

Patent ductus arteriosus: are we treating the right ones?
Variability in the diagnosis of haemodynamically significant patent ductus arteriosus (hsPDA) can result in treating inconsequential PDAs and causes difficulty in interpreting clinical outcomes from the available literature. This study evaluates the echocardiogram parameters used to ascertain hsPDA in very low birth weight infants in a tertiary care centre in the UK. Extremely premature infants that received pharmacological or surgical treatment for a PDA were evaluated for basic characteristics, diagnostic echocardiograms, closure rates and eventual outcomes of persistent duct on follow-up.
Daniel Hickman
Foundation Year Doctor1
Anupam Gupta
Consultant Neonatal Medicine2 and Honorary Senior Lecturer3
Arin Mukherjee
Consultant Neonatal Medicine2 and Honorary Senior Lecturer3
arin.mukherjee@mft.nhs.uk
1Wrightington, Wigan and Leigh Teaching Hospitals NHS Foundation Trust
2Department of Neonatology, St Mary’s Hospital, Manchester University NHS Foundation Trust
3University of Manchester
Hickman D., Gupta A., Mukherjee A. Patent ductus arteriosus: are we treating the right ones? Infant 2023; 19(6): 198-202.
A haemodynamically significant patent ductus arteriosus (hsPDA) contributes significantly to mortality and morbidity in infants born earlier than 28 weeks’ gestation.1 Not only is the incidence of PDA inversely proportional to gestational age, but the spontaneous closure of PDA during early postnatal life is also affected by the level of prematurity. 80% of premature infants born between 25-28 weeks’ gestation and 90% of those born at 24 weeks’ gestation have a clinically demonstrable PDA after four days following birth.1-4
A PDA serves as a conduit between the systemic circulation, which has higher blood pressure, and the pulmonary circulation, which has lower blood pressure. This causes the blood to flow across the PDA (often called a PDA shunt) from left to right, i.e. from the aorta to the pulmonary artery. The effects of PDA are only obvious after the first few days of life because of the high pulmonary vascular resistance at birth. The blood flow in the aorta (systemic circulation) is stolen away by the PDA, because of the physiological reduction in the pulmonary vascular resistance over the first several days. This phenomenon, known as ductal steal, happens as a result of the pressure gradient between the pulmonary and systemic circulation. This ductal shunt results in pulmonary over-circulation and consequent systemic hypoperfusion due to the blood diverting away from the aorta.4-6 A persistent PDA that steals a significant amount of blood from the systemic circulation is often called a haemodynamically significant PDA (hsPDA).
This simplistic explanation appears to allude to the concept that PDA is always harmful and that it should be closed either by medical treatment or surgical treatment. To substantiate this, a host of morbidities such as pulmonary haemorrhage, bronchopulmonary dysplasia, necrotising enterocolitis, renal failure, cerebral haemorrhage and periventricular leukomalacia have all been ascribed to a hsPDA.4-6 However, while PDA remains a plausible trigger for all these complications, numerous observational studies and randomised controlled trials (RCTs) spanning several decades have failed to demonstrate a cause-and-effect relationship between PDA and its supposed morbidities.7-9 In such a conundrum, the simple question that comes to mind is whether we are treating the right duct. This becomes a particularly relevant question for the trials that have compared a pharmacological treatment with a placebo (ie no treatment) and have gone on to measure the clinical outcome. The concept of haemodynamic significance is a matter of much contention. While it tries to differentiate a consequential duct from an inconsequential one, a unanimous definition remains elusive.10,11 TABLE 1 highlights the variability in the inclusion criteria and the echocardiogram parameters of all RCTs included in the systematic review by Katsaras et al (2022).9 The table presented here is a modified simplistic version adapted from the original.
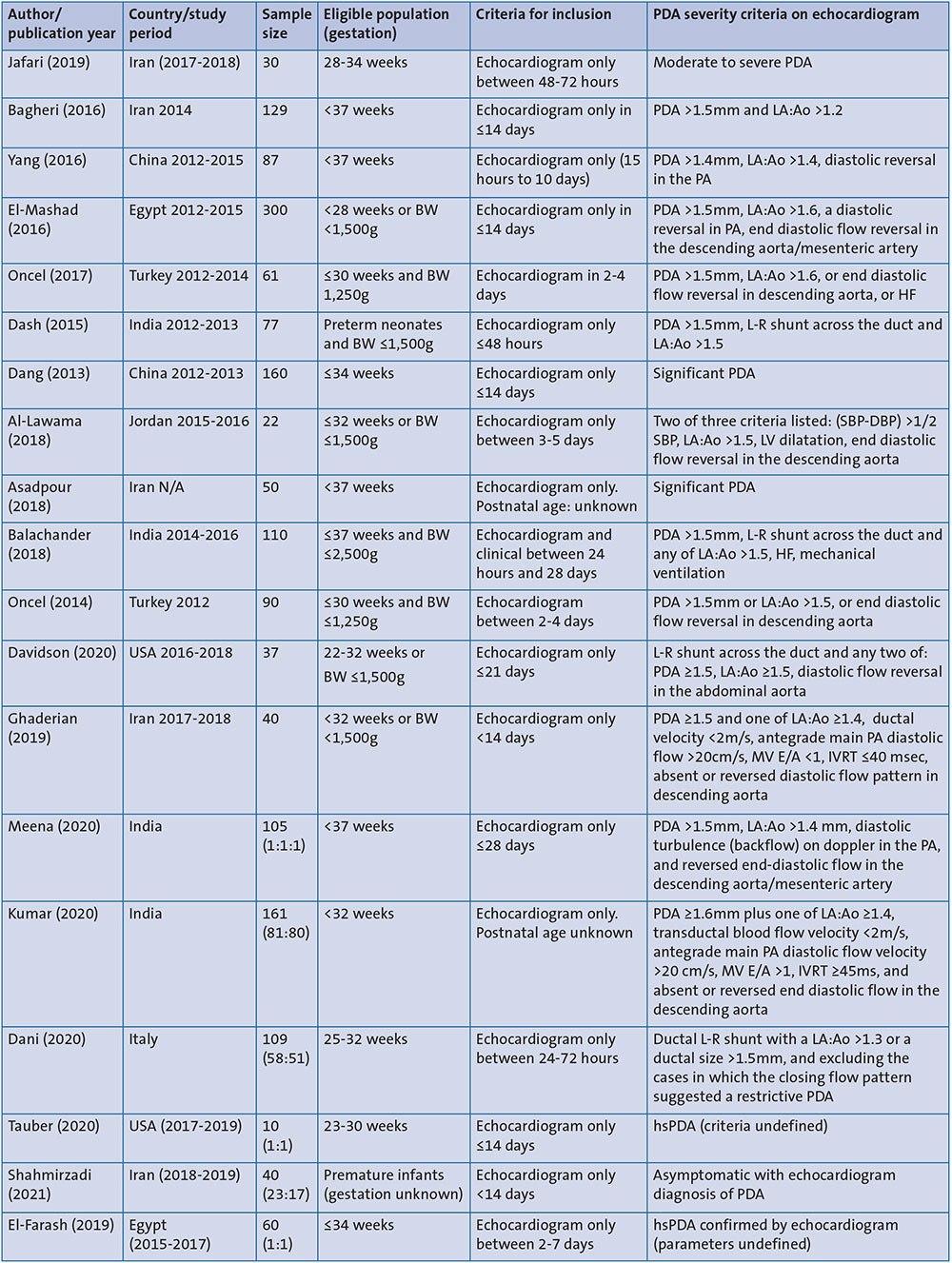
TABLE 1 A summary of the variability in the diagnosis of hsPDA in RCTs (extrapolated from the systematic review of Katsaras et al, 20229). Key: BW=birth weight; LA:Ao=left atrium and aortic diameter ratio; HF=heart failure; L-R shunt=left to right shunt; PA=pulmonary artery; LV=Left ventricular; MV E/A=mitral valve inflow E/A ratio; IVRT=isovolumic relaxation time; SBP=systolic blood pressure; DBP=diastolic blood pressure.
Methods and data collection
The primary objective of this study was to evaluate which PDAs are generally treated and how this selection of infants can affect the outcome.
Echocardiogram parameters to evaluate the haemodynamic significance of a PDA were revisited to ascertain the reasoning when deciding to actively treat or monitor PDA. A single-centre retrospective observational study was performed over a six-year period from 1 April 2015 to 31 March 2021 at a tertiary neonatal centre in the UK. Extremely low birth weight infants born under 28 weeks’ gestation were selected. The national standardised neonatal database (BadgerNet), a critical care information system (ICCA) and a web-based electronic patient record system (Chameleon EPR) were used for data collection. The search returned a total of 744 preterm admissions (gestation ranging between 22 weeks to 27+6 weeks) to our neonatal unit in the specified time period. 399 infants were identified as inborn and 345 as outborn (FIGURE 1).
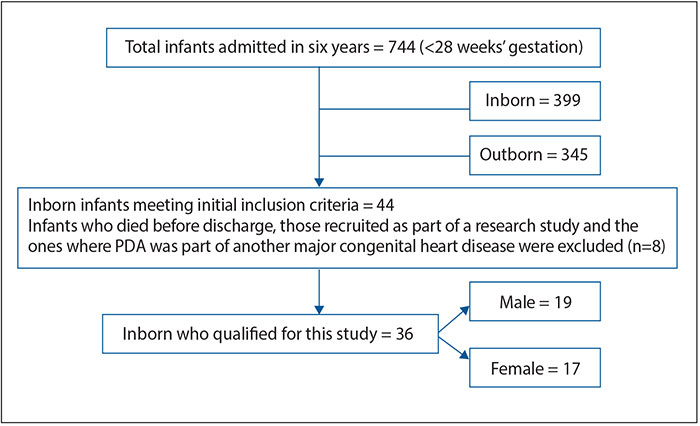
FIGURE 1 Patient selection.
Inborn infants were defined as babies that were born in our hospital and admitted to our neonatal unit. Outborn infants were defined as babies that were born or received treatment in other hospitals prior to their transfer to our neonatal centre for specialist care. Outborn infants were excluded from the study.
Out of the 399 inborn infants, 44 infants met the initial inclusion criteria (ie diagnosed as having a hsPDA and received treatment to close their PDA, during their stay in our unit). A further eight infants were excluded as either they died or were part of a research trial or the PDA was part of another major congenital heart lesion. 36 infants fulfilled the criteria for evaluation in our study.
Our departmental practice guideline did not have any defined echocardiogram criteria for diagnosing hsPDA at the time of this service evaluation. If PDA was suspected in preterm infants due to an audible heart murmur, an echocardiogram was performed by either a neonatologist with expertise in paediatric cardiology (PECSIG) or a cardiologist. The decision to treat would lie on the neonatal clinician looking after the baby based on the information provided and is largely influenced by the echocardiogram findings in addition to the respiratory and clinical status of the infant. The pharmacological agents used to treat a hsPDA were intravenous administration of ibuprofen or intravenous paracetamol.
The case records of these 36 infants were evaluated for infant demographics, the initial diagnostic echocardiogram reports, as well as the last echocardiogram report on record prior to discharge to assess the status of the PDA. If the infant was noted to have a PDA at discharge, electronic patient records were used to find the status of follow-up and eventual outcome in the cardiology outpatient clinics.
All relevant information was recorded on an Excel spreadsheet, infants were allocated a study number and identifiable information was only stored on a hospital password-protected computer or an encrypted USB. For data analysis, the Excel spreadsheet was anonymised.
Results
Thirty-six patients that met the inclusion criteria were treated for hsPDA. There were 17 female and 19 male infants. The average gestational age was 173 days (24+4 weeks). The average birthweight of the patients was 753g. All echocardiogram reports were evaluated including the first one used for the diagnosis of hsPDA. The respiratory status of each individual infant was also recorded.
58% (21/36) of the echocardiogram reports that were used to diagnose the hsPDA described the PDA using only verbal descriptors of size (eg small, moderate or large PDA). Only 33% (12/36) of the reports included the actual diameter of the PDA (in mm). 8% (3/36) had no recorded/accessible echocardiogram reports (FIGURE 2). 53% (19/36) of the reports included a description of the shunt flow pattern (eg closing flow pattern or opening flow pattern), and only 17% (6/36) of the total reports included any values of the shunt velocity (eg PDA systolic velocity and PDA diastolic velocity). 25% (9/36) of the reports included values for the left atrium and aortic diameter ratio (LA:Ao) (FIGURE 2).
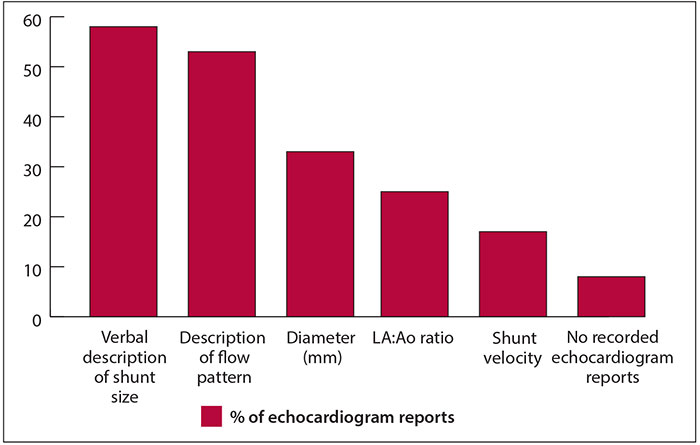
FIGURE 2 Variability in echocardiograms used for a diagnosis of hsPDA.
In terms of respiratory status, 92% (33/36) of patients were mechanically ventilated via an endotracheal tube, 3% (1/36) were on high flow nasal cannulae and 5% (2/36) were nursed in ambient oxygen in the incubator and both were noted to have increased oxygen requirements.
Treatment and outcomes
86% (31/36) of babies received ibuprofen as the first course of management. 3% (1/36) and 11% (4/36) of babies had paracetamol and ligation/catheter closure, respectively, instead. All of the babies who received paracetamol or underwent ligation/catheter closure were found to have successful closure. Out of 31 babies who received ibuprofen, 18 had successful reduction to non-hsPDA or demonstrated closure with a single dose of ibuprofen; a success rate of 58%. Out of the failed 13 courses, 12 received a second course of ibuprofen and one received paracetamol. The second course of ibuprofen had a success rate of 83% (10/12) with two infants receiving surgical ligation for failed treatment.
We reviewed the incidence of successful closure before discharge home. Pre-discharge scans demonstrated that out of 36 babies, all infants who had ligation or catheter closure (6/6) remained closed. Of the remaining 30 infants, 10 (33%) had full closure before discharge. Closure rate for infants by treatment regime is illustrated in FIGURE 3.
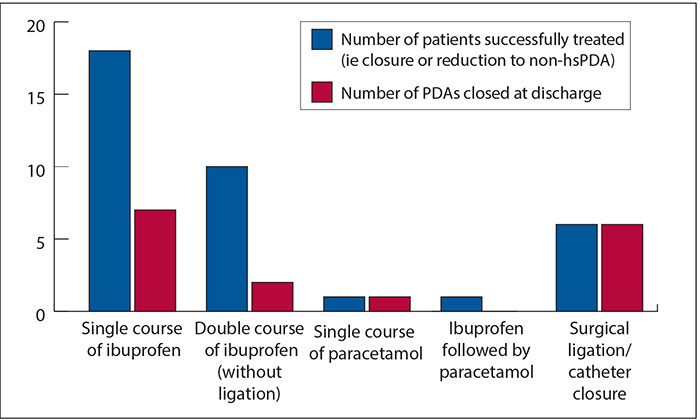
FIGURE 3 Number of PDAs closed at discharge by treatment modality.
Follow-up data were available for 19 out of 20 infants with an open duct noted on a pre-discharge echocardiogram. In the majority of infants (11/19; 58%) the duct had closed by the first outpatient follow-up. The PDA was noted as closed in 95% (18/19) of infants with the approximate mean duration of closure noted at 11.7 months of life (range=3.5-47.8 months). One infant continues to have an open duct and remains under follow-up with the cardiologists.
In summary, 36 infants received medical or surgical treatment for hsPDA. However, the recorded echocardiogram reports incorporated a range of verbal descriptors/jargons and inconsistent parameters that were not fit for purpose. 58% of reports used only verbal descriptors of size. Reviewing the management and treatment outcomes, 83% (30/36) of infants were treated by pharmacotherapy alone (i.e. without ligation or medical device closure) with either ibuprofen or paracetamol. Surgical ligation and transcatheter occlusion were noted to be 100% successful. The pre-discharge closure rates for medically managed infants (pharmaco-therapy) were noted to be 33%. Of the infants who had a persistent PDA at discharge, follow-up data revealed that 95% closed spontaneously. One infant required surgical ligation for a persistent duct and another one remains under follow-up.
Discussion
The review demonstrated that the criteria for diagnosis of hsPDA remain inconsistent. There is a lack of a uniformity in determining the haemodynamic significance of a PDA. The criteria used varies widely between infants, showing that the problem of heterogeneity is deep-rooted and that variation likely comes from differing opinions of doctors and the parameters they use to diagnose hsPDA. This absence of a consensus is illustrated in FIGURE 2. There is urgent need for an evidence base to support clinicians in diagnosing hsPDA.
We found that the overall closure rate of PDA in infants who received medical management by either paracetamol or ibuprofen was 33%. Also, the majority of infants who underwent pharmacological therapy had a resolved PDA by their first outpatient follow-up, ie within three months of discharge.
The optimum management of PDA in preterm infants remains one of the most debated topics within the field of neonatology. In such a conundrum, accurate identification of the infants at greatest risk of long-term morbidities from PDA exposure remains crucial. While an echocardiogram remains the gold standard to ascertain the significance of a PDA and its impact on an infant, the features of pulmonary over-circulation, systemic hypoperfusion and cardiac dysfunction, need to be comprehensively analysed. Failing this, treatment may be inadvertently offered to those PDAs that were destined to close spontaneously anyhow and so may not only be futile but can result in untoward side effects from unnecessary pharmacological treatment.
There are a number of RCTs and systematic reviews that have compared the efficacy of pharmacological treatment for hsPDA.7-9 However, these systematic reviews, composed of multiple RCTs, pool their results to draw a conclusion. One of the limitations of these reviews is the heterogeneity in the definition of hsPDA used in the collated studies, which reduces the reliability of the pooled results as they cannot be compared to one another.7-9 TABLE 1 from the review by Katsaras et al,9 shows the variation in diagnosing hsPDA in individual trials that compare the efficacy of various pharmacological agents. The authors of the review acknowledge that the differing diagnostic criteria may influence the reliability of the pooled results and therefore the quality of the conclusions.9
Limitations of the study
The limitations of our data are acknowledged, particularly the drawbacks of a retrospective observational study. Missing and incomplete data, while uncommon, present an issue, particularly when combined with the relatively small sample size. This may have affected the analysis of the diagnostic criteria, particularly because the original echocardiogram reports were not always available, so the resources used may have been summaries leading to the appearance of a lack of detail. By the definition of a retrospective study, only details deemed necessary were recorded so areas of potential importance, such as the timing of treatment after birth or doses used in treatment, have been omitted from the results, which may account for the low closure rates by discharge seen when compared with other reports.
Future directions and conclusions
It would be naive to assume that PDA is a simplistic entity whose haemodynamic impact is solely assessed either by clinical status or by echocardiogram alone. The ductal diameter on its own for assessing PDA significance by echocardiogram is often non-contributory. No one size of the duct fits all preterm infants. A strategy involving multi-organ assessment of the ductal impact should form part of the routine assessment for diagnosis of hsPDA, including:
- Clinical markers of pulmonary over- circulation (eg respiratory support and ventilator dependency).
- Clinical markers of systemic hypoperfusion (eg hypotension, urine output, renal profile).
- Gestational age.
- A comprehensive echocardiogram evaluation (eg echocardiographic indices of pulmonary over-circulation and systemic hypoperfusion and an appraisal of myocardial performance).
This should be undertaken prior to deciding on treating a duct with a pharmacological agent. Each baby should be treated as an individual and a uniform strategy should underpin which infants should be targeted for treatment. Variability in the diagnosis of hsPDA is a widespread issue that can result in treating inconsequential PDAs with pharmacological agents that have their own side effects. It also causes difficulty when comparing studies on treatment and applying them to improve clinical practice. An international consensus on hsPDA is required to create uniformity of practice and allow better application in future trials to improve clinical practice.
Or read this article in our
Tablet/iPad edition
- Variability in the diagnosis of hsPDA is a widespread issue that may result in treating inconsequential PDAs with pharmacological agents.
- Thirty-six patients were identified for evaluation. The detail on their diagnostic echocardiogram reports varied widely.
- A consensus on hsPDA is required to establish uniformity in practice and allow future trials to improve clinical practice.
Also published in Infant:
