and establish whether a further set of mydriatic eye drops should be administered prior to the examination (in accordance with the prescription from the medical team).
4. Nurse presence during the procedure
Was a neonatal nurse present during the examination to support the ophthalmologist?
5. Parent presence during the procedure
Was a parent present while the ophthalmologist performed the examination?
6. Application of positive touch/swaddling
The nurse or parent should employ hands-on containment or infant swaddling during the examination. If appropriate, the infant should be settled in a comfortable support (nest) and set in a flexed position with symmetric head position.5-7
7. Use of EBM/sucrose/non-nutritive sucking
Multisensory interventions such as the use of expressed breast milk (EBM), sweet tasting oral sucrose and non-nutritive sucking are recommended as pain relief/comfort measures.5-7
8. Use of eye protection
Protective phototherapy goggles and/or incubator covers are recommended to reduce light stimulation and manage stress related to photosensitivity during pharmacological dilation of the pupils.8,9
The minimum standard of compliance for criteria 1, 2, 3, 4, 6 and 8 was set at 95%. For criteria 5 and 7, a minimum of 80% compliance was chosen. The lower value reflected that criteria 5 and 7 were not directly related to the actions of the nurse (ie parents being able to visit, or baby being allowed to have EMB/sucrose/non-nutritive sucking).
Results
TABLE 1 shows the data collected during the first section of the clinical audit; nine cases were observed. TABLE 2 shows the data collected following implementation of the checklist. A total of 10 cases were observed.
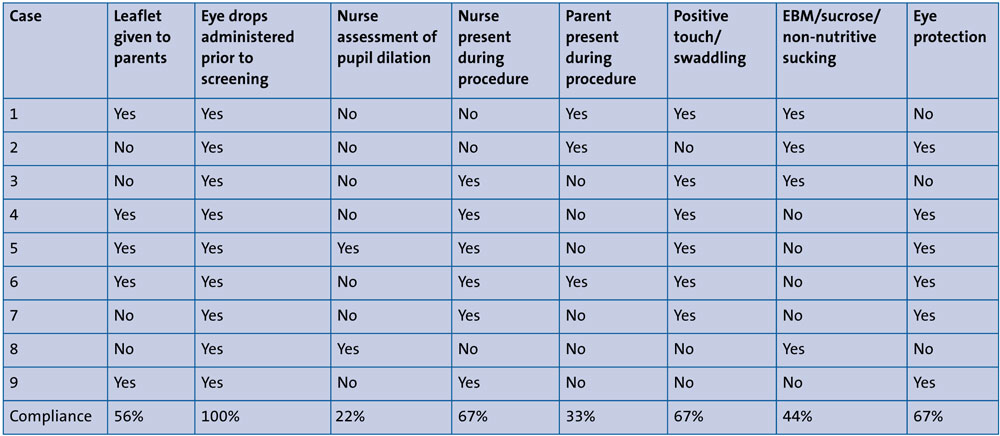
TABLE 1 Nursing interventions during ROP screening: pre-intervention.
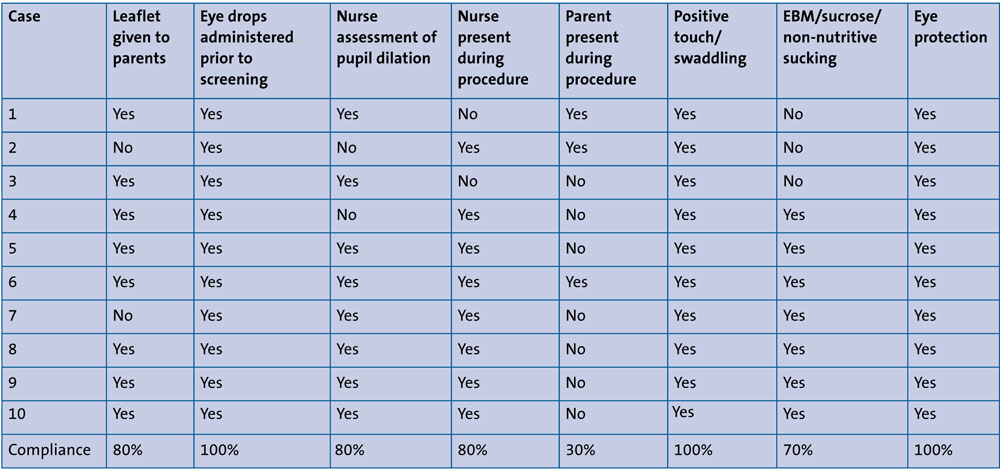
TABLE 2 Nursing interventions during ROP screening: post-intervention.
Discussion
Most evaluated criteria showed an improvement following the implementation of the checklist; the minimum compliance was achieved in standards 2, 6 and 8 following the implementation.
Involving parents
Parents were initially informed of the ROP screening in 56% of cases rising to 80% post-intervention. While some parents appreciated being given an information leaflet, others preferred (or would have preferred) having a direct conversation with the ophthalmologist, which was not always possible due to visiting times of parents and the scheduled time of the screening.
Eye drops administration
Mydriatic eye drops were administered within the appropriate time frame prior to ROP screening in both sections of the audit – in 100% of cases prior to and post-implementation. The neonatal nurse assessment of an infant’s pupil dilation improved from 22% of cases to 80% of cases. Furthermore, following the introduction of the checklist, the medical prescription for mydriatic eye drops was changed from three times daily to ‘as needed’, allowing the neonatal nurse to administer eye drops at an appropriate time to guarantee mydriasis during screening. This action improved the out-come in terms of efficiency and efficacy; reducing delays in the administration due to a missing prescription and ensuring a successful examination thanks to optimal pupil dilation.
More recently, some cot signs have been created, which say: ‘I have ROP screening today; the doctors are coming at (…)’. These can be left at the cot side to remind the nurses to give the eye drops on time.
Support from the neonatal nurse during ROP screening
The presence of a nurse assisting the ophthalmologist carrying out the examination improved from 67% of cases to 80% of cases. The support of a neonatal nurse during screening is vital – they are responsible for monitoring the infant’s vital signs and response during the examination as well as providing comfort to the infant when a parent is not available.
Presence of a parent during ROP screening
The presence of a parent during the examination for ROP corresponded to 33% of cases in the primary data audit and 30% in the secondary set. This was in part due to the unit visiting policy, which was affected by the COVID-19 restrictions.
Some parents said they did not wish to be present during the screening because they found it distressing.
Multisensory interventions during ROP screening
Comfort techniques such as positive touch and infant swaddling were employed in 67% of cases prior to implementation of the checklist, increasing to 100% of cases post-implementation. Non-nutritive sucking was employed in 44% of cases in the primary data set, rising to 70% post-implementation. Sucrose solution was the sweet substance most often adopted for sensory saturation, being easily available in the neonatal unit. Breast milk requires a double-checking procedure and warming up and hence was employed less frequently.
Protective measures against light
Great improvement was seen here. Protective measures were adopted in 67% of cases prior to introduction of the checklist, improving to 100% of cases post-implementation. Prior to the checklist, junior staff members reported not being aware of the stress caused by photosensitivity in infants who had received mydriatic eye drops. At this time, the protective measures comprised incubator covers, which were employed independently from the ROP screening. Following introduction of the checklist, incubator covers where used for infants in incubators as well as open cots and there was greater understanding of the effects of mydriasis among staff members. Incubator covers and muslin cloths were the most commonly used measures as they were readily available in the neonatal unit and better tolerated by the infants, compared with phototherapy goggles.
Conclusion and recommendations
The pre-intervention section of the clinical audit highlighted some sub-optimal aspects of care regarding nursing management of neonates undergoing screening for ROP. These were related to lack of experience of junior staff members, or time issues and workload.
The post-intervention section of the clinical audit showed improvement in care, which was optimal or nearly optimal in most aspects evaluated. This demonstrates the importance of staff training in delivering high standards of care to patients. In general, there is a better awareness regarding the management of babies undergoing ROP screening. The hope is that for the coming year, ROP nursing management will be included in developmental care teaching sessions on the unit. Ideally, further audits will be carried out at regular intervals to ensure that best practice is maintained.
Or read this article in our
Tablet/iPad edition
- Junior nursing staff should be trained in ‘best practice’ to improve nursing care and minimise complications during neonatal screening for ROP.
- A standardised unit protocol (checklist) has been developed for nursing staff to refer to as a guide for newborns undergoing ROP screening.
- Compliance with the checklist led to an improvement in care.
Also published in Infant:
