

Perinatal emergency multidisciplinary simulation: identifying latent errors and improving communication between teams
Perinatal medicine requires a multidisciplinary approach with teams working in synchrony to achieve optimal outcomes. In the wake of the Ockenden report,1 a multidisciplinary perinatal simulation programme was designed and introduced at Chelsea and Westminster Hospital, aiming to improve teamworking, interdisciplinary communication and ultimately, patient outcomes. The design and implementation of the programme followed by preliminary findings are presented in this article. These include the key learning outcomes, latent errors and the influence on teamworking and current practice.
Catherine Jane DouchPaediatric Registrar and Teaching Fellow c.douch@nhs.net
Corresponding author - full author details in TABLE 1.
Work attributed to: Neonatal Intensive Care Unit, Chelsea and Westminster Hospital NHS Foundation Trust
Douch C.J., Sein E., Chow L.Y., Bayer A.S., Quiambao A.M., Patel D.S. Perinatal emergency multidisciplinary simulation: identifying latent errors and improving communication between teams Infant 2024;20(1):20-24.
TABLE 1 Author details.
Perinatal emergencies, including any subsequent neonatal care, are invariably multidisciplinary events. Multiple specialist teams, often trained in different silos, must come together and function collectively in a coordinated and simultaneous effort to complete time-critical tasks. To standardise the urgency of perinatal emergencies, all caesarean and emergency births in the UK are categorised 1 to 4 (category 1 indicating an immediate threat to the life of the mother or baby, and category 4 indicating that the birth can be timed to suit the family or healthcare staff).2 This requires effective communication and teamworking between disciplines to ensure excellence in patient care during perinatal emergency events.3
Medical teaching has traditionally focused on individual scholar’s learning skills, but this does not reflect the team nature of practice in perinatal care, where errors often arise from a failure of human factors such as poor communication practices between team members. In medicine the team nature of mistakes was first raised in ‘to err is human’ which moved the idea of ‘medical error’ away from the mistakes of individuals and towards systemic and systems failures with a focus on human factors.4 Simulation has evolved to become a fundamental pillar of training in medical education and often includes training in human factors, particularly for teams working in emergency situations such as in maternity.
Multiple reports highlight poor communication between teams as key components to failures causing perinatal mortality.1,5 The Joint Commission’s Sentinel Event Alert,6 found communication issues were the most commonly identified cause of perinatal mortality, implicated in 72% of cases alongside institutional cultural barriers. The need for formalised teaching and training around multidisciplinary team (MDT) communication was highlighted in the Ockenden report, which stated: ‘Staff who work together must train together’.1
There are approximately 6,000 births at Chelsea and Westminster Hospital maternity unit annually. The associated neonatal unit is a tertiary and surgical centre with more than 600 annual admissions.7 Since 2013, simulation has been a major aspect of junior neonatal doctor and neonatal nurse departmental training within Chelsea and Westminster Neonatal Unit. In addition, the multidisciplinary obstetric and midwifery simulation (MOMs) course has been implemented since 2010. Thus, departments were each training in parallel silos to perfect their own practice.
In response to the Ockenden report,1 the maternity and neonatal departments at Chelsea and Westminster Hospital joined together to implement MDT real-time simulations on maternity wards. The focus was on human factors, primarily communication between obstetric, midwifery, anaesthetic and neonatal teams during perinatal emergency scenarios.
Methodology and theory
The objective was to simulate emergency scenarios to examine and learn from various human factor interactions and to train together to facilitate a greater understanding of the way in which the wider team works and thinks. Each scenario was designed to last one hour, which included a 30-minute scenario and 30-minute debrief led by faculty.
Faculty
The MDT simulation faculty consisted of:
- consultants with an interest in medical education
education fellows in obstetrics, neonatology and anaesthetics
practice development staff (midwifery and neonatal) within the trust.
Logistics
Faculty members met to determine the scenarios for use in each simulation following a simulation template and learning objectives (TABLE 2 and 3). Simulations were organised and structured according to the trust format with involvement and notification of emergency bleep operators and resuscitation teams. Rota coordinators, consultants and senior midwifery staff were notified in advance of the day to ensure the barrier of time pressure to simulation was mitigated.8 To facilitate organisation and prioritisation of clinical work, on-call teams were pre-briefed.
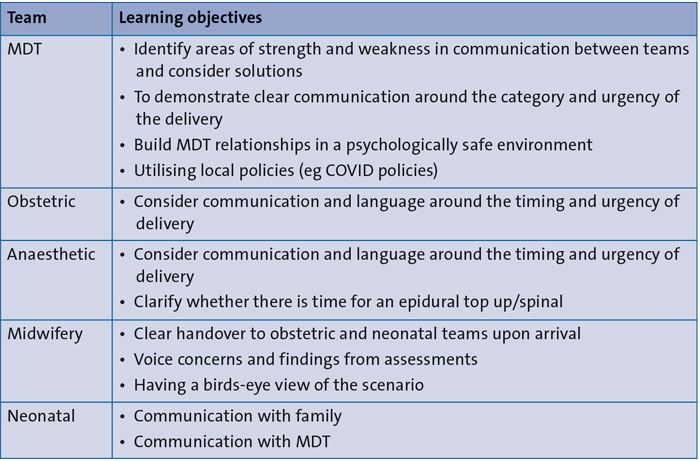
TABLE 2 General learning objectives for multidisciplinary simulation.
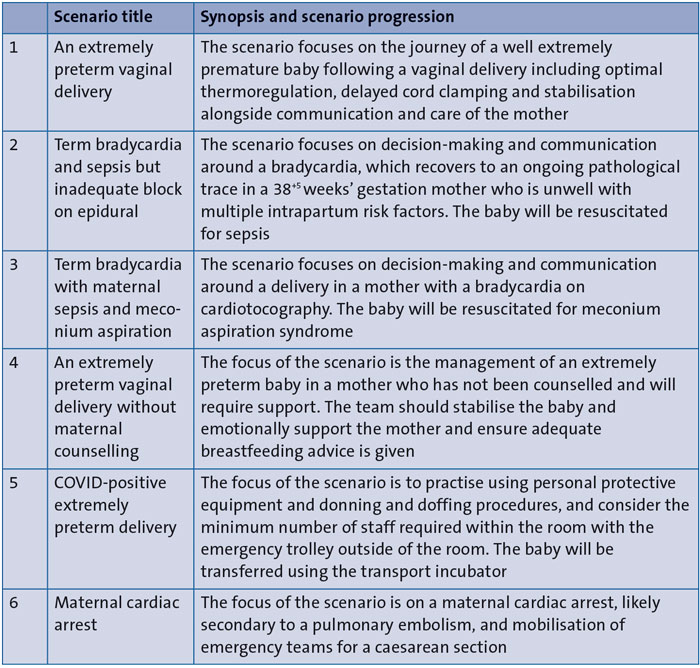
TABLE 3 MDT simulation scenarios.
Scenarios and learning objectives
All scenarios were emergency situations seen on the labour ward with a focus on interdisciplinary communication and teamworking, rather than medical rarity or complexity. Scenarios created were co-constructed with various disciplinary team inputs and designed specifically to be real time, true-to-life and of 30 minutes duration (TABLE 3).
Learning outcomes focused on the upper levels of Bloom’s taxonomy9 to encourage participants to identify problems and consider solutions. Learning outcomes were designed to integrate flexibility and problem solving, incorporating the ‘doing’ component of Miller’s pyramid,10 as experiential learning invariably involves uncertainty and unexpected interactions.11 Simulations were located on the labour ward or within obstetric theatres, allowing staff to practise and learn in the environment where they work, where knowledge is recalled, in their usual role and with the teams they work with. Adult learners are motivated by self-selected interests and engagement in tasks that will be applicable to future practice,12 therefore, the aim was to create scenarios that are commonly encountered and reflect current practice to maximise learning and stimulate a sustained change in attitudes and behaviours.13
Equipment and environment
The simulations were run in obstetric theatres with real equipment, where appropriate. Simulated patients (birthing person and birthing partner) were played by experienced faculty members. Where needed, the faculty member simulating the birth parent donned an abdominal pregnancy prosthetic. All emergency equipment was prepared in replicated trolleys that contained equivalent equipment from expired stock for purposes of costs and avoiding environmental wastage.
Participants
Scenarios involved between eight and 13 on-call MDT members and included midwives, neonatal nurses, theatre staff, doctors-in-training and consultants from neonatal, obstetric and anaesthetic teams. Consent was gained for digital recording of the scenario and debrief, for use for training development and the sharing of any learning and scholarship. On-call teams were informed of the timing of the simulation in order to redistribute urgent work during the simulation and attend the session uninterrupted. Participants were invited to the scenario via a simulation crash call, alerting the attendees to the perinatal emergency.
Debriefing
On scenario completion, a debrief was held straight after the simulation in a seminar room. The move to another room aimed to reduce stress and allow the environment to feel safe. A 30-minute debrief was led by a different nominated faculty member. MDT debriefing enables the group to unearth learning often missed in day-to-day practice. Learning together allows greater appreciation and facilitates teamworking through shared interests and problem solving.14 The intent was to provide a focus on learning rather than critique, as adult learners may disengage if judgement is perceived.13 Adequate seating and refreshments were provided to maintain comfort, as physiological needs are integral to learning and engagement.15
The intent of simulation is to provide experience while debrief is to catalyse reflective observation and abstract conceptualisation. The debriefing structure reflected that recommended in current literature.16,17
Firstly, factual recollection and description of events (‘what happened and why’) was encouraged. Participants self-select learning outcomes and concerns during this phase, this selection is part of adult learning theory and respects participants as autonomous and educated individuals. The second phase reflects ‘analysis’ during which learners reflect, dissect and consider their ‘mental models’ of practice. Patterns of behaviour, frames of thought, knowledge, understanding and their impact on decision-making and action were self and peer evaluated, under the guidance of faculty who probed where appropriate.
The final phase involves deepening knowledge and appreciating individual and group interface with human factors alongside future mitigation and optimisation with deliberative practice. This results in take-home messages for specific human factor errors. The rationale for the utilisation of this methodology is to attempt to mitigate stress and focus on learning rather than critique.13,16,17
Outcomes and analysis
Sessions were well attended including a good representation of all grades and all members of the perinatal team. Analysis of reflective notes from the debrief sessions revealed communication errors were dominant, this may reflect the common medical scenarios. Disparities between perceptions of the clinical situation and gaps in knowledge between the different disciplines were unveiled, thus promoting learning between the disciplines. The groups problem-solved and brainstormed, offering solutions and highlighting how their future practice would change. To close, each participant and faculty member shared a key learning point which closely mirrored the learning outcomes with a focus on communication and strategy.
Debriefing and outcomes were analysed within themes. From the analysis, the main themes were teamworking, communication, roles and environment (FIGURE 1).
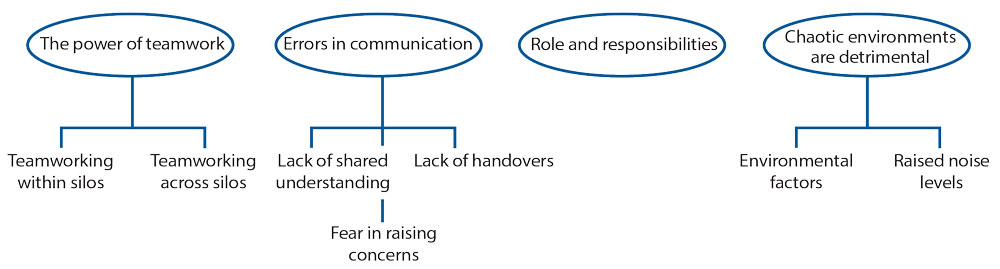
FIGURE 1 Key themes raised during debriefing.
Theme 1: Teamworking across disciplines
Teamworking was evident during the scenarios. Multiple scenarios demonstrated each team working effectively within its silo, displaying optimal communication strategies including closed loop feedback and role allocation. This display of effective communication may be attributed to previous training in human factors and simulation provided at the trust. However, teamworking was less optimal between teams; teams often did not know what other specialty teams were doing during the simulation. This manifested as a relative lack of collaborative decision making, shared understanding of the clinical scenario and appreciation for the priorities of other teams. An example of sub-optimal teamworking included the frequent lack in the completion of the obstetric surgical checklist ‘time-out’. Reasons for non-completion included the urgency to expedite delivery of the baby due to the deteriorating clinical situation plus a lack of knowledge as to the mandatory nature of the checklist.
During the debrief, the participants discussed the relevance of the obstetric surgical checklist, demonstrating a lack of knowledge of the mandatory nature during emergency deliveries in the operating theatre. This was expressed by all teams. Further discussion of the checklist revealed an anaesthetic focus resulting in key information being missed in relation to the obstetric and neonatal teams. An example of this was the lack of inclusion of the need for specialist equipment and nor was there understanding of the ‘category’ (urgency) or indication for delivery. This resulted in faculty and relevant stakeholders developing and introducing a revised obstetric surgical checklist inclusive of all teams.
Theme 2: Error in communication
Errors in communication were present within each simulated scenario. Teams experienced a lack of shared understanding about the level of urgency for delivery of the baby. As such various silos had a different perception of urgency. Participants failed to share pertinent investigation results with other teams (for example, an abnormal cardiotocography or CTG, showing a fetal bradycardia) or the clinical background (for example, sepsis in the mother or meconium liquor in labour). This lack of sharing of information led to confusion between teams and as such the desired course and urgency of action, resulting in teams not working in harmony but rather as disjointed silos.
When reflecting in debrief, participants discussed feeling unable to express their lack of understanding even when recognised in the operating room environment. On exploration they surmised that vocalising the category or urgency of delivery including the rationale was vital to fostering a unified action plan and efficiency of care. As a result, it was agreed that a vocalised discussion around the decision for the type of anaesthesia to be used was integral, which was added to the revised obstetric surgical checklist.
The simulations unveiled a lack of handover between the different teams, particularly in relation to the neonatal team. This absence of handover to the neonatal team resulted in neonatal staff having to request key information from the family or anaesthetic teams. Recognition of this during the debrief highlighted the importance of handover to the neonatal team primarily from the midwifery team. Subsequently, the revised obstetric surgical checklist was adapted to include neonatal concerns, gestation and relevant background.
Lastly, there was a reticence in junior staff to speak up about errors during the scenarios. An in-depth discussion revealed that junior staff (junior doctors and theatre staff) felt speaking in the high stakes, often loud environment felt challenging due to their perception of inferiority and sense of hierarchy. Rank and a sense of hierarchy are well known to decrease the ability of staff to communicate in emergencies, which will be additionally complex in a multidisciplinary environment.18 In the debriefing it was acknowledged that all staff should be empowered to raise concerns and that seniors should actively listen and invite questions or ideas from juniors during emergency situations.
Theme 3: Roles and responsibilities
The third extractable theme revolves around roles and responsibilities. During the scenario it appeared that each team understood the expectations of the wider MDT. However, discussion around the roles of others was fruitful during debriefing and uncovered discrepancies in the understanding of expectations from specialty groups. In scenario 1 (TABLE 2), which involved an extremely preterm delivery, both midwifery and neonatal teams felt it was the responsibility of the other to ensure the mother was expressing milk within an hour of delivery. During the debrief, it was outlined that responsibility is shared but in the immediate post-partum period, the bedside midwife should commence discussions pertaining to feeding. This has since been further explored and evaluated by the MatNeoSIP team (Maternity and Neonatal Safety Improvement Programme – a national initiative aiming to improve the quality and reliability of perinatal care) with a programme of education and facilitation being implemented.
Theme 4: Chaotic environments are detrimental
Environmental factors were reported as affecting performance significantly. Participants described a cluttered environment as stressful during the simulated scenario of the birth of an extremely preterm infant. As a result of this discussion the largest labour rooms have been prioritised for newborns expected to require neonatal resuscitation at birth. It was also agreed that non-essential equipment would be removed prior to the birth to optimise space.
Raised noise levels were reported as disruptive by participants. During one scenario, multiple conversations happening at once created a sense of chaos, which was distracting for teams performing procedures such as intubation, and listening for a heartbeat. It was agreed that while performing tasks such as intubation, quiet should be requested and respected. Emphasis was placed on the fact that there is a shared responsibility for ensuring this occurs.
Simulation has facilitated the introduction of new equipment and training of staff. The LifeStart platform (Inspiration Healthcare) was introduced as part of an initiative to improve delayed cord clamping rates. The platform was utilised in multiple MDT simulations, allowing the perinatal team to experiment and practise with all involved stakeholders. Latent errors were uncovered relating to the gas supply and the group reached a consensus about optimising future use. The gas supply was altered as a result. Simultaneously, interdisciplinary learning encouraged team and community building.
Discussion
MDT simulation has been met with enthusiasm by obstetric, midwifery, neonatal and theatre teams in our department and as a result, it has been integrated into current practice. Prior to the introduction of MDT simulation, the perinatal team rarely trained together. Multidisciplinary learning catalysed improvement in individual and team communication practices – the participants highlighted improved understanding of the communication requirements of other teams as a result of simulation. The negative impact of hierarchy on communication was noted and shared from the perspective of all perceived levels, solutions were considered and future changes in practice agreed.
Healthcare teams have been described as groups of expert individuals who, if not specifically educated, will form non-expert MDTs.19 The use of both mother and baby simulated patients allowed true-to-life scenarios and teamworking where multiple teams collaborated to resuscitate two patients simultaneously in the same clinical space. While individual teams focus on separate patients, there is a strong need for collaborative communication between disciplines to optimise understanding of the mother-baby dyad and inter-dependent health outcomes.
Multidisciplinary training allowed debriefing with all perinatal specialty groups. Individual specialty teams would previously debrief within individual silos, this limited the generalisability of learning and its use in future practice. MDT debriefing and discussion facilitated a shared understanding of the process by which mistakes were made. A more robust appreciation of the expectations and roles of individual teams during emergencies will act to improve future MDT practice and teamworking.
The chosen debriefing style was one of exploration and self-evaluation rather than critical judgement. As the group was a team of experts regularly collaborating in perinatal emergencies, this method aimed to encourage motivation, engagement and to utilise their expertise to consider solutions to identified learning needs. The literature relating to the degree of judgement shared by faculty is varied. The Diamond Method recommends a focus on positive behaviours and that undesirable behaviours are discussed with extreme caution.20 Alternatively, Rudoph21 recommends faculty utilise ‘good judgement’ and share their own ideas of best practice with participants after identifying the thoughts behind their actions.
One proposed barrier to simulation programmes is the lack of wider team participation and hesitancy for involvement, especially of experienced senior staff. However, in this instance the progressive success of the simulation programme resulted in increasing senior buy-in. Though initiated by individual consultants, fellows and practice development staff, the programme progressed to involve senior staff from all specialties. Currently all on-call consultants and senior nursing and midwifery staff attend simulations as participants. A full specialty faculty are engaged to support the writing and debriefing of scenarios. This has formed part of a culture of change in our department – embracing the opportunities that simulation offers.
The learning from the programme was limited due to the resource-intensive nature of simulation. A small number of staff attended each session (n = 8-13), limiting the accessibility of learning to the wider team. To mitigate this, key learning points were circulated in the form of posters and via email to the wider perinatal team and integrated into departmental teaching or utilised as a learning outcome in simulation at a later date.
Some sessions have been cancelled or rescheduled due to work pressures. While we have attempted to mitigate this by involving rota coordinators and seniors in the organisational process, this is not always possible. This has been recognised and met with extreme pre-organisation in management and funding. Rota coordinators are alerted six months in advance of simulation training to allow additional staffing during sessions, ensure teams are compensated and maintain patient safety. Senior management of all departments are aware staff must be released for sessions. Funding has been designated from the Ockenden fund ensuring the receipt of a training budget for simulation.
Conclusions
MDT simulation has become ingrained into departmental culture. This article presents our voyage and initial learning outcomes. The implementation of MDT simulation was achievable with the involvement of a dedicated educational MDT group and senior stakeholders. This journey can act as guidance for others in the introduction of MDT simulation locally. Key learning outcomes related to teamworking, communication, the roles and responsibilities of other teams and environmental factors. Successful MDT simulation requires active engagement, protected time, funding and planning.
Or read this article in our
Tablet/iPad edition
- With significant planning it is possible to integrate multidisciplinary perinatal simulation into departmental practice.
- This article can act as a guide for departments planning to initiate local multidisciplinary simulation programmes.
- Key learning outcomes focused on interdisciplinary teamworking, communication between disciplines, roles and responsibilities and environmental factors.
Also published in Infant:
