

The anatomy of compassion: courage, connection and safeness in perinatal practice
The new NHS England Three Year Delivery Plan for Maternity and Neonatal Services advocates for compassionate care for families and compassionate, psychologically safe workplace cultures for staff. In this article we propose the need for a shared language and understanding of what compassion is, how it works, why it can feel hard and why practising compassion is an act of courage. We aim here to share our understanding of compassionate approaches from using them clinically in our work in maternity, perinatal and neonatal services. We also give some suggestions for growing compassion across the system, both for leaders and systems as well as individuals.
Davy Evans
davy.evans@nhs.net
Ruth Butterworth
ruth.butterworth@alderhey.nhs.uk
On behalf of the Neonatal Leads for Psychological Practice in England’s Neonatal Operational Delivery Networks (see TABLE 1)
Evans D., Butterworth R., Atkins E., Chilvers R., Marsh A., Barr K., Cole S., Cordwell J., D’Urso A., Higgins S. The anatomy of compassion: courage, connection and safeness in perinatal practice. Infant 2023; 19(3): 88-92.
TABLE 1 This report was produced by the Consultant Clinical Psychologists listed in their roles as Psychology Leads for the Neonatal Operational Delivery Networks across England.
The new Three Year Delivery Plan for Maternity and Neonatal Services1 sets out the priorities of NHS England for the delivery of safe, personalised and equitable maternity and neonatal care. We warmly welcome the intention of this document, which advocates for compassionate care for families and compassionate, psychologically safe workplace cultures for staff.
We witness compassion in the intentions and actions of our colleagues across the system and have seen clinically the transformative power that compassion can hold. We also often encounter misunderstandings about the nature of compassion, which is sometimes seen simply as ‘being nice’. The central place of compassion in the Delivery Plan warrants a discussion of the complexity of compassionate care. In the same way that one would not expect a medical professional to intubate a baby without a grasp of that baby’s anatomy, we believe that an understanding of the ‘anatomy of compassion’ will help systems to grow cultures of compassionate care. With this shared understanding of compassion established, we plan in a future article to share more practical ideas about how compassion can be lived in action.
What is compassion?
Gilbert (2013)2 defines compassion as: ‘A sensitivity to suffering of self and others, with a commitment to try to alleviate and prevent it’. The essence of compassion is in leaning into difficult conversations; having the capacity to approach discomfort, with the intention of helping. There have been some very difficult conversations about maternity and neonatal care in recent years, with high profile reviews highlighting the vital role that compassionate care plays in ensuring safe and quality services,3,4 a position that is not new.5 These reviews assert that cultures of blame and fear maintain a context of threat and defen-siveness, undermining compassion and perpetuating gaps in quality and safety.
While we can recognise blame as being unhelpful, a compassionate mind also brings understanding and empathy not only to the initial concern but also to a blaming response. When working in a high-stakes, high-threat system, people instinctively seek safety through primitive processing such as blame and ‘othering’. For this reason, it can be challenging for a system to address cultures of blame without:
- further resorting to the rhetoric of blame
- placing responsibility in the hands of individual frontline staff to ‘be kinder’ to both patients and themselves.
A compassionate mind acknowledges the challenges of both providing and receiving care in a system that evokes these responses, and searches for ways to connect patients and staff in their shared humanity. Bringing a compassionate lens to systemic failures provides the context for more effective accountability and learning rather than blame and scapegoating.
The case for compassion
The giving and receiving of compassion and the practice of self-compassion, organises the mind and body into a state of safeness in which we:
- have the courage to face and engage with very difficult situations
- think more creatively, having the courage to explore new ways of working from a secure base of safeness
- learn most effectively when something goes wrong
- more effectively take the perspective of others, allowing for sincerity and authenticity in our interactions with families (as advocated for in the Patient Safety Incident Response Framework process6)
- can best birth, heal after birth, and breastfeed.
The indisputable evidence for compassionate care being linked with safer and better-quality outcomes is clearly articulated by Michael West (2021).7 West also makes an additional convincing financial argument that compassionate care, by improving patient safety, would go some way to reducing the £2.5bn of litigation claims against the NHS, 62% of the total of which is related to obstetric care. Compassionate care is important in all healthcare settings, but especially so in maternity and neonatal care, where both the stakes and threats are so inherently high.
A model to understand compassion
The understanding of compassion as engagement with suffering with the intention to alleviate and prevent it, is an ideal that is at the heart of NHS care. The compassionate mind approach offers a way of making sense of this ideal in its full complexity and also a road map to promoting and nurturing it. Gilbert (2013)2 describes how the human mind is primed to be motivated towards compassion. He also emphasises that compassion can feel overwhelmingly difficult to connect with in situations of high threat. Such threat is ever-present in maternity and neonatal systems.
The compassionate mind approach begins with an evolutionary perspective. Over time humans have developed minds that are capable of great innovation and flexibility, but that are also still driven by the same basic drives as all species. The model proposes that our activity is governed by three motivational systems (FIGURE 1):
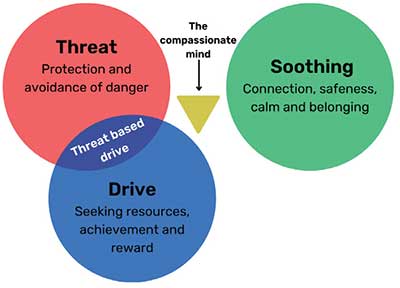
FIGURE 1 The three systems of motivation.
- The threat system
- The drive system
- The safeness and soothing system
- An activating system motivated by protection and safety seeking – the fight/flight/freeze system
-This system is associated with feelings such as anger, anxiety, disgust and shame.
– An activating, incentive/resource-seeking system that is motivated by achievement, pursuing, consuming and acquiring
– This system is associated with a sense of being driven, excited, purposeful and feeling pleasure, reward and vitality.
–A contented state where we feel meaningfully connected with others, within which safeness and kindness are engaged and the body and mind can come to settle
–This system is characterised by a sense of connection, safeness, calm.
These three systems interact in important ways. When we are soothed by a safe connection with a trusted other, our threat system can be regulated and calmed. This can be seen when a parent offers gentle containment holding on to an infant in an incubator to soothe and settle them, or when a frightened parent feels able to slow their breath in the presence of a member of staff who listens and hears their distress. In this way, the safeness and soothing system can act like a brake on the threat system.
Sometimes our drive to achieve can be motivated by efforts to escape threat, as opposed to efforts to pursue meaningful and valued goals. Faced with real or perceived threat of criticism, loss of status or reputation, we can feel a need to constantly achieve to avoid this threat. This is often called threat-based drive and can be an unsustainable strategy with diminishing returns.
No one system is better or more important – each is fundamental to our surviving and thriving as individuals and as a species. However, maintaining a balance in these systems is key to optimal functioning both at an individual and systems level, and fundamental to the delivery of safe, compassionate care.
Threat in NHS maternity and neonatal systems
While the arrival of a new baby can be a time of joy and connection for infants, families and staff alike, it can also be a time of great threat and uncertainty. Having a baby is an inherently risky and vulnerable process. Although many families have chosen to have babies, the maternity system might be the first time in adulthood that they have been dependent on others for their wellbeing and survival. Certainly, no parent would choose to have a birth experience that carries additional risk or be in a situation where their baby requires neonatal care. When pregnancy complications arise, birth trauma occurs or when an infant is born prematurely or unwell, uncertainty and threat are ever-present for families (FIGURE 2). Many parents experience a secondary source of threat from their own internal self-critic, which can lead to feelings of guilt and shame. Such experiences are amplified by a wider context that is also threat-saturated: financial austerity, a cost-of-living crisis and a time in history where our sense of connection and community is increasingly fragmented.
Although increased survival has offered so much hope to families, hospital admission provides an experience of substantial threat for infants. Exposure to pain, isolation and sensory overload are experiences of threat in neonatal care that infants cannot control, at a time when their primary source of soothing and safeness – their parent – is not always readily accessible.
For staff, threat can be pervasive, with a staffing crisis often leaving teams feeling stretched to breaking point. This can result in a ‘gap between the noble ideals of their profession and the realities of its business’,8 leading to distress when professional values are thwarted. Increasingly healthcare systems are responding to threat by demanding improved performance of teams who are monitored and scrutinised through targets. This threat-based activation of the drive system – avoidance of criticism or being penalised becoming the primary motivation to achieve – itself becomes an additional source of threat for the reason that success is elusive, or the effort exhausting, or because the meaning and therefore the satisfaction is lost (FIGURE 2). Such experiences of threat for staff have been amplified in recent years through the physical and psychological aftermath of COVID and in a wider culture that is suspicious of and often hostile towards public sector workers. Experiences of threat and threat-based drive likely account for much of the increased risk of trauma and mental health difficulties in parents of preterm infants, and of burnout and trauma in staff.9
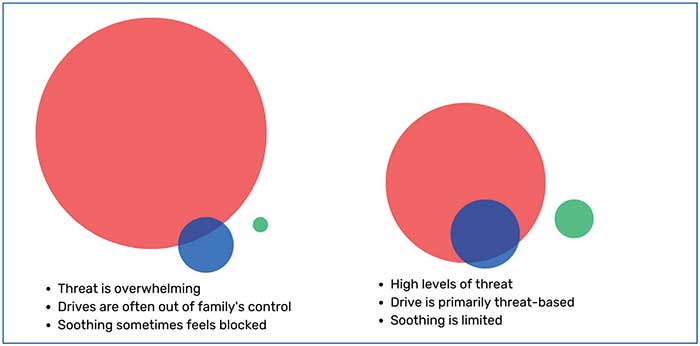
FIGURE 2 An illustration of a common balance of motivations for families in neonatal care (left) and staff in maternity and neonatal services (right). Red = threat; blue = drive; green = soothing.
What is the impact?
The combination of physical and psychological risk and competition for physical and human resources converge to leave both staff and families within maternity and neonatal systems spending large periods of time with a highly activated threat system.
In our ‘threat mind’ we function at a more primal level focused on survival and begin to process our environment accordingly. We:
- become preoccupied with competition and hierarchy – the need to be better than, to avoid being worse than (and therefore vulnerable), which sets us up for a focus on blame
- become hyperalert to risk and danger, narrowing our field of vision, making it harder to work collaboratively, think creatively or respond in an agile way to our circumstances
- are primed to avoid perceived threats rather than move towards them, making it harder to engage effectively with risk or challenge
- are more cut off from our safeness and soothing system, which is key to promoting connection with those around us
- revert back to old, habitual ways of thinking, acting and relating rather than being able to extend and develop our practice and take in new learning or information.
When our threat system is intensely activated over a prolonged period, our brains and bodies adapt, from cortisol responses and epigenetic gene expression to immune-inflammatory processes and the gut-brain axis.10 We become sensitised and develop a lowered threshold for shifting into this threat mindset. This especially occurs when our attempts to control or regulate our threat system have been unsuccessful.
A compassionate mind
Our capacity for compassion sits within and between the three motivational systems (FIGURE 1). The wisdom of our compassionate mind supports our safeness and soothing system to calm our threat system, allowing us the courage to turn towards difficulty rather than away from it. Our compassionate mind can also help us be open and curious about our motivations and drives: whether our actions are driven by our values or by threat-based attempts to avoid rejection or criticism.
As humans, we will encounter ongoing fears, blocks and resistances to compassion. This is how we are built; it is not our fault. Some blocks to compassion might include:
- fear of being seen as weak or a sense of disgust at our own or others’ vulnerability
- belief that to slow down, however briefly, will result in catastrophic risk or failure
- belief that compassion excuses problematic behaviour or allows it to go unchallenged.
If we can meet these experiences them-selves with compassion, we are freed up to work through the resistance and continue to act from a compassionate position.
Growing a compassionate mind for individuals
Gilbert (2017)11 has attempted to operationalise some of the work required for compassion to flourish by identifying a series of attributes and skills that we can cultivate within ourselves and the systems in which we operate. To effectively respond to suffering with compassion, an individual must have access to six engagement attributes:
- Care for wellbeing (a motivation and willingness to respond to suffering)
- Sensitivity (an ability to identify suffering)
- Sympathy (the capacity to feel connected to the suffering of self or others)
- Distress tolerance (the ability to move towards rather than away from the emotions evoked by suffering)
- Empathy (the ability to stand apart from and make sense of suffering)
- Non-judgement (the commitment and ability to take an accepting, non-condemning approach).
In addition to these attributes, individuals must also have the skills and wisdom to take action towards alleviating suffering in self and others (TABLE 2).
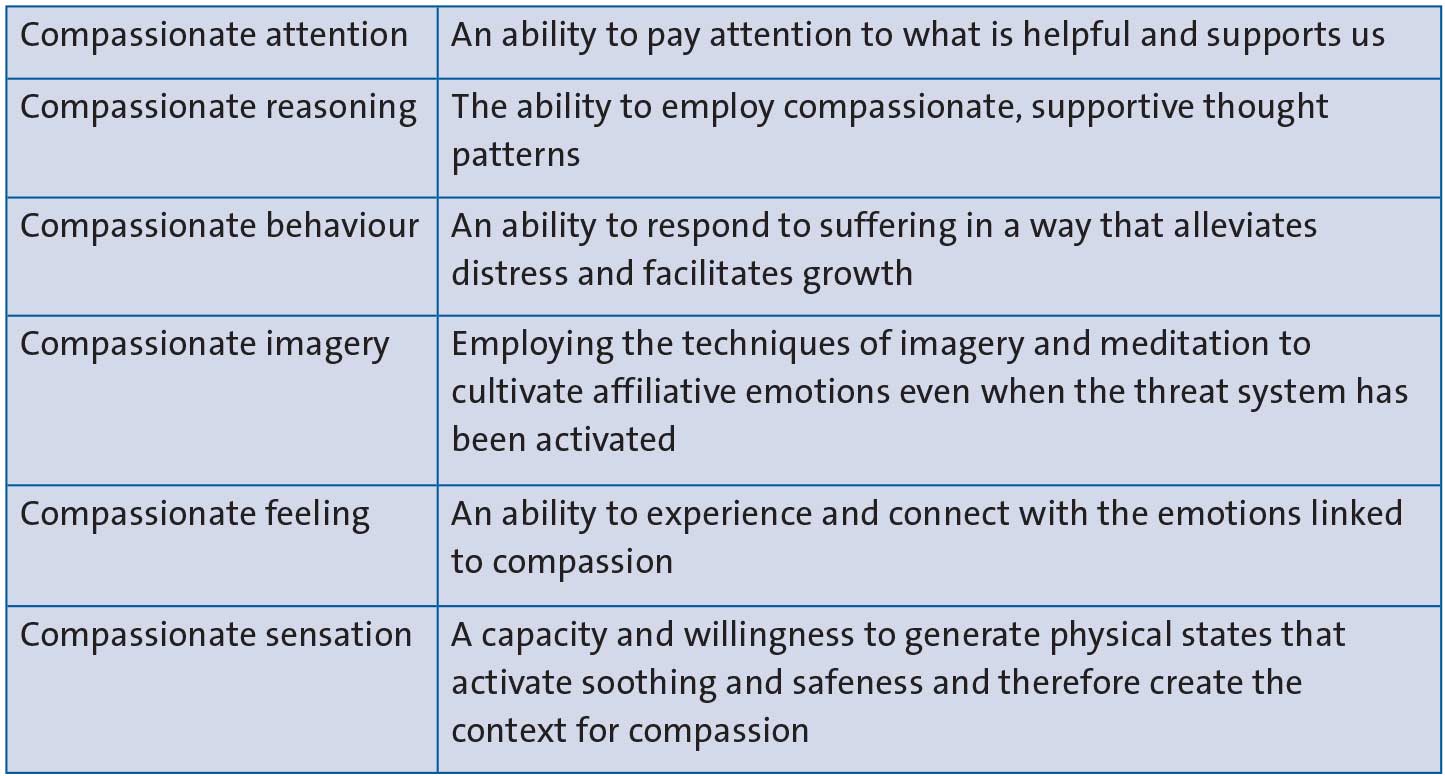
TABLE 2 Some of the skills and wisdom required to take action towards alleviating suffering in self and others.
The compassionate mind approach offers a series of practices and activities that can help to facilitate the development of these skills and attributes through individual and collective practices, as well as exercises that support maternity and neonatal settings to engender soothing and safeness. These might include individual practices to connect with safeness in difficult moments, mechanisms for introducing soothing and safeness to a debrief or practices such as a ‘compassionate walkabout’ or collective ‘compassionate kitbag’ where staff are encouraged to work together to modify threat and increase psychological safeness within the workplace.
There are many opportunities for training in the principles and practices of the compassionate mind approach or compassion focused staff support and a growing evidence base for the power of this intervention.12 This approach is not, however, a quick fix and relies on ongoing growth and practice at a system as well as individual level – creating compassionate spaces to think, where staff can come together with colleagues in conditions of safeness, reflect on their own experiences of threat and soothing, and engage in an ongoing commitment to developing a collective wisdom and compassionate mind.
In a future publication we aim to build on the anatomy of compassion discussed here with a more practical guide for the practice of compassion.
Growing a compassionate mind for the system
NHS rhetoric frequently describes the institution as indistinguishable from its people. Within the maternity and neonatal systems this incorporates more than 40,000 highly skilled, trained and caring staff who are motivated to deliver compassionate, high quality and safe care. Their compassionate initiatives can be knocked off course by busyness, experiences of threat and exhaustion. Staff frequently describe the system around them as impeding their ability to deliver the safe, compassionate care that they are driven to provide. If the system responds with compassion, this course can be righted. However, as discussed previously, attempts to steer the course through demanding improvement, or seeking to blame are likely to backfire and disconnect staff even further from their intentions. The role of managers and leaders is to consider what has thwarted staff in their efforts to deliver compassionate care and to ask: ‘How can I help?’
Within the NHS England Delivery Plan, a positive culture and compassionate culture are referred to interchangeably, although they are quite different. While positivity and compassion are often compementary, they are different mentalities and rely on different neural systems.13
Positive cultures, involving learning from excellence and focusing on success, have been advocated for some time and demonstrate effectiveness in driving improvements in quality and safety.14 This approach of striving for what works well (which involves engagement of the drive system) has been termed ‘Safety II’ as a response to a more traditional healthcare safety culture focused primarily on avoidance of harm that is rooted in the threat system.
Compassionate cultures are rooted in connection, safeness and values-based motivation. For this reason, we might consider this as ‘Safety III’ or, preferably, ‘safeness’. There is a crucial distinction here between safety (which is about the absence, avoidance or prevention of threat) and safeness (which is the presence or flourishing of contentment, care and connection). As we move towards widespread implementation of the Patient Safety Incident Response Framework,6 this is an important time to consider both safety and safeness and to embed the culture and support necessary for engendering both.
Leading with compassion
In maternity and neonatal services in the UK, caregiving is coordinated across large multidisciplinary teams. One of the benefits of this team approach is the diverse range of perspectives and positions that can shape a family’s care. This comes at a cost; resources and time are finite, potentially resulting in activation of the threat system and associated competition for resources, time and power. Even when intra-team collaboration is effective, relationships with other teams within the perinatal pathway can sometimes feel complex and challenging.
For a team to navigate this and collaborate effectively, retaining a focus on the quality of care (rather than resorting to sometimes arbitrary metrics in an attempt to escape threat), requires those leading change to have the capacity to switch from their own threat system to the courage of their compassionate mind. In doing so, they free themselves up to prioritise relationships and communication, asking: ‘How can I help?’ In turn, this provides staff with a containing safe haven to return to, allowing them to switch patterns and connect with their own compassionate mind even in the context of significant challenge – and a secure base that enables them to take responsibility for their own needs and to go back out into a challenging environment and thrive. It is vital that we see the compassionate mind not as a strength or weakness of individuals, but as a necessary characteristic of the system of governance itself.
For this reason, we welcome the Delivery Plan’s commitment to supporting senior leaders through the perinatal culture and leadership programme. This is a helpful place to start, and will be most effective in bringing about cultural change when a deeper understanding of the importance and complexity of compassionate care is embedded across the whole system. We work with colleagues who lead with great compassion, and we know that their efforts have the greatest impact when the systems they lead are well resourced and adequately funded.
Conclusion
This formulation of compassion is far from a fluffy or nebulous concept. Neither is it a ‘given’ or something that is always easy to give or to receive. The compassionate mind is a way of being and responding to our experience as humans and as professionals that requires ongoing cultivation and courage. In a future article, we aim to share some practical steps that foster compassion for individuals and teams. However, it is the responsibility of the wider system to create circumstances in which compassion can flourish in perinatal practice. This will require a courageous commitment to, and above all investment in, a context of safeness in maternity and neonatal services.
Acknowledgement
The authors appreciate comments and feedback on earlier drafts from Michelle Cree, Consultant Clinical Psychologist.
Or read this article in our
Tablet/iPad edition
- Compassionate care and compassionate cultures are advocated for in recent key documents.
- A full understanding of the nature of compassion is essential for bringing about compassionate culture in maternity and neonatal care.
- Opening a discourse of ‘safeness’ in relationships as well as ‘safety’ in care will be key in achieving the ambitions of NHS England’s Three Year Delivery Plan.
Also published in Infant:
