

The anatomy of compassion part 2: nurturing compassionate cultures of maternity and neonatal care
The NHS England Three Year Delivery Plan for Maternity and Neonatal Services1 prioritises compassionate care for families and compassionate cultures for staff. In a previous article, we proposed a shared language and understanding of the complexities of practising compassion in this context and why it can feel hard to do.2 In the following article, we outline what is required to take practical steps – at each level of the system – to foster compassionate care in maternity and neonatal services.
Neonatal Leads for Psychological Practice in England’s Neonatal Operational Delivery Networks (see TABLE 1)Evans D, Butterworth R, Atkins E, Barr K, Chilvers R, Cole S, Cordwell J, D’Urso A, Higgins S, Marsh A. The anatomy of compassion part 2: nurturing compassionate cultures of maternity and neonatal care. Infant 2023; 19(6): 213-18.
See also part 1: The anatomy of compassion: courage, connection and safeness in perinatal practice. Infant 2023; 19(3): 88-92.
TABLE 1 This report was produced by the Consultant Clinical Psychologists listed in their roles as Psychology Leads for the Neonatal Operational Delivery Networks (ODNs) across England.
Maternity and neonatal services provide care for families at a hugely important point in their lives. Infants and their families are cared for with great skill and expertise. At the same time, threat – including uncertainty, change, risk or loss – pervades the perinatal period.2 This threat is amplified for infants, families, staff and organisations by many situations (feared/imagined and actual). For example, when:
- an infant needs intensive medical care
- a family’s previous perinatal trauma is triggered
- staff are exhausted
- organisations have limited resources or feel pressure to ‘perform’
- societal events such as the COVID pandemic place restrictions on how care is offered.
The recent conviction of a neonatal professional for intentionally harming and killing babies on a neonatal unit in England has sent shockwaves of threat throughout the system, potentially undermining the trust between families and staff that is so pivotal for effective neonatal care.3
As threat escalates, our minds respond by switching into a survival-focused mode of rigid thinking, feeling and acting. This makes it harder to connect with others or to be open with each other about our doubts or mistakes. The quality of care, and the system’s ability to learn and improve, suffers.
However, just as relationships are undermined by threat, they are also the route back to a more balanced state of mind. The social engagement system that is wired into our brains and bodies allows us to be soothed by compassion when we feel overwhelmed, enabling us to feel safeness and compassionate courage when facing adversity. In turn, this improves outcomes – effective team working, job satisfaction and motivation, creative and effective problem solving and, ultimately, improved patient experience.
The challenge is how to engage and sustain this compassionate mind. How do we remain sensitive and open to the struggling parts of ourselves, of the infants and families we care for, of our colleagues, and of our institutions while finding ways to helpfully respond? How do we resist the urge to avoid the threat without becoming engulfed by it? How do we bring soothing and safeness to ourselves and those around us to find more balance?
In essence, how do we enact compassion in practice? The UK Government’s response to Bill Kirkup’s review of maternity and neonatal services in East Kent recommends that work is undertaken to ‘report on how compassionate care can best be embedded into practice’.4 This article is a statement of our position on this question.
The challenge of adapting our ways of working may feel like an overwhelming task, especially when it might invite us to become more aware of our own struggles. For readers who feel courageous and would like to explore these ideas further, links to additional resources can be accessed via the QR code. These resources are signposted throughout this article as Padlet#.
Links to additonal resources can be accessed via the QR code or at https://padlet.com/NeoLeaP/anatomy-of-compassion-links-and-resources-dsxf3gvvezxa0e32

A relational approach
To understand practical steps towards compassion, it is important to appreciate the connected and reciprocal nature of a relational system such as maternity and neonatal care (FIGURE 1). Within a culture of family-integrated care, infants are cared for by their families, who are cared for by multidisciplinary teams of staff, who are cared for by their organisation. A process of mutual influence occurs across all these layers of the system: the needs and actions of one layer influence all other layers. Soothing can percolate through the system through a process called emotional containment: “Where a person receives and understands the emotional communication of another without being overwhelmed by it and communicates this back to the other person.”5
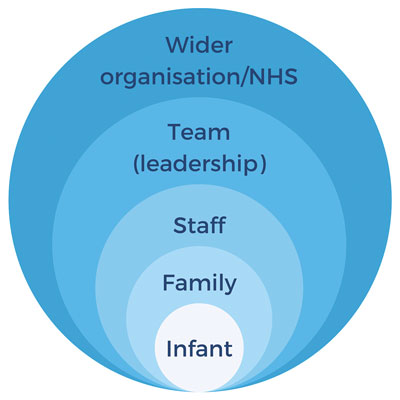
FIGURE 1 The interlinked system of relationships in maternity and neonatal car.
But threat can also percolate through this system. When dysregulated by threat, our emotional arousal is high and our ability to be open to our own inner worlds and those of others (a skill called mentalising) becomes more rigid and impaired.6 Emotional containment is lost, and threat trickles up and down the system (FIGURE 2).
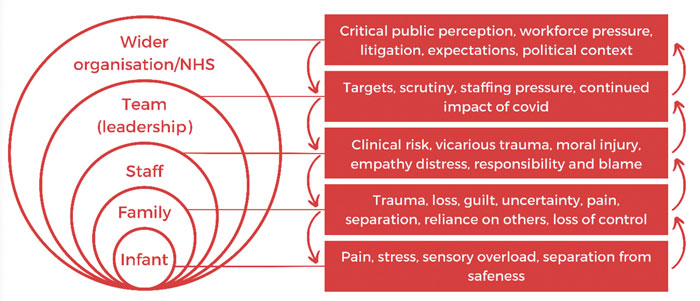
FIGURE 2 Some of the sources of threat in maternity and neonatal care and how these percolate through the system.
Compassion across the system
In this context, we can use our compassionate mind to bring soothing and safeness to experiences of threat, enabling all levels of the system to re-establish skills of mentalising and social connectedness. This commitment to compassion allows soothing and containment to filter through the system (FIGURE 3).
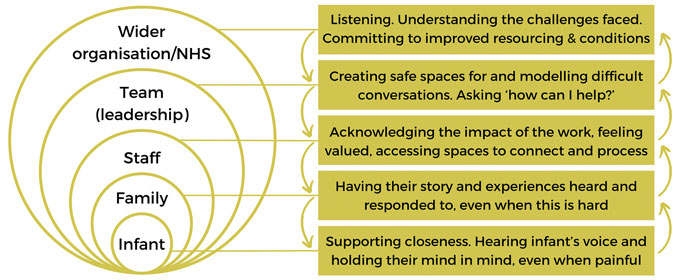
FIGURE 3 Some of the commitments of the compassionate mind to bring soothing to threat in maternity and neonatal care and how this percolates through the system.
When the organisation nurtures a psychologically safe environment for staff, those staff feel more contained, which reciprocally allows them to work in collaborative and prosocial ways, contributing to that psychologically safe environment. Similarly, staff who are experiencing soothing and safeness are better able to provide care that is compassionate, meaning families feel safer and more contained, contributing to collaborative relationships with the staff team.
One key practical implication of this is that compassion is not something that we practise in isolation. There is a need for approaches across all levels of the system to bring about cultures of compassionate care.
Practical steps towards compassionate systems
Wider NHS
An NHS system that engages compassion-ately with its patients, staff and organisational partners will set the tone and create the context for psychological safeness to flourish. When senior managers at a national, regional and local level listen to the experiences of staff and service users with openness and curiosity, and prioritise collaboration over competition, there is greater dialogue and containment in the system.
This begins with a commitment to ask and hear about what it is like to provide and receive care in a service. It requires a willingness to acknowledge the challenges faced by service users and staff, even when this is uncomfortable, and to invest in meaningful co-production of services. This can be thought of as ‘compassion through commissioning’ as illustrated by the provision of a well-resourced specialist psychology service within the Shrewsbury and Telford independent maternity review to ensure families had ‘an opportunity to feel that their experiences had been listened to and heard’.7
Organisations and teams: leadership and culture
Staff in leadership positions have a crucial role to play in creating compassionate cultures in health care. A compassionate, inclusive and collective approach to leadership is clearly outlined by West,8 underpinned by leaders’ commitment to attending to, understanding, empathising with and helping their teams’ needs. Such leadership aims to foster experiences of autonomy, belonging and contribution in a team, which contribute to improved clinical outcomes by creating an environment where teams feel safe to disagree, to admit mistakes and vulnerability, to not have all the answers but seek true collaboration and ultimately to ask each other ‘how can I/we help?’ rather than ‘where have you failed?’
One means for fostering compassionate team culture involves a ‘top-down’ approach of providing training and support to individuals in leadership positions. A number of such programmes exist, including the Maternity and Neonatal Culture and Leadership Programme (www.england.nhs.uk/culture/culture-leadership-programme) and a number of courses provided by the King’s Fund (www.kingsfund.org.uk/courses). These trainings offer a combination of teaching and reflective practice, integrating a consideration of the self with a framework of compassionate leadership.
More ‘bottom-up’ approaches to developing inclusive team culture and relationships include the ProSocial method,9 which facilitates groups of people to learn flexible ways of collaborating within their team and with other teams. ProSocial engages with the reality that many behaviours that interfere with collaborative team working are motivated by avoidance of threat. The method fosters flexibility, openness and dialogue in a team’s collective and relational practices, centred around core evidence-based principles that promote cooperation. Stories of ProSocial in practice illustrate the significant cultural impact the approach has had across one NHS Board in Scotland (Padlet1).
Staff
The experience of many families using maternity and neonatal services is of excellent care from dedicated, skilled and compassionate professionals. But recurrent public government inquiries over the years have demonstrated that this is not a universal experience for all families, and that there are systemic blocks to compassion in maternity and neonatal care. As described by Evans et al,2 acute or chronic activation of brain/body responses to threat can make it harder for us to practise compassion. Healthcare staff need opportunities to connect with experiences of soothing (from self and other) to regain the capacity for compassion in the face of threat. Some examples of these soothing and connecting experiences include:
- sharing food and drink together as a team
- tea trolley rounds with space to talk
- colleagues offering cover to give each other a moment to breathe
- celebrating successes together
- being mindful/aware of those that are having a difficult day and letting them know it has been noticed/asking what they need to get through the shift
- saying thank you, or demonstrating appreciation
- sub-teams (sometimes referred to as ‘family teams’) to create safeness within large staff groups
- regular ‘check ins’ alongside colleagues (eg at handover and during challenging clinical tasks such as overseeing and supporting end-of-life care) (Padlet2, Padlet3).
Further to these brief and often spontaneous ‘micro-compassions’, there is compelling evidence for the benefits to healthcare staff of accessing more structured, facilitated spaces to acknowledge and explore challenges in their work. In doing so, staff are able to feel safeness, calm, self- and collective-efficacy, hope and connection with support – experiences that are understood to be protective in the face of trauma.10 These spaces can be reactive:
- Post-event team reflection following a particularly difficult episode of care. This requires careful framing to avoid causing psychological harm. Guidance for the delivery of safe post-event team reflection led by trained professionals has recently been published.11
Or more proactive and preventative:
- Compassion practices provide a safe and supportive space to slow down, connect with and listen to each other, with a focus on caring for ourselves and our colleagues (www.compassionpractices.net).
- Reflective practice involves an exam-ination of diverse perspectives on particular aspects of work (eg dilemmas, challenges or successes) with the intention of broadening and deepening our understanding of what we do. Attendance at well-facilitated reflective practice groups is associated with improved professional quality of life for nursing staff.12
- Clinical supervision offers containment (the ‘restorative function’), opportunities for learning and developing (the ‘formative function’) and safe governance of our work (the ‘normative function’).13 Clinical supervision has demonstrated efficacy in reducing stress and burnout and improving compassion satisfaction for non-psychological professionals.14 For most psychological professionals, supervision is a requirement of the code of professional practice. For clinical supervision to be safe and effective, clear agreement around expectations is important, as is a cascaded approach in which supervisors receive supervision and training for this work (‘supervision of the supervision’).
More explicit training in application of the compassionate mind approach is also a helpful and viable approach to fostering compassion in healthcare staff.15 Such training in the skills and practice of compassion has been shown to increase prosocial, cooperative behaviour and also enhance neural networks supporting mentalising skills, goal-directed behaviour and positive emotions.16
There is evidence that both reflective space and training in psychological skills can reduce staff burnout and compassion fatigue.17 A combined approach of training and reflective space, provided by clinical psychologists, has been reported to have resulted in a 40% reduction in the cost of sickness absence on a neonatal unit.18 Therefore, it is our view that the most effective means of directly facilitating the skills and practice of self- and other-focused compassion in the maternity and neonatal workforce is threefold (TABLE 2).
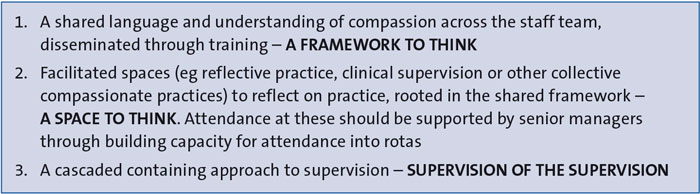
TABLE 2 An approach for facilitating skills for compassion in the maternity and neonatal workforce.
Feedback from one member of a neonatal team who engaged in this work from a clinical psychologist working on their unit, illustrates the value of this coordinated approach:
“These sessions help me process and understand why families may be going through these traumas… I have felt so much more able to process what I am having to deal with. As a leader, it has helped me to understand how my team are thinking and feeling… particularly when someone from the team has taken on a heavy burden of a particular case. It has also supported our team's relationship as we all reflect on how we deal with certain situations, which has enabled us to develop a deeper empathy for each other.”
Staff-family relationships
One area that can become particularly problematic when compassion becomes derailed and emotional containment lost, is the relationship between staff teams and families. Threat can escalate conflict and hostility, impacting on shared decision-making and the quality of care.
Rupture in the professional caregiving relationship is helpfully understood through the frame of mentalising. For both families and staff, the experience of acute distress makes it harder to consider the other’s perspectives, motivations and intentions, leading to more superficial and mis-attuned understandings (eg family: ‘they don’t care’; staff: ‘they are being difficult’). The development or maintenance of trust is impeded.
Engaging with the compassionate mind and bringing soothing to these experiences of threat can restore people’s capacity to see each other as human and maintain curiosity about others’ inner lives, contributing to the repair of relationship rupture. This may be supported for staff through reflective practice, clinical supervision or compassion-focused training and practices, and for parents through psychological intervention.
There are some additional strategies that can aid in the repair of relationship rupture (Padlet5). For example, ‘team formulation’ is a process, usually facilitated by a psychological professional that collectively constructs a shared team understanding of a particular family’s psychological needs and how these might be met by a team intervention plan. In mental health settings, team formulation has been shown to result in less restrictive team interventions and improved clinical outcomes for service users.19
Families
A detailed discussion of the direct psychological and social-environmental interventions that can increase soothing and compassion for families is beyond the scope of this article. However, there is good evidence for the effectiveness of compassion-focused therapeutic inter-ventions across a wide range of presenting difficulties,20 and these should be accessible to family members who encounter psychological difficulties in maternity and neonatal services. There is a need for robust mechanisms to identify and support family members experiencing psychological distress. Where the need is complex, psychological professionals with specialist expertise should offer support.21
Infants
A system-wide engagement of the compassionate mind across maternity and neonatal care will provide a conducive environment to support close and connected relationships between parents and their infants, providing a buffer to their own experiences of toxic stress and ultimately improve their clinical, psychological and neurodevelopmental outcomes. In order for the system to bring a compassionate mind to infants, we need to ‘hold their mind in mind’ – being curious about their experience, sensitive to their pain (especially when they face the challenges of neonatal care) and committed to our part in offering experiences of soothing, safeness and regulation. There are a range of approaches that can support this from practical methods such as kangaroo care, to methods that require more scaffolding, such as infant observation (eg the Newborn Behavioural Observations tool or psychoanalytic observation), parent education (eg Solihull Approach) or psychotherapeutic methods (eg ‘Watch, Wait, Wonder’). These approaches invite families and staff to slow down and consider the inner world of an infant. When this inner world might be confusing or painful, as it may be in neonatal care, this can be a source of threat for caregivers, which is where emotional containment and compassion at other levels of the system becomes so important to sustain our curiosity about infant experience.
Putting it all together
Compassionate care should not be considered an additional aspect of maternity and neonatal care, but rather a core value that underpins and threads through all aspects of that care. In this regard, compassion requires minimal additional time at the point of delivery. However, as we have outlined, in a system that faces so many threats, posing so many risks to the undermining and eroding of compassionate practice, a meaningful investment of time and resource is required to prepare the ground and scaffolding to continue to grow a culture in which all can thrive.
TABLE 3 provides examples of how compassion can be offered as an alternative to threat-based practices across all levels of the system. Based upon a psychological understanding of what compassion is and how it best functions, we recommend that this investment is targeted at the following domains:
- A sufficiently resourced system with the correct skill mix (across medical, nursing, psychological and allied health professionals) to ensure that there is adequate capacity to practise safely and without unreasonable cognitive and emotional load.
- Sustained training for staff in a framework to think about compassion, with resources to help embed this framework (Padlet4).
- Psychological professionals to facilitate safe spaces to reflect and learn, and to provide the interventions described in this article.
- Time and resourcing for frontline staff and leaders to attend such reflective spaces.
Perinatal services have repeatedly been tasked with learning from the past and increasing kindness, accountability, team working and communication. At the heart of all of these is a culture of courageous compassion, with the time, space and support to open up thinking and welcome difficult questions. There is good evidence for ‘what helps’ to underpin such a culture. There has never been a more critical time to invest in this change.
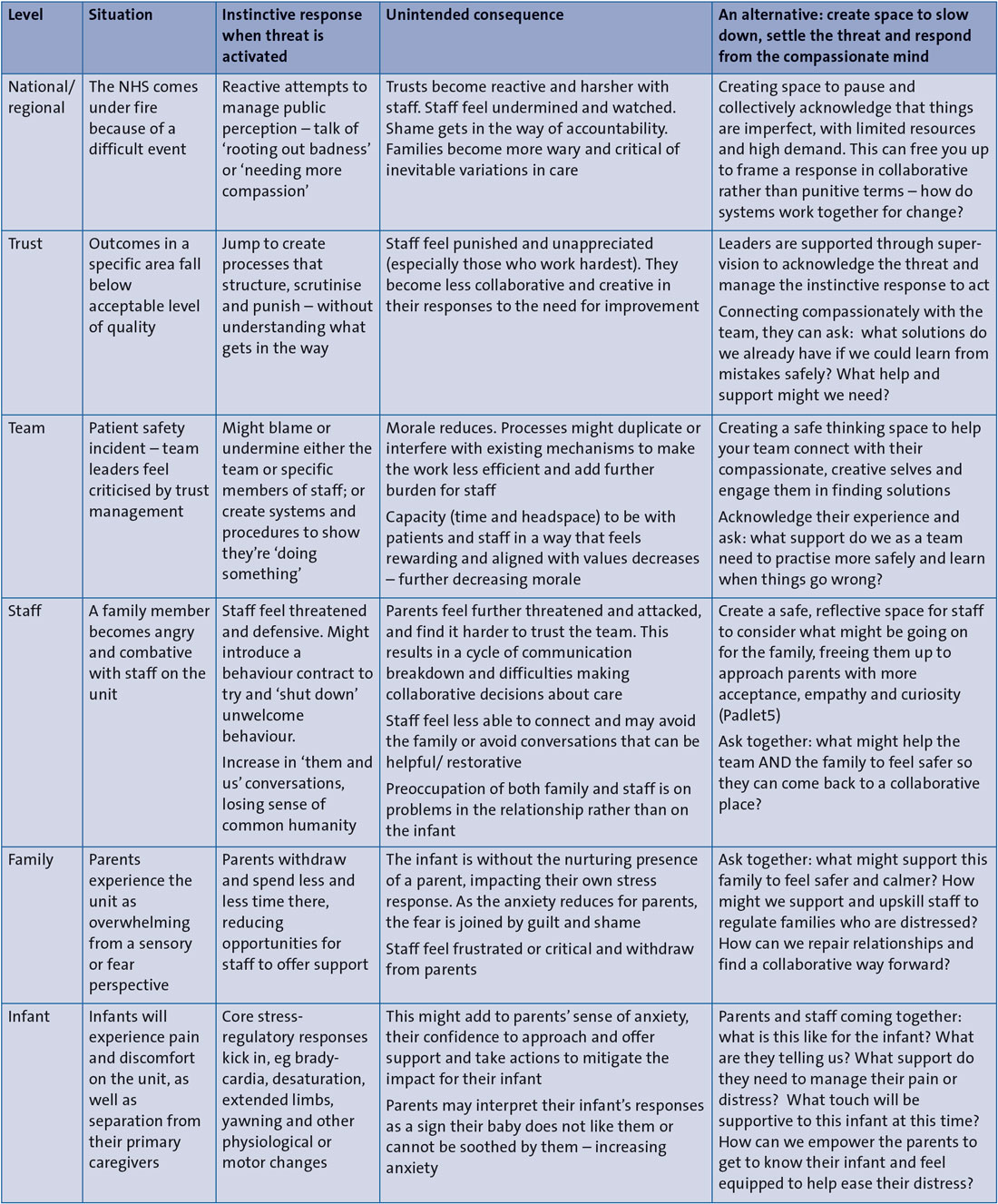
TABLE 3 Examples of how compassion can be offered as an alternative to threat-based practices across all levels of the system.
Acknowledgement
The authors appreciate comments and feedback on earlier drafts from Dr Victoria Selby. Some of the ideas discussed were developed during a British Association of Perinatal Medicine webinar on com-passionate culture in collaboration with Dr Katie Bohane and Dr Ria Evans Fry. Consent was given to use the quote from the staff member included in the article.
Or read this article in our
Tablet/iPad edition
- Compassionate practice needs to be built on a clear understanding of the science of compassion.
- Experiences of threat and soothing filter up and down through layers of the system through the presence or absence of emotional containment in connected relationships.
- Bringing about compassionate cultures in maternity and neonatal care involves action at all levels of the system.
Also published in Infant:
