

BadgerNet admission data entry: a quality improvement project
Completion of BadgerNet data is important for every neonatal unit yet often it is incomplete and the quality/accuracy of the data could be better. The aim of this quality improvement project was to monitor accuracy and compliance with National Neonatal Audit Programme (NNAP) data and to audit the accuracy of BadgerNet admission summaries. The project assesses outcomes in the local neonatal unit at Kettering General Hospital before and after the formal introduction of a set of improvement measures.
Edward Artley
MBChB
ST2 Paediatrics
Kainaz Singh
MBBS, MRCPCH
ST8 Paediatrics
Poornima Pandey
MBBS, DCH, MRCPCH
Consultant Paediatrician
poornima.pandey@nhs.net
Neonatal Unit, Kettering General Hospital NHS Foundation Trust
Background
BadgerNet Neonatal forms a single record of care for all babies within neonatal services. It is currently in use in over 250 hospitals throughout the UK, New Zealand and Australia. From admis-sion data to everyday care, it provides a comprehensive record of all care delivered to neonates from intensive to special care and provides follow up records for all of these infants. Good quality BadgerNet data ensure a better quality of care for babies and their parents, and can stimulate quality improvement (QI) projects.
To assess whether babies admitted to neonatal units in England, Scotland and Wales receive consistent high quality care, the National Neonatal Audit Programme (NNAP) publishes annual reports based on audit measures, which identify areas for QI in relation to the delivery and outcomes of care.1
NNAP uses routinely collected data to support QI in neonatal units of all types. Units can use their NNAP data as a driver for change and an opportunity for QI activities and regular review to measure improvement progress.
Aim and objectives
The aim of this QI project was to monitor accuracy and compliance with NNAP criteria and to audit the accuracy of BadgerNet admission summaries. Admission summaries are a good area to focus a BadgerNet data quality review as many of the NNAP criteria are set at the point of admission, in particular:
- Are all mothers who deliver babies between 24 and 34 weeks’ gestation inclusive given any dose of antenatal steroids?
- Are mothers who deliver babies below 30 weeks’ gestation given magnesium sulphate in the 24 hours prior to delivery?
- Does any admitted baby born at less than 32 weeks’ gestation have its first measured temperature of 36.5 to 37.5°c within one hour of birth?
- Is there a documented consultation with parents by a senior member of the neonatal team within 24 hours of admission?
Completion of these criteria on the initial admission data was recognised as a key quality indicator. This information should be readily available within 24 hours of admission. Failure to enter this information within this timeframe might infer that there is delay in delivery of care.
It also increases the risk of information being lost, a breakdown in communication between teams, and loss of data pertaining to the quality of care being delivered. Therefore, the next key quality indicator identified was:
- Time to completion of the admission summary including a brief history, physical examination and initial management plan.
Methodology
Project design
The PDSA (plan, do, study, act) cycle and model for improvement was used to guide the project.
Four episodes of retrospective data collection were used to analyse the admission summaries of every baby admitted to the local neonatal unit (LNU) at Kettering General Hospital. The first two episodes covered all neonatal admissions in the months of April 2018 and June 2018.
Data collection was completed using the audit-trail function on BadgerNet, which can track every data entry point of each registered user with an accurate time of entry. To ensure validation of clinical summaries a random selection of five physical notes per month were assessed. This ensured that the data entered on the clinical summaries matched that of the physical notes. To assess if any improvements are maintained and embedded into practice, we repeated a second wave of audits for October and November 2018.
Participants
In total 24 babies were admitted in April 2018, and 22 babies were admitted in June 2018. These included babies requiring different levels of care, irrespective of their duration of stay. Babies on intravenous antibiotics on the postnatal ward were not included. In the second wave there were 20 babies admitted in October 2018 and 15 in November 2018.
Implementations
As part of the QI project a set of implementations was formally put into effect on the 1 May 2018, which comprised the following:
- a BadgerNet information proforma sheet was designed (FIGURE 1), which helped as a data collection aid and a prompt to ask whether NNAP criteria had been met antenatally, as well as other information required for the admission summary completion
- a new local policy that every BadgerNet admission summary should be reviewed by a paediatric trainee grade ST4 and above (middle grade level)
- the creation of ‘Badger champion’ roles at senior house officer and registrar grade position, who will regularly assess data
on an informal basis, and instruct non-paediatric trainees in the use of the BadgerNet system
- an education package at induction regarding the use of the BadgerNet system and use of the proforma sheet.
We also conducted an online survey of all junior trainees in November 2018 for feedback on the proforma sheet, to recognise any short-comings and to permit further changes.
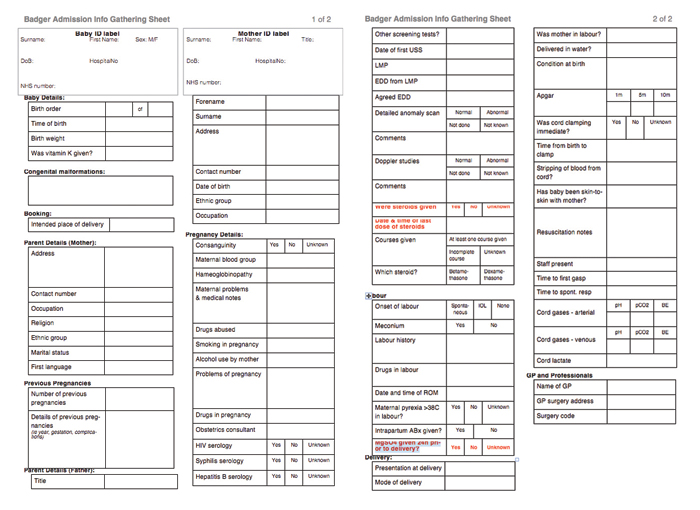
FIGURE 1 The proforma – designed to aid data collection for BadgerNet admission summaries.
Assessments and outcomes
The following outcomes were identified as indicators of quality of admission data:
- proportion of admission NNAP criteria completed on initial admission summary
- time to completion of admission summary from point of admission to unit
- proportion of admission data entries that include a physical examination and clinical plan in the summary.
These outcomes can be directly compared to one another as a key indicator of admission data quality.
Results
NNAP criteria
In the first wave (April and June), there was an increase in completion rates for every NNAP criterion outcome following the introduction of the improvement measures (FIGURE 2). There was an improvement in documentation for all the NNAP criteria:
- use of antenatal steroids increased from 71 to 91%
- recording of admission temperature increased from 75 to 82%
- parental discussion in the first 24 hours increased from 79 to 95%
- there was a marked improvement in the documentation of magnesium sulphate administration from 46 to 77%.
In the re-audits of October and November improvement in entry of admission criteria was sustained for most of the data entry but there was a decline in some of the admission data entry in November, notably antenatal steroids and parental discussion.
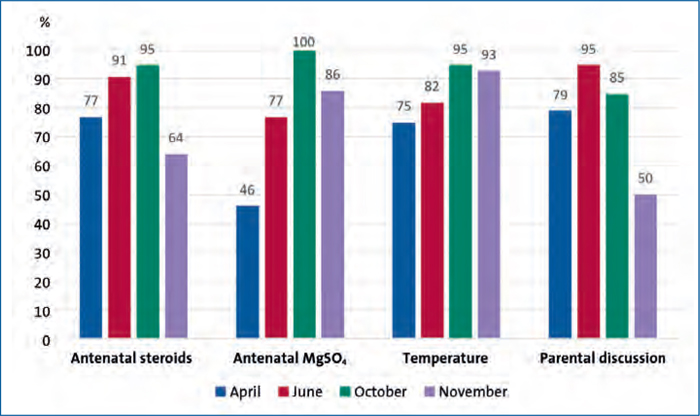
FIGURE 2 BadgerNet entry of admission criteria.
Time to completion
When comparing April and June, there was a 7% increase in admission summary completion within 12 hours of admission; however, there was a 5% increase in those completed more than 24 hours after admission (FIGURE 3). In November only 57% of admission summaries were completed within 12 hours and 86% were completed within the target of 24 hours.
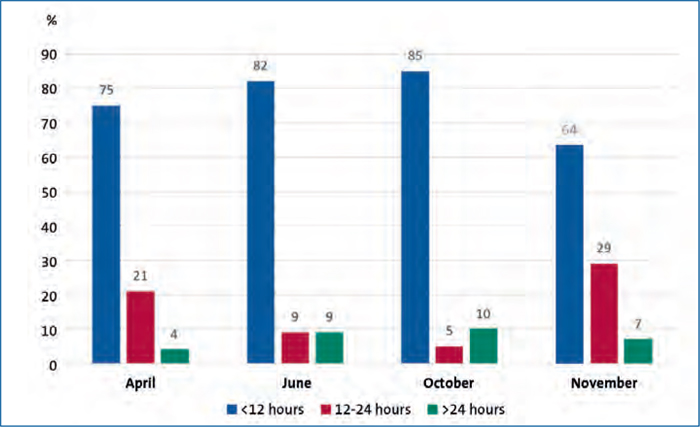
FIGURE 3 Time to completion of admission summaries.
Admission summary completion
When comparing April and June, there was a 36% increase in the proportion of BadgerNet admission summaries containing a clinical examination summary (FIGURE 4). In October and November there was 100% clinical summary completion.
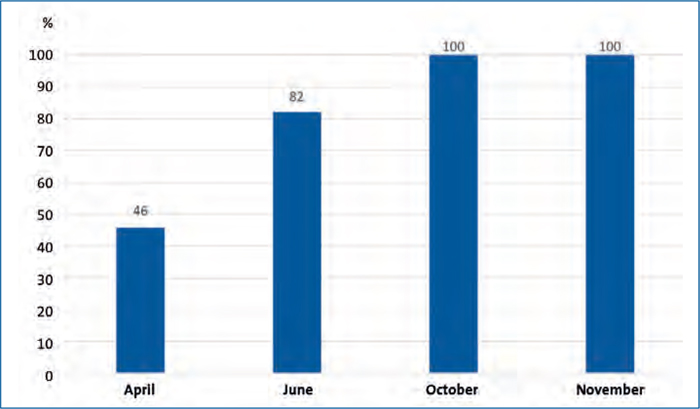
FIGURE 4 BadgerNet admission summaries containing a clinical examination.
Results of online survey
We surveyed all junior trainees for feedback on the proforma sheet in November; nine out of 14 responded. Disappointingly only 44% said they used the proforma to collect data (FIGURE 5). In the previous four months, respondents had used it:
- most of the time = 22%
- sometimes = 22%
- rarely = 33%
- never = 22%.
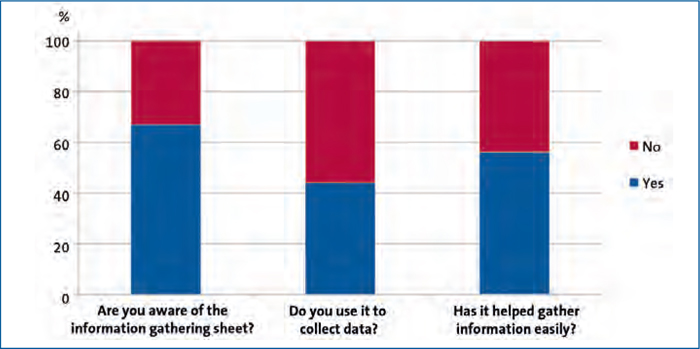
FIGURE 5 The online survey findings.
Some of the comments reflected a sense of duplication of work, accessibility to the sheets and availability in different clinical areas; however, there was a general willingness to continue use of the proforma. Based on the recommendations and suggestions from the survey, we raised awareness of the proforma, made it easily accessible on the neonatal unit and labour ward and also put in steps to ensure it was highlighted in the induction package for junior doctors. It has also been added on to the paediatric shared drive for trainees, which allows easy access. Perhaps a longterm solution is to enable use on the labour wards on mobile tablets and we are in contact with the trust IT department to make this possible
Discussion
The NNAP brings together a multidisciplinary, multiagency group to translate key findings and results into recommendations that can be acted upon to improve neonatal care. Recommendations support the existing goals and priorities of neonatal and perinatal services and outline areas where healthcare professionals in neonatal units must improve.2 Accurate and complete BadgerNet data is key for this to occur.
This audit shows that the timeliness and quality of BadgerNet admission data can be improved by the introduction of an educational package. Shortterm improvements are good but these must be sustainable. Overall in this QI project we noted an improvement in data entry compared to preimplementation of the education package. This can be seen in the increased proportion of NNAP criteria completed and an increased proportion of admission summaries completed within the first 24 hours. However, we need to formulate ways to ensure that some data entry points that have a low rate of data input can be increased, for example parental discussion.
At present, the majority of junior doctors work full shift patterns. In LNUs there are GP trainees who work on the neonatal unit for two months during their four-month paediatric rotation and are not aware of the BadgerNet database. Hence this has been a timeintensive exercise – to train junior doctors in a short period of time and also continue to reinforce training every four months. There have been difficulties in assigning roles of BadgerNet champions in view of shift patterns. In order to maintain a sustainable digital service for the future, we need successful adoption of initiatives to ensure accurate data entry. This requires alignment of leadership and culture change to match with needs and expectations.
There are approximately 182 neonatal units in England, Scotland and Wales including 88 level 2 LNUs such as the one featured in this study. While local practice will inevitably vary between units, it is hoped that the measures implemented in this study will be of consideration. Challenges remain to ensure that this progress continues on a regular basis and forms part of ongoing reviews.
Acknowledgement
The authors wish to thank Lisa Wallberg (ST3 Paediatrics) for designing the BadgerNet proforma sheet and Sara Hales (Senior Neonatal Administrator) for helping with data collection.
Or read this article in our
Tablet/iPad edition
- Accurate data entry enables effective benchmarking of quality of care.
- Prompt and high quality data input driven by a shared ownership will ensure timely updates and effective communication.
- Successful adoption of initiatives into practice must be sustainable. Ongoing review will ensure that progress continues.
Also published in Infant:
