

The use of massage to reduce pain and stress associated with retinopathy of prematurity screening
Massage was implemented into a level three neonatal unit in Scotland. The Neonatal Pain, Agitation and Sedation Scale (NPASS) was used to measure the preterm infants’ pain prior to, during and post-retinopathy of prematurity (ROP) screening. Staff and parents provided feedback/testimonials on their experiences with the massage therapy.
Michelle Brooks
Advanced Specialist Nurse – Neonatal Practice Education
michelle.brooks@lanarkshire.scot.nhs.uk
Gill Currie
Advanced Practitioner Neonatal Occupational Therapist
Neonatal Unit, University Hospital Wishaw, Scotland
Brooks M., Currie G.The use of massage to reduce pain and stress associated with retinopathy of prematurity screening. Infant 2023;19(5):174-78.Background
Historically, touch has been utilised for its healing properties in various cultures.1 Touch is the first sensory system to develop in the fetus and it is experienced in utero while the fetus is surrounded by amniotic fluid. As the fetus moves, it pushes against the mother’s uterus and abdominal wall, which provides the early sensation of tactile stimulation.2 Preterm infants have limited exposure to this type of internal positive touch stimulation as it replaced by external negative procedural touch and sensory stimuli, including light, noise, pain and handling.3 Any pain and stress that a preterm infant is exposed to occurs during a period of rapid brain development – at a time when it is developmentally unexpected.4 It is believed that an average preterm infant will experience a minimum of two invasive procedures per day and this number can increase and/or vary greatly within the neonatal intensive care unit (NICU).5 Consistent exposure to various procedural touches and painful interventions may negatively impact the long-term neurodevelopment of preterm infants.6 The frequency and severity of exposure to pain and stress has been recognised as having an influence on cortical connectivity and altered brain function. Neurobehaviour from as early as 30 weeks post-menstrual age can be a potential indicator for adverse developmental outcomes. Effective pain prevention and management can contribute to neuroprotection in the preterm infant.4 Preterm infants face enforced separation from their parents, which also potentially has a negative effect on brain development and long-term neurodevelopmental outcomes.4 Physical and emotional closeness are essential to the health and wellbeing of parents with preterm infants.7 In addition, parental participation in care can help with attachment, increased confidence, and interaction, thus contributing to the concept of family-integrated care.8 The stressful environment of the NICU – specifically for preterm infants who encounter frequent essential, yet invasive and painful, procedures – has previously been acknowledged. One such procedure is retinopathy of prematurity (ROP) screening, which is a necessary diagnostic tool to identify those at risk. If ROP is left untreated, loss of vision and blindness can result. During the screening examination, ophthalmologists use eye drops for dilation and instruments that cause pain and discomfort (FIGURE 1), which can lead to an increase in heart rate and a decrease in blood oxygen saturation in a preterm infant.9 FIGURE 1 During the ROP screening examination, ophthalmologists use eye drops for dilation and instruments that can cause pain and discomfort. 
A study explored the use of massage as a developmentally supportive intervention and defined massage as ‘systematic touch by human hands which stimulates the tactile sense of the infant’.10 Moreover, Field and Diego (2006) describe massage therapy as ‘one of the most effective forms of touch, used primarily to treat pain’.11
Lieu et al (2022) suggest that massage is a more effective pain relief for procedures than positive therapeutic touch.12 There are additional benefits of massage for preterm infants with several studies stating that providing massage with coconut oil and moderate pressure can also contribute to improved weight gain.3,13-16 Pupala et al (2019) carried out a systematic review and concluded that the topical application of coconut oil on the skin of preterm infants reduced infection rates, while improving skin condition.17
Various non-pharmacological methods to relieve pain are utilised in the NICU, which include skin-to-skin contact, breastfeeding or use of expressed breast milk, oral sucrose, facilitated tucking, non-nutritive sucking and massage.18,19 A study by Jain, Kumar and McMillan (2006) proposed the use of massage led to lower pain scores for venepuncture.20 Moselhi et al (2019) concluded that massage provided lower pain scores during venepuncture and suggested it should be used routinely for preterm infants undergoing painful procedures.21 Venepuncture, however, is performed at variable and unpredictable times; therefore the use of massage for a more predictable procedure known to cause pain and or discomfort was identified for our project.
The starting point: the massage project
The neonatal occupational therapist (OT) at University Hospital Wishaw was already certified in massage and had been using massage with infants and families within the NICU for a number of years. Parental feedback was extremely positive, with many parents saying they felt a stronger bond and had more confidence in handling their babies. Closeness, both physically and emotionally, between parent and infant is important in the emerging parent role as providing care for their baby helps acknowledge them as a parent as well as contributing to infant mental health.8 Therefore, parental participation wherever possible, is actively encouraged in the NICU.
The OT and neonatal practice educator nurse, in collaboration with the neonatologists, identified the use of massage for the relief of pain and stress related to ROP screening. The rationale for identifying this particular procedure was that it was well documented to be painful and it occurred weekly at a predictable time when the OT was available to perform massage and/or support parents to provide massage. The ophthalmology team were consulted and were very supportive of the project.
In order to facilitate massage, the use of an oil had to be considered. Topical oils have been used for massage as traditional practice in India and South Asia for centuries.3,15,22 Following a review of the evidence with our lead consultant in agreement, coconut oil was chosen due to its well-documented benefits.
Our NICU utilises the Neonatal Pain, Agitation and Sedation Scale (NPASS), which is a reliable assessment tool for neonatal pain. Scores are calculated and recorded using the electronic patient record (EPR). The NPASS scale ranges from 0 (no pain response) to 10 (highest pain response). The assessment criteria of NPASS are:
- crying and irritability (from no crying with painful stimuli through to continuous inconsolable crying)
- behaviour state (from no arousal through to arching/kicking)
- facial expression (from no expression through to continual pain expression)
- extremities and tone (from no grasp reflex/flaccid tone through to clenched toes/fists or finger splay and tense body)
- vital signs (heart rate, respiratory rate, blood pressure, oxygen saturation).
Prior to officially launching the project, the OT and practice educator selected a pilot preterm infant to gauge the response to massage prior to ROP screening. The eligibility criteria for massage were used (see Methods section) and consent from the parents was obtained. The parents were also taught how to perform the massage themselves. The schedule for this pilot incorporated 10 minutes of massage, 15-30 minutes prior to ROP screening with NPASS scores obtained prior to the massage, prior to the procedure, during the procedure and 10 minutes after the procedure. The scores revealed a moderate pain response during the procedure; however, 10 minutes post-procedure, there was no pain score (back to baseline).
Parental and staff feedback was collected throughout this pilot trial. Prior to the trial, the parents were often unable to handle/cuddle their baby following ROP screening due to clinical incidents and/or the baby often struggling with feeds. In this aspect, the parents reported a marked difference and major improvement each week from the start of the massage trial – they increasingly reported being able to hold and comfort their baby. Staff also reported that the baby was tolerating handling better following massage and a more stable heart rate, respiratory rate, oxygen saturations and improved feeding patterns. The lower NPASS scores and positive feedback from the parents provided reassurance and we were confident to increase the sample size and offer massage to all infants receiving ROP screening who met the eligibility criteria.
Aim and hypothesis
The aim of the project was to determine whether massage can reduce the pain and stress associated with ROP screening for preterm infants. The working hypothesis was that infants who received massage prior to ROP screening would have reduced NPASS scores during the ROP screening process and within 10 minutes following the screening (FIGURE 2).
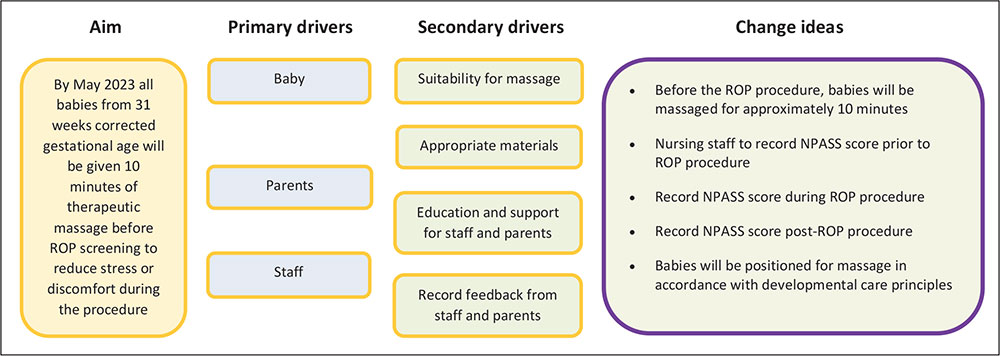
FIGURE 2 The driver diagram.
Methods
The project documented 40 NPASS scores for infants not massaged and 60 NPASS scores for infants massaged before, during and after ROP screening to compare the potential effect of massage on NPASS scores.
It was agreed that massage prior to ROP screening would be routine in the NICU and therefore an opt-out policy would be adopted should parents not want their infant to receive massage. All parents were encouraged to be present for the massage or provide it themselves with the support of the OT. Parental presence is supported during ROP screening but most parents choose not to hold their baby nor watch the procedure as it is upsetting.
Scoring infants before, during and after ROP screening commenced in November 2022 to gather baseline data. Thereafter, any baby not massaged prior to ROP screening was either due to not meeting the eligibility criteria or the OT or parents being unavailable to perform the massage.
The order of the ROP screening was dictated by the order of massages, which required agreement from the ophthal-mologist. The timing of massages was dictated by feeding times. The OT performed/assisted parents with the massages while the practice educator coordinated data collection and scoring. Nursing staff assisted with NPASS scoring and dressing/undressing babies, where required.
The standard practice for ROP screening with local anaesthetic drops, expressed breast milk/oral sucrose and containment holding was adhered to throughout the project.
Eligibility criteria
The OT has massage certification and this guided the eligibility criteria. Infants were eligible if they were over 31 weeks corrected gestational age and weighed more than 1,200g.
In our neonatal unit, infants born at <31 weeks’ gestation or under 1,500g are examined to screen for the presence of ROP. The ophthalmologist continues ROP screening for many weeks post-eligibility criteria and post-discharge as an outpatient, if required. Therefore, the criteria for massage from 31 weeks’ corrected gestation aligned with the ROP screening criteria.
Protocol
Massage therapy was performed either an hour before or after feeding. The OT and practice educator would check with the nursing staff for any clinical signs that would be a contraindication to massage, such as recurring incidents, infection and instability with handling.
For the purpose of the project, it was agreed that infants would be massaged for 10 minutes, 15-30 minutes prior to ROP screening. However, this did not prove practical due to slight variation in the ophthalmologist arrival time on the NICU. Therefore, on average, massages were generally given one hour prior to ROP screening.
The OT provided 10 minutes of massage for the infants that were receiving ROP screening. The method was adapted to facilitate the least amount of position changes. Infants were placed in a side-lying position with massage strokes applied to their back, top arm and top leg (FIGURE 3). Throughout the massage, the OT observed the infant for any signs of stress while being aware of the monitor displaying any changes in heart rate, respiratory rate and oxygen saturation. Prior to any massage, the baseline clinical status of the infant was noted.

FIGURE 3 Infant massage prior to ROP screening. (A-C) Massage given by OT. (D) Massage given by OT and parents.
NPASS scores were recorded prior to, during and 10 minutes following ROP screening. The standard practice for ROP screening with local anaesthetic drops, expressed breast milk/sucrose and containment holding was adhered to throughout the project. NPASS scores were collected over a six-month period.
Outcome measures
The definitive outcome measure was pain scores. The NPASS scale was used to measure the infants’ pain and stress levels. These scores were recorded on the EPR before, during and 10 minutes after the ROP screening. The staff and parents completed feedback forms on their visual observations and clinical observations/ occurrence of incidents during and in the 10 minutes following the procedure, were also included.
Results
The NPASS scores were lower during and post-ROP screening for the babies massaged (median 4 and 0) compared with those not massaged (median 7 and 1). This is consistent with the pilot trial infant (FIGURE 4). We recorded the NPASS scores of infants prior to massage and prior to ROP screening, which provided a useful baseline. We have not included any data on this as the effect was demonstrated with NPASS scores recorded during and post-screening.
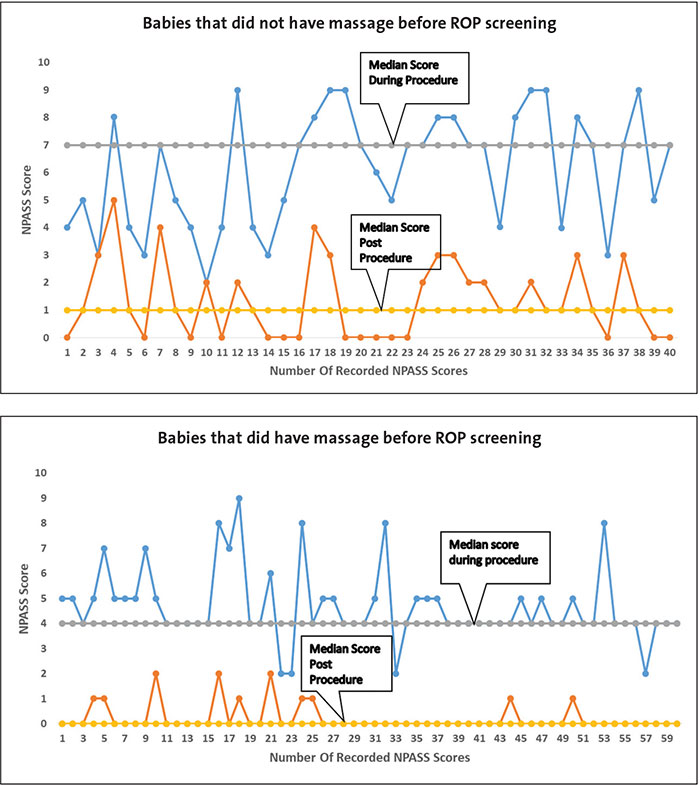
FIGURE 4 The run charts of NPASS scores during and post-ROP screening. Top: For those infants who did not receive massage (n=40). Bottom: For those infants who did receive massage (n=60). The blue lines represent the NPASS scores during the screening procedure and the orange lines are the NPASS scores after screening. The solid grey/yellow horizontal lines indicate the median.
Challenges and successes
The initial challenge was the uncertainty of using massage specifically with ROP screening. The West of Scotland Guideline 2022 advises provision of non-pharmacological pain relief for babies prior to ROP screening using expressed breast milk and oral sucrose.23 Other methods of pain relief are pharmacological, such as local analgesic eye drops administered prior to the procedure.
Another challenge was setting the parameters for:
- duration of massage
- method of providing massage
- time lapse between massage and ROP screening.
All of the above were experimental but appeared to be appropriate.
The main success of the project was identification of a correlation between preterm infants receiving massage and lower NPASS scores during and post-ROP screening. In addition, the data revealed reduced NPASS scores at over one-hour post-massage. This suggests that the comfort provided by massage has a longer lasting effect than initially anticipated.
The authors are not aware of any studies relating to the length of effect that massage can provide.
The infants all responded positively to massage with fewer incidents; increased clinical stability and tolerance of handling; and improved feeding patterns and parent satisfaction compared to before the massage project. Because of these positive results, we would like to review the use of massage as non-pharmacological pain relief. Our future plan is to facilitate and encourage parents to use massage in the neonatal unit; we can now reassure them that massage provides comfort and pain reduction, which we hope will encourage them to use massage during their visits to their baby. Three of our nurses are going to complete the massage certification training in the next couple of months; this will mean more staff are available to demonstrate the massage techniques to parents.
Testimonies
Parental testimonials have been exclusively positive. The parents felt their baby was relaxed and enjoyed the massage experience, as did they. They felt that the massage helped with bonding and attachment. With regards to the ROP screening procedure, the parents felt their babies were more settled and coped better with being held and fed following screening.
“The whole massage experience was so calm and relaxing and made a big difference to our baby coping with the ROP check”
Parent 1.
“One of the most positive experiences we had with our baby. This experience was invaluable and helped so much with our confidence to touch our baby”
Parent 2.
“Massage helped with the pain after our baby’s ROP screening. Both of us enjoyed being able to provide comfort for her with massage”
Mum and Dad.
“I am aware babies can become distressed both during and after ROP. The baby was a lot less visibly stressed than babies usually behave during ROP. His posture was more relaxed in the crib and he was nice and sleepy after the procedure was complete”
Nursing staff member 1.
“I think our babies are really benefiting from the project”
Nursing staff member 2.
“The babies are a lot more settled during the procedure and have less incidents”
Nursing staff member 3.
Conclusion
As hypothesised, massage can contribute to a reduction in the pain and stress associated with ROP screening. There is no reason why these results could not be transferable to various other painful procedures. Additionally, the comforting effect of massage lasted longer than expected and, therefore, a daily massage could potentially counteract painful procedures throughout the day in a NICU, although further studies to explore this theory are required. Integrating massage into existing pain management policies and procedures, and empowering parents to lead is our vision for the future.
A goal of family-integrated care is to involve parents in providing care for their infants. Procedural touch is unavoidable for our fragile preterm population but positive touch is encouraged and beneficial for preterm infants. The outcome of this project has been extremely positive in terms of reduced NPASS scores and in the positive reactions of content and settled infants. The parents were encouraged by their baby’s response and this inevitably provides comfort to them also.
As clinicians, we must acknowledge the importance of the parent-infant relationship and how we can support the physical and emotional needs of the parent and preterm infant. Henceforth, massage can be seen as method of empowering parents in providing comfort for their baby as part of a developmentally supportive family-integrated care approach.
Contributions
The authors shared a vision of using massage to reduce pain and stress for infants receiving ROP screening in the neonatal unit at University Hospital Wishaw. They worked collaboratively with the multidisciplinary team to plan, implement and review the project, displaying the data in an easily adaptable form to facilitate shared learning.
Acknowledgement
The authors are grateful for the help of Lorraine McGrory, Augusta Anenih, Lorna Lennox, Andrew Brown, the ophthalmology nurses and the neonatal nursing team.
Or read this article in our
Tablet/iPad edition
- Massage can reduce procedural pain for preterm infants.
- Massage given to infants and demonstrated to parents in the neonatal unit can provide comfort and reduce pain and stress associated with ROP screening.
- No babies experienced any untoward side effects.
Also published in Infant:
