

Unwanted intrusive thoughts in the context of neonatal care: coping with the ‘what ifs?’
As neonatal psychological professionals, we are hearing of increased levels of intrusive thoughts of harm in both neonatal staff and parents since the Lucy Letby trial. This increase makes sense in light of what we know about the experience of intrusive thoughts. Understandably, these thoughts can lead to high levels of anxiety and can start to undermine confidence and trust in ourselves and others. This paper aims to help colleagues understand what these thoughts are, how they arise, normalise experiencing them and reduce anxiety about their relationship to actual harm.
Fiona L. ChallacombeLecturer in Perinatal Clinical Psychology, King’s College London, in conjunction with the Neonatal Leads for Psychological Practice (NeoLeaP; TABLE 1)
fiona.challacombe@kcl.ac.uk
Challacombe F.L., Chilvers R., Butterworth R., Atkins E., Barr K., Cole S., Cordwell J., D’Urso A., Evans D., Higgins S., Marsh A. Unwanted intrusive thoughts in the context of neonatal care: coping with the ‘what ifs?’ Infant 2024;20(1):16-19.
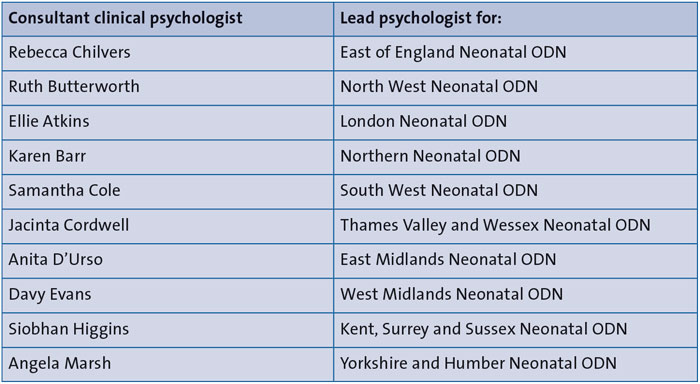
TABLE 1 The English Neonatal Leads for Psychological Practice (NeoLeaP).
“But what if they harm the baby?”
Distress is a familiar companion in neonatal care for families and staff alike. The infants in our care are often fragile and the risk of harm occurring is a source of fear for many. It is not surprising, therefore, that both staff and families experience intrusive thoughts about harm. ‘Intrusive thoughts’ is a broad term used to describe unwanted and uninvited thoughts, images or urges that might feel highly upsetting, unacceptable or shameful. These can relate to something terrible happening, either by making a mistake or by deliberate actions. Distressing intrusive thoughts are in direct opposition to what a person intends to do or what they want.1
Intrusive thoughts in the context of threat: parents
Becoming a parent involves being responsible for a vulnerable infant in the context of threat and uncertainty. It is normal for new parents to experience upsetting and unwanted thoughts about negative things that could happen to their infant. Almost all new parents experience intrusive thoughts (or images or impulses) of accidental harm coming to their baby. However, it is also very common for parents to experience intrusive thoughts of deliberately harming their baby. Intrusive thoughts of either type can lead to an increase in caution and in behaviours intended to protect the baby (eg excessive cleaning, avoiding contact, delegating care tasks to others, repetitive checking, seeking reassurance).2 These experiences may be part of an evolutionary protection mechanism, which drives parental attention to enhance protection of the infant.3
For neonatal parents the vulnerability, threat and uncertainty of the postpartum period are hugely intensified, and often compounded by the trauma of medical care for the mother, their baby or others on the unit.4 A reduced opportunity to fulfil multiple aspects of their parenting role and responsibilities in the neonatal context (particularly in intensive care) comes at exactly the point when the need to nurture and protect are highly activated. The impact on mental health for those parents beginning their postnatal journey in neonatal care is starting to be better documented, with recent research highlighting that about 40% of parents experience clinical levels of anxiety, post-traumatic stress and depression for months and possibly years following discharge.5,6 Importantly, our own studies have also highlighted that unwanted intrusive thoughts of both accidental and deliberate harm are very common for neonatal parents both on the ward and post-discharge. Investigating parents while on the unit, Childs et al (unpublished doctoral thesis) found that 67% of neonatal parents reported a clinical level of severity of intrusive thoughts and compulsions (ways of trying to manage these thoughts) at 1-2 weeks post-birth rising to 94% at 4-6 weeks and the impact increased over time.7
Intrusive thoughts in the context of threat: neonatal staff
It is not only parents who are exposed to increased levels of threat in the neonatal context. Neonatal care is a high-risk, high-stakes environment where outcomes are often uncertain. Staff are under increased scrutiny in the context of a range of high-profile court cases and a culture of fear and shame is often pervasive.4,8 We know that some healthcare professionals are, by the nature of their work, more vulnerable to intrusive thoughts (see below), and it is unsurprising that we are hearing anecdotal reports of an increased experience of these on neonatal units.
After a traumatic event, it is not uncommon for people to feel a generalised sense of unease, experience intrusions (eg unwanted memories or thoughts about imagined scenarios) about the event and about similar things happening in the future. Often people will increase compulsive-like coping behaviours such as checking and washing in order to try and create a sense of safety.9 Parents may come to the unit after a traumatic pregnancy and birth, and both staff and parents in the neonatal unit can be exposed to a high number of further traumatic events once there.
Unwanted intrusive thoughts: what they are and how they can lead to cycles of distress
Intrusive thoughts are experienced by 90% of the general population.1 The content of specific thoughts tends to be themed around what is personally meaningful to the individual, aligning with experiences of threat, uncertainty and personal responsibility. That is to say, they tend to be about what matters most to people. Therefore, it is not surprising that for new parents, their intrusive thoughts usually centre around their baby. In our study, which predates the Lucy Letby trial by five years, neonatal parents reported themes of accidental harm and contamination of their baby, but also noted intrusive thoughts of deliberate harm, by their own actions and those of neonatal staff.7 The fear of something going wrong, or someone doing something wrong is very normal in the context of caring for a highly vulnerable infant.
Although almost everyone has occasional intrusive thoughts of the worst happening, they elicit differing levels of distress and responses in individuals.10 It is the meaning given to the thought that drives reactions. While many parents have intrusive thoughts that their baby could be harmed, some may feel mild discomfort but not dwell on that thought or change their behaviour.11 Where having the thought is interpreted as giving a meaningful message, either about the situation (“I’ve had this thought so it could happen”) or the person experiencing them (“Having this thought means something awful about me”), they can be given more weight and lead the person to try and do or think something to relieve the anxiety caused (“I have had this image of something bad happening and it would be irresponsible not to do something to prevent it” – see FIGURE 1). People can be particularly distressed if the thought seems to violate their sense of self or moral code, and they lack a framework to make sense of why this thought has occurred to them.
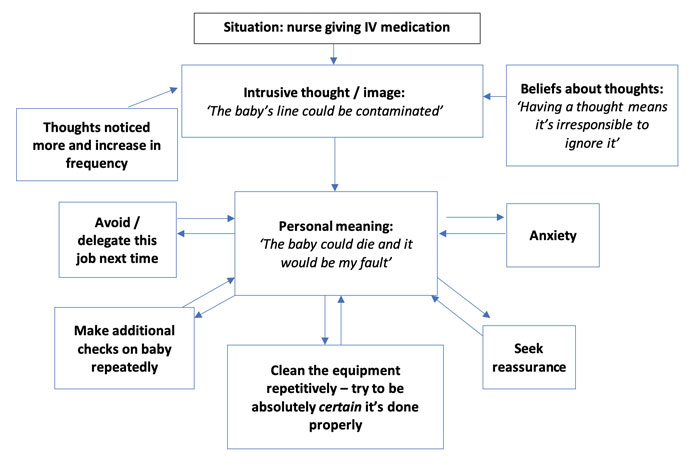
FIGURE 1 This model shows relationships between intrusive thoughts, their meaning and the feelings and behaviours that result for a common scenario in a neonatal unit (after Salkovskis 199912). The arrows are a series of ‘vicious circles’; each emotional or behavioural response makes sense given the meaning, but also inadvertently reinforces it and keeps the person in a state of threat. Past experiences and pre-existing beliefs underlie the meaning given to thoughts.
Due to the importance of the outcome, standards of absolute certainty are often applied (“I need to be completely sure it’s ok or the baby could die”). In this way, people can start to get drawn into cycles of responding that can (inadvertently) lead to more anxiety, uncertainty and intrusive thoughts as they try too hard to be certain or safe. They pay more attention to their thoughts as they are flagged in the mind as needing action. People may become preoccupied and routine activities can take much longer than needed. The impact may also be felt outside the unit: rest and sleep may be affected, which could make parents or staff more fearful of making errors, thereby also increasing self-doubt and intrusive thoughts. Obsessive-compulsive disorder (OCD) is the term for when intrusive thoughts and responses become repeated patterns that are difficult to change or interrupt and interfere with day-to-day functioning.
Neonatal professionals can also be considered to have a very high level of responsibility for the vulnerable infants they care for. FIGURE 2 outlines some examples from neonatal units. The context of having personal responsibility for an outcome enhances the meaning of intrusive thoughts.13 There is evidence that some people in professional roles with high levels of responsibility towards others in their care, such as medics, pharmacists and other healthcare professionals, are also prone to intrusive thoughts and may get caught in these cycles.14
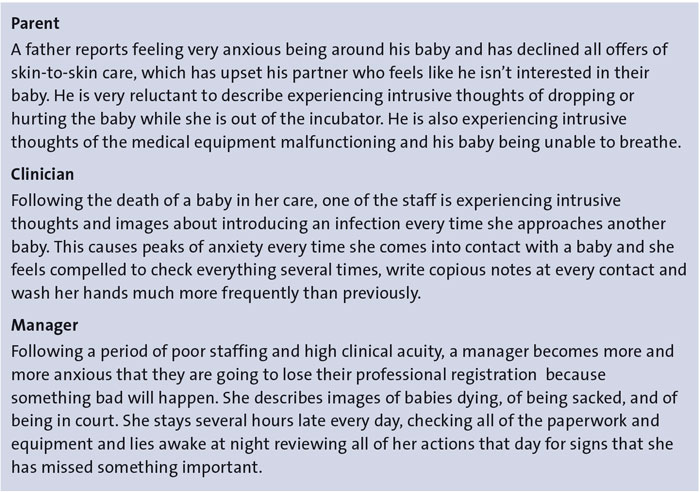
FIGURE 2 Examples in practice.
A focus on thoughts of deliberate harm
The experience of occasional unwanted intrusive thoughts of deliberate harm are reported by about half of new parents in the general population.2 These intrusive thoughts are not related to actual aggression or harm towards the baby15 and there is a clear distinction between thought and action – there is no known evidence of people with OCD acting on their intrusive thoughts.16 Intrusive thoughts by their nature frequently include topics that elicit high levels of disgust or shame, eg thoughts/images of sexual acts or violent harm, in direct opposition to a person’s intent or value system. Intrusive thoughts of this nature seem to arise frequently in the perinatal period due to a communal notion of society’s worst fears of what a parent could do.17
Trust and certainty undermined
The idea that anyone could act harmfully in a deliberate way towards children, and especially in the context of neonatal care, is for most people unthinkable. However, recently in an extremely rare case, a nurse was convicted of this, violating all contracts of trust and morality. When something so painful happens, it is normal for those either working or receiving care in this context to look for signs or signals in the hope of preventing it happening again.
Often those experiencing intrusive thoughts will engage in processes of questioning themselves or others (FIGURE 3): “But how can I be completely sure I won’t act harmfully?” It is not possible to be absolutely sure that a person will not do something, but in general life we do not need or seek such assurances. Seeking complete certainty is counterproductive as it increases doubt and distress in our relationships with ourselves and others. It also often has the double bind of moving us further away from our personal values or what is important to us (eg our value might be to be a caring doctor but the time spent checking equipment/medication means we are less connected to our patients and colleagues). Repeated checking can also itself undermine ‘sureness’ that something is safe18 – careful work and some checking is of course essential to many protocols on neonatal units. However, excessive checking that goes beyond this can make us feel less sure and then driven to check more.
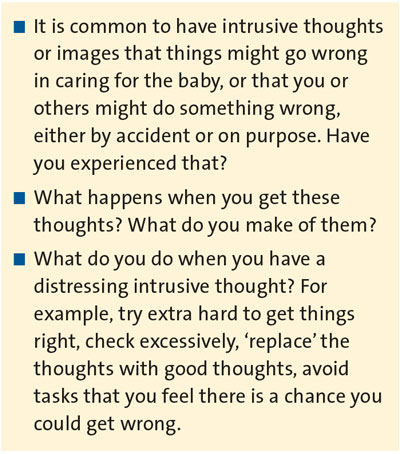
FIGURE 3 Useful questions for understanding intrusive thoughts.
The Lucy Letby case has undermined the trust that is fundamental in health care, and it will likely take further time to restore. Healthcare professionals are often especially conscientious, thoughtful and caring, which is why experiences of intrusive thoughts may be particularly common following such an enormous systemic shock. Rebuilding trust both within and between parents and professionals will be key.
Conclusion
While distressing intrusive thoughts are common both in new parents and healthcare workers, the current environment in neonatal care may be amplifying this phenomenon. Although hearing about intrusive thoughts may cause some anxiety, it is key that professionals recognise what these mean, and where parents and staff are brave enough to share their experiences, that they are received and supported with empathy (FIGURES 4 and 5).
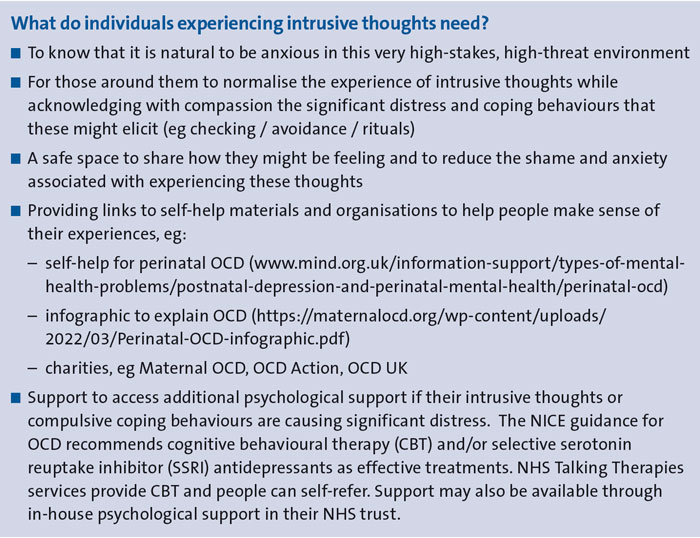
FIGURE 4 Help for individuals experiencing intrusive thoughts.
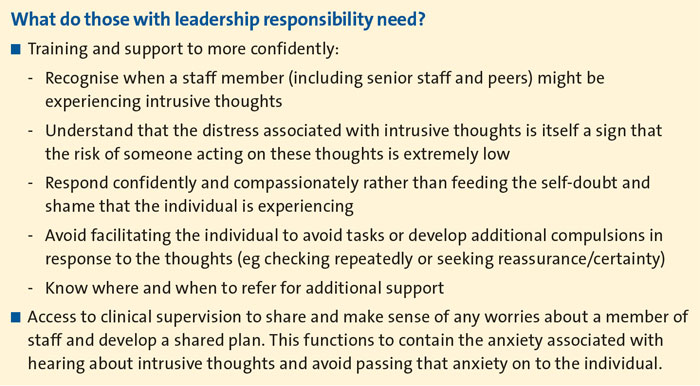
FIGURE 5 Help for managers, professional nurse advocates, freedom to speak up guardians or others with leadership responsibilities.
Or read this article in our
Tablet/iPad edition
- Intrusive thoughts of infants being harmed are common in new parents and in healthcare professionals.
- Thoughts can be about accidental or deliberate harm by self or others.
- People feel distress about intrusive thoughts that they do not want to happen and will not act on.
- Reducing threat in the environment and responding compassionately to these experiences will help to reduce the impact of intrusive thoughts and prevent them interfering in the care of the infant.
Also published in Infant:
