

Widening access to SHINE (Simulation to Help in Neonatal Emergencies) to include QIS students
Simulation is known to improve clinical skills and team communication. This article describes how an existing full-day simulation and workshop-based course, originally designed for post-graduate doctors-in-training, was adapted to provide educational opportunities and experiential learning for nurses undertaking the qualified in specialty (QIS) course. This also gave the doctors-in-training a more authentic multidisciplinary approach to clinical scenarios.
Jessica GroucuttSpecialty Trainee in Paediatrics, West Midlands Deanery
j.groucutt@nhs.net
Jennifer Bradford
Band 7 Nurse Educator
Matthew Nash
Clinical Director, Neonatal Consultant and Programme Director for Postgraduate Neonatal Simulation, West Midlands Deanery
Neonatal Department, Birmingham Women’s and Children’s NHS FT
Groucutt J., Bradford J., Nash M. Widening access to SHINE (Simulation to Help in Neonatal Emergencies) to include QIS students. Infant 2024;20(1):25-28.
Background
Simulation is well-established in health care as an excellent modality for learning; it allows us to refine clinical practice, reflect and reframe ideas as well as explore communication, human factors and multidisciplinary team working in a safe, patient-risk-free environment.1 Simulation facilitates interprofessional learning, which is in line with the NHS model of integrated, multidisciplinary care working. This has been shown to increase patient satisfaction and the quality of care received.2 The UK simulation strategy currently aims to ensure equity of access to simulation facilities, equipment and learning opportunities nationally so that all learners and staff can benefit.1
The recent independent maternity review, the Ockenden report,3 highlighted seven immediate and essential actions for all maternity trusts, including: ‘staff who work together must train together’.3 This can be interpreted as further in situ, multidisciplinary and clinical simulation training. The neonatal intensive care workforce is varied and large in number leading to endless permutations of teams for clinical scenarios. This coupled with new starters and rotating postgraduate doctors-in-training means that we need to also equip nurses with suitable language, escalation and clinical skills when working within unfamiliar teams.
Nursing students have had access to simulation tools, such as task trainers and anatomical models, since the 1800s, however, there are new innovations in sophisticated technology and high-fidelity simulation. In our deanery, the medical teams seem to have greater access to simulation-based education and courses, with funding being more readily obtained. Nursing education has traditionally been primarily placement-based with student experience dictated by current patient variety and specific shift experiences. The value of simulation in nursing education has been recognised as a collaborative, interactive, experiential learning experience. The Nursing and Midwifery Council, realising that direct patient experience may have been limited by the COVID-19 pandemic, introduced a set of emergency and recovery standards for nursing and midwifery education, which allowed students to undertake up to 300 hours of simulated learning out of the overall 2,300 practice learning hours.4
The QIS course
Nurse education is not limited to undergraduates but continues throughout career progression. In our unit, nurses typically start their career looking after special care babies and then build up their knowledge to care for high-dependency and then intensive care babies. To care for intensive care babies, the nurses interview for, and then complete, the qualified in specialty (QIS) course (TABLE 1). The course runs for six months, building the skills of caring for sick and preterm babies.
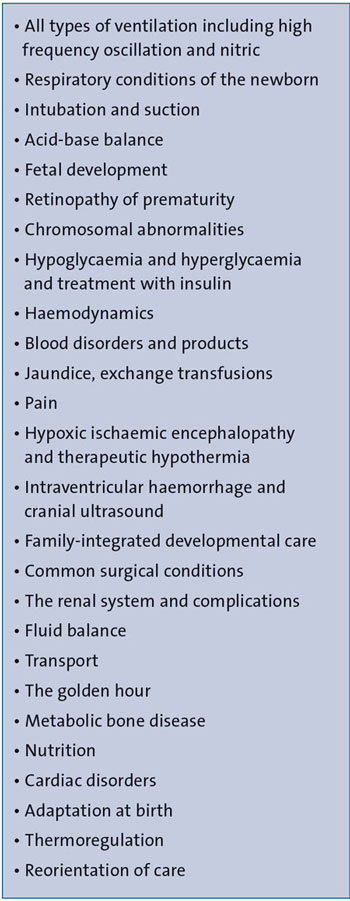
TABLE 1 Typical topics covered in the QIS course.
In our unit, the course is assessed through a verbal presentation of a baby that each nurse has cared for, covering evidence of all elements of that baby’s care; a written case study on a baby or a review of articles relevant to intensive care. At work, each nurse is allocated to an existing QIS-qualified nurse and has one supernumerary shift per month to develop their skills. The education team members also work shifts with them to support their development. They are allocated a bleep day which follows the tier one medic, allowing familiarisation with the delivery suite, initial resuscitation process and support that may be required from the team. The bleep day, as with neonatal care, is unpredictable and thus varied experiences are had by the nurses, meaning some are more prepared than others when taking the nursing delivery suite bleep for the first time. They also must be a neonatal life support (NLS) provider, prior to carrying the delivery suite bleep.
Health Education England published a review of education and training for the QIS Course in 2021.5 Key findings included:
- a lack of standardisation of QIS skills and knowledge
no professional regulation or monitoring of the content, quality or consistency of the qualification.
Concerns were raised over funding and the time allowed for QIS training. Several recommendations were made as a result of this investigation, including more practical experience structured to consolidate learning and ensure significant experience.
As well as looking after babies from 22 weeks’ gestation, our unit is a specialist cardiac, surgical and cooling centre. We, therefore, want to equip our nurses with the education and confidence to deal with these cases.
The SHINE course: Simulation to Help in Neonatal Emergencies
To standardise the ‘bleep’ and scenario experience and to give nurses more practical experience, we invited those nurses just about to complete the QIS course to take part in our SHINE (Simulation to Help in Neonatal Emergencies) Course.
SHINE is a full-day neonatal emergency simulation course that was established in 2018 for West Midlands paediatric postgraduate doctors-in-training. It consists of four scenarios and two workshops (TABLE 2) for eight candidates. It runs four times per year. The candidates are split into two groups allowing each to ‘lead’ a scenario with, traditionally, faculty placed as nursing ‘plants’. The simulation structure would be brief – for five minutes, the scenario itself lasting 10-15 minutes – with a structured debrief, utilising the Diamond debriefing model6 and advocacy of enquiry.
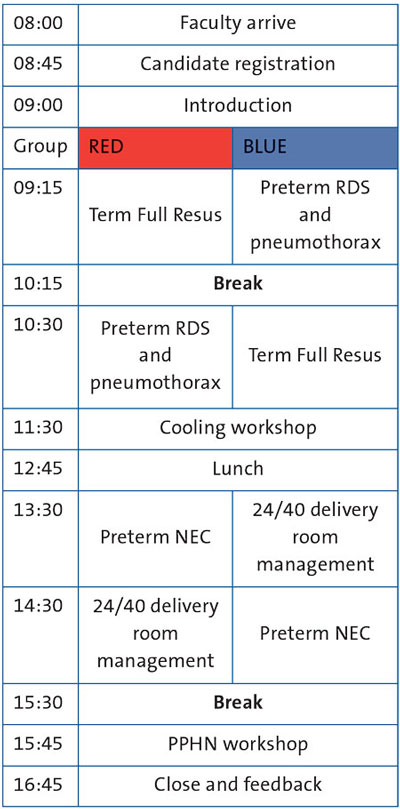
TABLE 2 SHINE course structure. Key: RDS=respiratory distress syndrome; NEC=necrotising enterocolitis; PPHN=persistent pulmonary hypertension of the newborn.
The simulations run on our neonatal unit involve both nursing staff and medical candidates, allowing for true multidisciplinary working and these experiences are highly appraised by candidates. The QIS nurses took the nursing role (traditionally the faculty ‘plants’) in the SHINE scenarios, either caring for the simulated mannikin in the neonatal unit or carrying the labour ward delivery nursing bleep, aiming to make the scenarios more authentic.
The aim of the study was to:
- make the SHINE course more authentic to real life with a multidisciplinary approach to the scenarios
see if inviting neonatal unit nurses to the course affected the postgraduate doctors-in-training feedback
assess if the nurses felt it was beneficial for their training.
Evaluation
We evaluated the relevance, confidence levels and learning environment for both the doctors and nurses attending the course in written anonymous feedback. Questions were either a Likert scale, discrete answers or free text (TABLE 3).
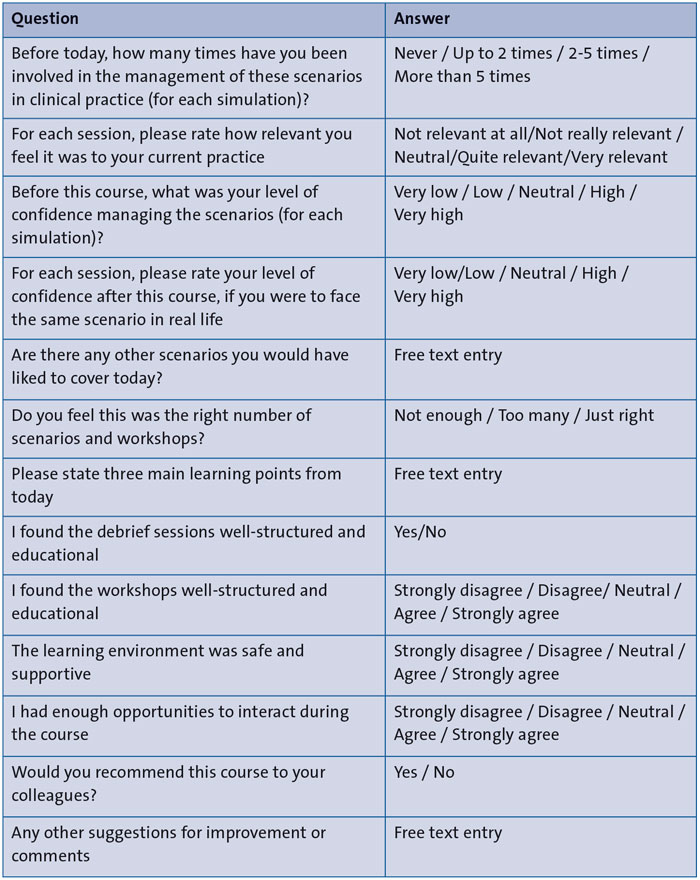
TABLE 3 The feedback questionnaire.
To ensure that inviting neonatal QIS students wasn’t detrimental to the postgraduate doctors-in-training learning experience, we compared previous feedback from SHINE courses using nursing ‘plants’ to this course format.
Results
Feedback from the nurses who attended so far (n=16) has been very positive and we have now run this format on three occasions. Previous experience of the scenarios was variable but generally low with all candidates feeling that all scenarios were quite or very relevant to their current practice. FIGURE 1 shows self-rated confidence levels for facing all scenarios in real life before and after the course.
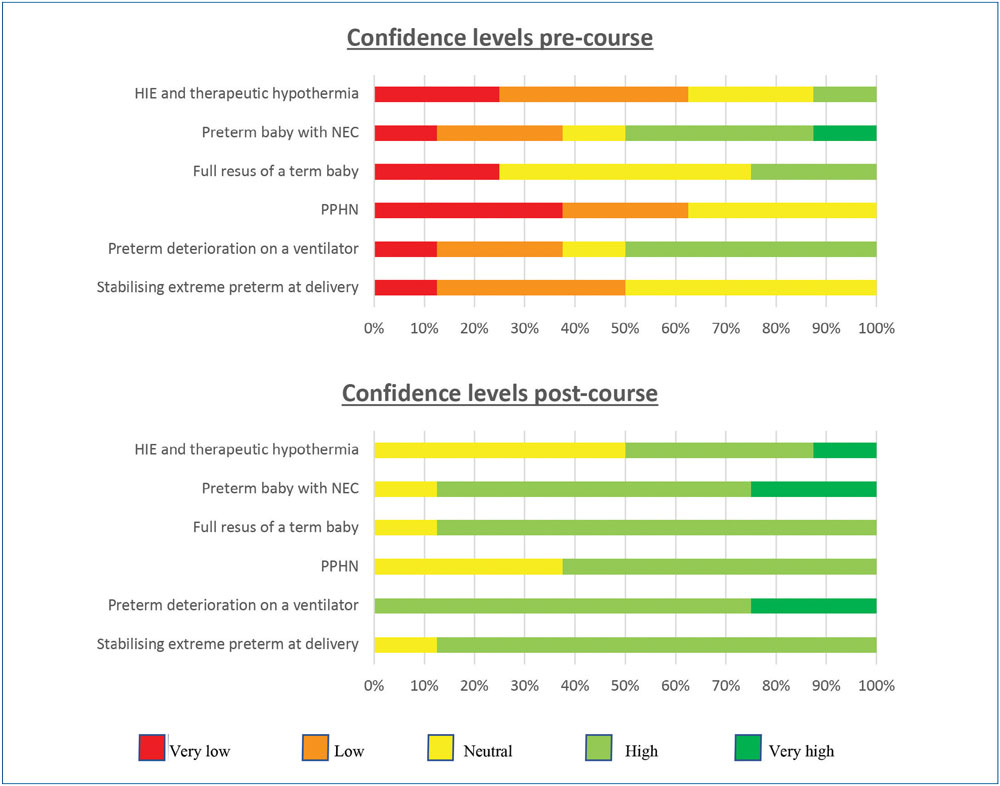
FIGURE 1 Self-rated confidence levels for facing scenarios in real life before and after the course (feedback from nurses who attended, n=16). Key: HIE=hypoxic ischaemic encephalopathy.
All candidates felt there were the correct number of scenarios and workshops. All agreed that the workshops were well structured and educational with 62.5% strongly agreeing with this statement. All agreed that the learning environment was safe and supportive with 87.5% strongly agreeing with this statement. 87.5% felt they had enough opportunity to interact on the course.
87.5% rated the debriefs as extremely useful with a further 12.5% as useful. The debriefs covered any questions or concerns about the clinical management of each scenario but nurses felt that the key learning points were actually more about team interaction. The themes listed included the importance of clear communication: using clear, concise language, closed-loop communication, escalation, questioning and prompting and practice of SBAR (situation, background, assessment and recommendation) handovers. They learnt about leadership and having a ‘helicopter’ view, the importance of good followership and calling for help at an appropriate time point. In anonymous feedback, all of the nurses that have so far attended (n=16) would recommend this course to a colleague.
Informal feedback has also been given to the nursing education team. Those attending felt that they found it very useful to see and deal with emergencies in a safe environment with an opportunity to debrief. It was suggested that it would be more useful after the students had completed the Neonatal Life Support training, but this would depend on the timings of the courses. The nurses also liked that the focus was on what goes well and the reasoning through things if they haven’t gone well, rather than what went wrong.
The nursing education team felt there were challenges with embedding the course due to not getting confirmed course dates early enough, as study leave must be rostered several months in advance and demand outstripping course places (staff who have completed QIS would also like to attend).
The postgraduate doctors-in-training feedback (n=32) was very positive and comparable to previous courses that have run. All would recommend the course to their colleagues and felt they had enough opportunity to interact.
Constructive developmental points were also suggested for the course and so we now start each neonatal unit-based scenario with the nursing team, as this is true to real life. We have also adopted the same course structure but with different scenarios and workshops in our Advanced SHINE course, including a communication workshop that allows nurses to talk about active comfort care in a dying baby. Advanced SHINE also covers some of the scenarios that the nurses and doctors suggested for simulation in their feedback, such as management of cardiac arrhythmias and congenital surgical conditions.
Conclusion
SHINE is a well-established sought-after course shown to be effective and highly valued by paediatric postgraduate doctors-in-training. Given the positive feedback, we will be inviting four nurses to each SHINE course and integrating it into QIS training.
We suggest that simulation should always strive to be multidisciplinary. Existing courses and training days can be adapted to add nursing staff benefiting both the medical team and the nursing team. This is possible without incurring additional costs (other than paying those staff members for a day of study leave) and means that QIS nurses get more standardised practical experience in a safe learning environment.
Acknowledgements
The authors are grateful to the following for their roles in the neonatal simulation programme:
For scripting the original scenarios:
- Isobel Fullwood, Consultant Paediatrician, University Hospitals Birmingham NHS Trust
Ashley Holt, Consultant Paediatrician, The Royal Wolverhampton NHS Trust
Catherine Powell, Advanced Neonatal Nurse Practitioner (ANNP), Birmingham Women’s and Children’s NHS Foundation Trust (BWC NHS FT)
Our regular rotating faculty on the SHINE course:
- Amrit Dhillon, Consultant Neonatologist, BWC NHS FT
Gillian Preston, Consultant Neonatologist, BWC NHS FT
Catherine Powell, ANNP, BWC NHS FT
Helen Cornes, ANNP, BWC NHS FT.
Or read this article in our
Tablet/iPad edition
- Access and funding for simulation can be difficult, however, the protected environment and the sense of security enhance nursing students’ learning.
- There is a lack of standardisation for nurses undertaking the neonatal QIS course.
- We propose inviting nurses to existing simulation courses to standardise experiences and improve multi-disciplinary team working.
Also published in Infant:
