

The PAIR trial: is paracetamol the way forward in management of hsPDA?
Currently, intravenous (IV) ibuprofen is the only licensed medication for the medical treatment of patent ductus arteriosus (PDA) in the UK; however, there is emerging evidence to suggest that paracetamol may be a promising alternative with fewer side effects. The PAIR pilot trial is the first study in the UK to investigate the efficacy and safety of IV paracetamol in comparison to IV ibuprofen for the management of haemodynamically significant PDA (hsPDA) in preterm infants. This article describes the rationale for the use of paracetamol and the design of the PAIR pilot trial, which will help to inform a much larger future study.
Arin Mukherjee
Consultant Neonatologist1 and Honorary Senior Lecturer2
Ruth Gottstein
Consultant Neonatologist1 and Honorary Lecturer3
Consultant Neonatologist1 and Honorary Senior Lecturer2
anupam.gupta@mft.nhs.uk
1Department of Neonatology, St Mary’s Hospital, Manchester University NHS Foundation Trust
2University of Manchester
3School of Health and Society, Salford University
Background
An IV preparation of ibuprofen is the only licensed medication for the treatment of PDA in the UK; hence, its use as a first line medication to treat hsPDA in preterm babies. It is preferred over other medications, especially indomethacin, because of lesser adverse effects on the gut and kidneys. However, it does come with its own set of side effects.
There is some evidence that while paracetamol confers comparable treatment efficacy to ibuprofen for PDA closure, it has a lower risk of adverse events, particularly relating to acute kidney injury, reduction in gastrointestinal perfusion (risk of necrotising enterocolitis, NEC, or perforation) and/or bleeding. The PAIR trial (Paracetamol And Ibuprofen Research) is the first study in the UK to examine the efficacy and safety of paracetamol in comparison to ibuprofen for treating hsPDA in preterm infants (TABLE 1).
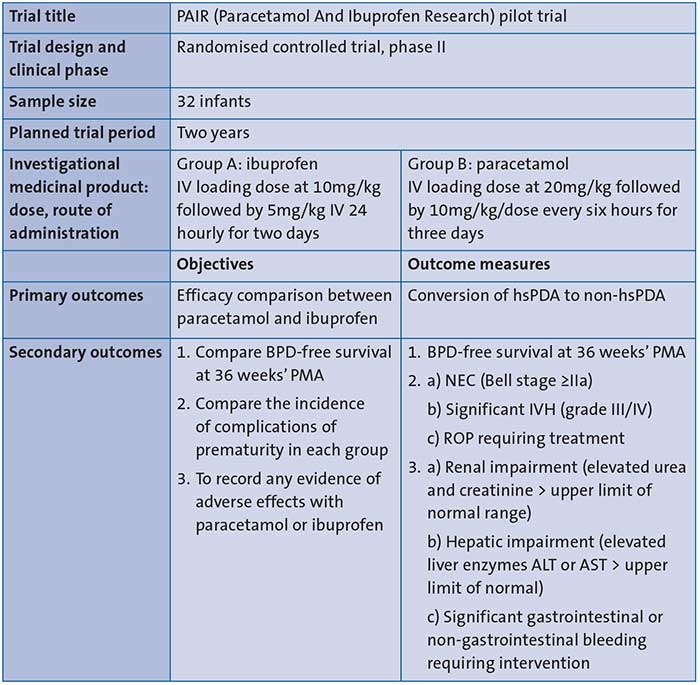
TABLE 1 The PAIR trial summary. Key: PDA=patent ductus arteriosus; hsPDA=haemo-dynamically significant PDA; PMA=post menstrual age; BPD=bronchopulmonary dysplasia; NEC=necrotising enterocolitis; IVH=intraventricular haemorrhage; ROP=retinopathy of prematurity; ALT=alanine aminotransferase; AST=aspartate transaminase.
The study objectives
The primary objective of the PAIR trial is to investigate the efficacy of IV paracetamol in treating hsPDA in comparison to IV ibuprofen in preterm infants born at <32 weeks’ gestation OR <1,500g birth weight. Infants are treated only if they are ≤28 days of age.
The study design
The trial is currently set up as a single-centre prospective randomised pilot study conducted at St Mary’s Hospital, Manchester. All infants who are clinically symptomatic (requiring any form of respiratory support) and suspected to have a PDA will have an echocardiogram to confirm presence of a hsPDA (defined in TABLE 2). The decision to treat infants with hsPDA will lie with the clinician. If infants are found eligible (TABLE 3) and a decision to treat the hsPDA is made, the parents will be approached. The study will be introduced with a parent information leaflet and once consented, infants will be randomly allocated to receive either IV ibuprofen or IV paracetamol for three days.
Following completion of the course of treatment, an echocardiogram will be repeated within 72 hours to reassess the ductus arteriosus. Conversion of PDA to non-hsPDA (TABLE 2), will be regarded as the trial end point for the primary outcome. If hsPDA persists following completion of the trial medications, participating infants will return to standard care and clinicians will be able to decide on further management of the PDA in keeping with the unit policy (FIGURE 1).
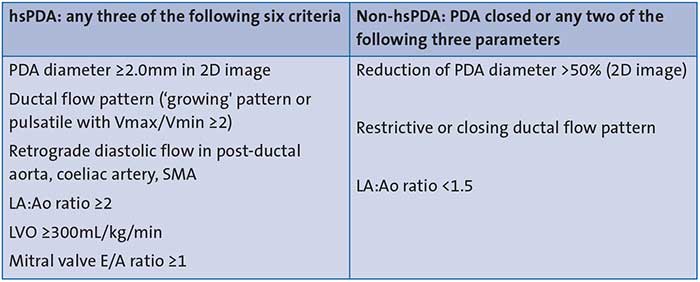
TABLE 2 Echocardiographic criteria for hsPDA/non-hsPDA. Key: LA:Ao=left atrial to aortic root ratio; LVO=left ventricular output; SMA=superior mesenteric artery; E/A=E wave to A wave ratio.
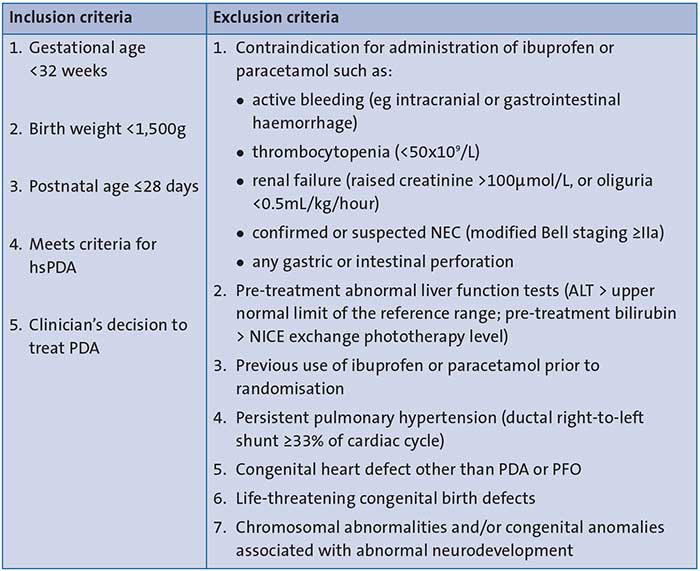
TABLE 3 The PAIR trial: inclusion and exclusion criteria. Key: NICE=National Institute for Health and Care Excellence; PFO=patent foramen ovale.
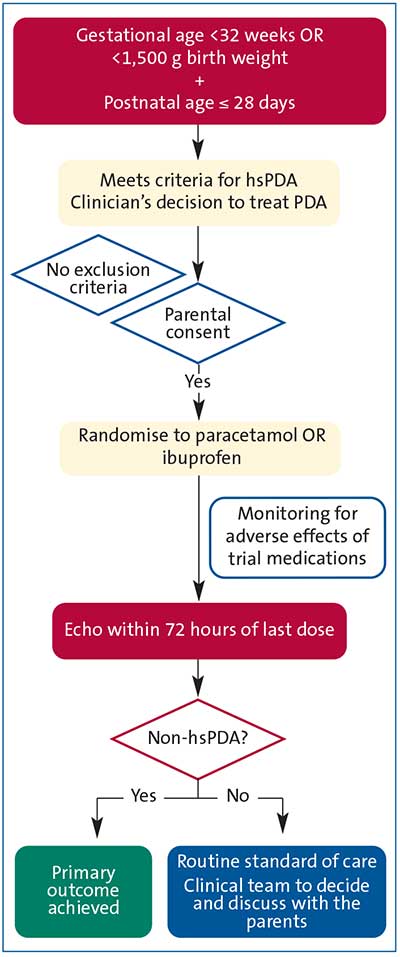
FIGURE 1 The PAIR protocol flowchart.
Monitoring during the trial
All infants on trial medications will receive standard care and monitoring. Their vital parameters will be recorded and analysed as per the standard unit policy. Blood tests such as full blood count, renal (urea and electrolytes) and liver function tests (liver enzymes and serum bilirubin), will be performed as baseline investigations to ensure suitability and as part of daily monitoring during administration of the trial medications.
Discussion
Association of PDA with adverse neonatal outcomes
Despite several clinical trials over the past decades, management of PDA in premature infants has remained largely unclear. While there are consistent reports of association of PDA with adverse neonatal outcomes (eg chronic lung disease, NEC, acute kidney injury and intraventricular haemorrhage), no clinical trial to date has demonstrated a causal relationship with these negative outcomes. A purist interpretation of such an observation is that PDA is an innocent bystander and better left on its own. On the other hand, there have been several purposeful reviews1,2 that have explored the reasons that preclude existing clinical trials from ascribing a causal relationship between ductal patency and adverse outcomes in extreme premature infants. These reviews highlighted issues in the existing trials with:
- selection bias (which results in choosing low risk infants where a PDA is likely to close spontaneously)
- methodological flaws (eg incorrect timing of pharmacological intervention – either too early or too late)
- inappropriate sample size
- contamination of the intervention arm by open label treatments
- use of the same dose of pharmacological treatment across a range of gestations
- bias in the selection of secondary outcomes.
In the last few years, we have witnessed a targeted approach in selecting infants who are likely to be affected by PDA. However, a standardised validated protocol for the diagnosis and treatment of hsPDA remains elusive.3,4 There is no uniform consensus on how a hsPDA is defined. Clinical trials continue to utilise a heterogenous and diverse set of clinical and echocardiographic parameters to reflect the haemodynamic effects of a PDA; hence, it has become difficult to draw meaningful conclusions.
Pharmacological therapies for preterm infants with a PDA
The pivotal roles of prostaglandin and oxygen in mediating ductus arteriosus closure were uncovered back in the 1970s, which led to the introduction of pharma-cological therapies for preterm infants with a PDA.5 Cyclooxygenase (COX) inhibitors block prostaglandin synthesis and are effective in ductal closure. Among the non-selective COX inhibitors, indomethacin was the first drug used for PDA treatment, presenting a closure rate of about 75-80%.6 It was widely used as first line standard therapy for several years; however, its use was marred by several unacceptable side effects primarily resulting from high vasoconstrictor action. Impairment in renal function (acute renal failure and chronic renal failure), oliguria, proteinuria, hyperkalaemia, cerebral white matter damage, NEC, intestinal perforation (especially when co-administered with corticosteroids) and platelet dysfunction were noted.7
Ibuprofen, another non-selective COX inhibitor, shares the same mechanism of action in effecting ductal closure as indomethacin, but it has lower vasoconstrictor side effects. Ibuprofen, therefore, has a relatively lesser impact on the microcirculation and consequent impairment of renal function. This difference may be partly explained by a preferential effect of indomethacin on COX-1 instead of COX-2 receptors, but there are other mechanisms that not fully understood.7
A recent systematic review compared ibuprofen with indomethacin in the treatment of hsPDA.8 It summarised findings from 39 randomised and quasi-randomised trials, which had enrolled a total of 2,843 infants. The review concluded that ibuprofen was not only as effective as indomethacin in closing a PDA, but also caused fewer side effects on the kidneys and reduced the risk of NEC. Now, ibuprofen has largely replaced indomethacin in most of the world and remains the only licensed medication for treatment of PDA in preterm infants in the UK.9 That said, although ibuprofen appears to be ‘friendlier’ than indomethacin, it is still far from ideal and is not without its own side effects; the hunt for a safer pharmacological agent continues.
Is paracetamol the way forward?
Vasoconstriction is generally believed to be the primary causative factor for renal impairment, cerebral ischaemia and NEC and these side effects are common with the use of non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen and indomethacin. Since the first case report by Hammerman et al in 2011,10 several observational studies have indicated paracetamol as a safer alternative medication to ibuprofen.
Paracetamol’s advantage over conventional NSAIDs can be related to its unique mechanism of action. Paracetamol is not a classic NSAID, having only weak anti-platelet and anti-inflammatory activity; it exerts mainly central effects (as an analgesic and antipyretic). It reduces the synthesis of prostaglandins through the inhibition of prostaglandin synthetase, as happens with NSAIDs, but acts at a different enzyme site, called the peroxidase region. More interestingly, paracetamol exerts a vasodilatory effect,11 which may explain the fewer adverse effects encountered with paracetamol use in clinical practice.
A recent national survey12 in the UK has highlighted that 82% (49 of 60) of neonatal intensive care units (NICUs) use paracetamol for management of hsPDA. It was observed that, while the majority of NICUs (65%) used it as a second-line treatment for PDA, 10% use it as a first-line treatment in preference to ibuprofen. While paracetamol has shown a lot of promise, definitive evidence to support its use in this vulnerable population is not yet established.
A systematic review13 of paracetamol recognised it as a promising alternative to ibuprofen with a better safety profile but was unable to provide practice recommendations due to the hetero-geneity in the methodology and designs of the available clinical trials. Assurance regarding its optimum dosage, route of administration, short and long-term implications from studies conducted so far remains limited.
We have reviewed all of the existing randomised controlled trials (RCTs) involving the use of IV paracetamol (TABLE 4). To date, only three RCTs were noted to compare IV paracetamol directly with IV ibuprofen. These were all single-centre trials. While Mashad et al14 observed similar efficacy of paracetamol in comparison to ibuprofen and indo-methacin, Tauber et al15 reported no effect with a first course of ibuprofen whereas Dani et al16 noticed paracetamol to be much less effective in comparisonzto ibuprofen in ductal closure.
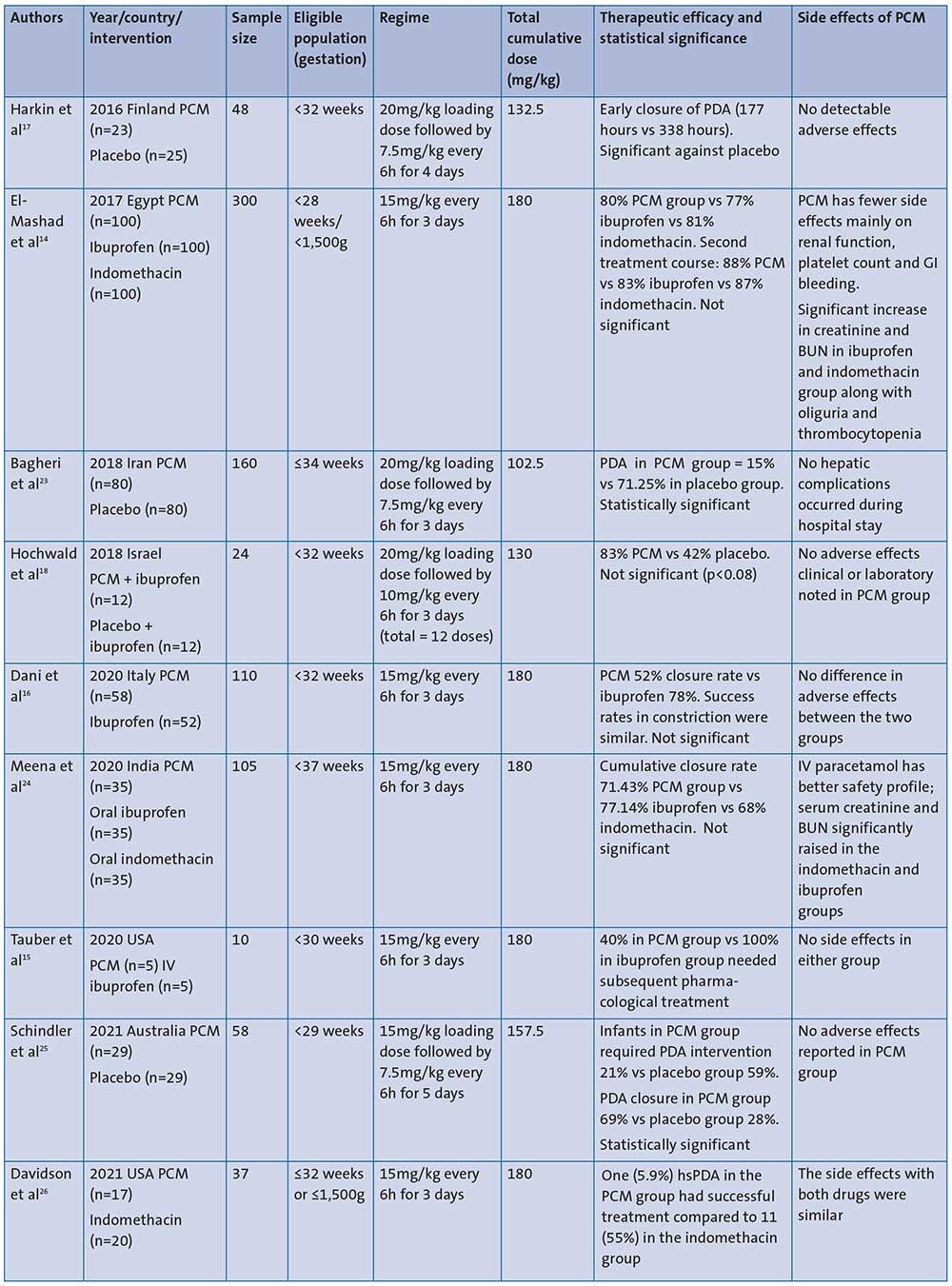
TABLE 4 Summary of RCTs using IV paracetamol for PDA management. Key: PCM=paracetamol; GI=gastrointestinal; BUN=blood urea nitrogen; echo=echocardiography.
Paracetamol administration in the PAIR trial
The dosage, duration, and the route of paracetamol administration in the PAIR trial has been carefully extrapolated from the available evidence in the literature. Although a number of these trials have used higher cumulative doses of paracetamol (ranging up to 180mg/kg for a course), lower cumulative doses of as low as 102.5mg/kg to 130mg/kg have been shown to be equally effective.17-19 In addition, cumulative doses of 180mg/kg have been associated with hepatic toxicity.20 Terrin et al20 recommended a limitation of dosing to 45mg/kg/day to avoid potential toxicity and still demonstrated similar efficacy rates to those of higher doses. From these, as well as from the pharmaco-kinetic study performed by Allegaert et al,6 the paracetamol treatment regime of loading dose of 20mg/kg followed by 10mg/kg every six hours for three days was chosen for the PAIR trial. This regimen promises a consistent steady state level of paracetamol and uses a relatively lower cumulative dose (130mg/kg) for the entire course.
One of the biggest advantages of the chosen paracetamol regimen in the PAIR trial is that, while it confers similar efficacy (up to 80% for closing ductal patency), in comparison to the higher cumulative doses used in other trials, there are no reported side effects in the literature. The current evidence regarding the pharmacokinetic and pharmacodynamic properties of paracetamol for hsPDA closure in extreme preterm infants can be seen in our recent article in a previous issue of Infant.21
Echocardiography in the PAIR trial
In the UK, echocardiograms are mostly performed by neonatologists. The echo-cardiogram indices for hsPDA have been extrapolated from the widely accepted recommendations by the European Special Interest Group on Neonatologist Performed Echocardiography.22 While the jury is still out on the evidence-base of echocardiogram parameters for diagnosis of hsPDA, both the treatment groups in the PAIR trial are diagnosed using the same echocardiogram parameters, there-fore the echocardiography is unlikely to introduce bias or interfere with the objective of the trial. The PAIR trial defines non-hsPDA as a state in which the PDA is either closed or is insignificant and therefore unable to affect the infant adversely.
PAIR: the way forward
Many neonatologists remain in equipoise on the perils of a PDA versus the safety of administering a pharmacological treatment. Nevertheless, neonatologists continue to use pharmacological treatments to manage a PDA. We envisage that paracetamol has the potential to provide a credible alternative to ibuprofen as the drug of choice.
Although the PAIR trial is a single-centre, open label pilot study, going forward the results of this pilot study will answer questions on the efficacy and long-term safety of paracetamol in management of hsPDA through a large-scale, double blinded, randomised controlled, non-inferiority multicentre phase III/IV PAIR trial. Such a trial will also aim to gather information on long-term neurodevelop-mental outcomes between 18-24 months corrected gestational age through follow-up data and PARCA-R questionnaire (Parent Report of Children’s Abilities – Revised). Paracetamol is a much cheaper drug than ibuprofen and, hence, a pharmacoeconomic analysis as part of this multicentre trial will enable us to assess cost effectiveness.
Trial progress and contact information
The PAIR trial is currently running as a single-centre randomised pilot trial. Approval from regulatory bodies such as the Research Ethics Committee, the Medicines and Healthcare products Regulatory Agency (MHRA) and the Integrated Research Application System (IRAS; ID 100053) have been obtained. The study is sponsored by Manchester University NHS Foundation Trust and is registered in the clinicaltrials.gov website (ClinicalTrials.gov identifier=NCT04986839). The trial duration is two years and the sample size for this pilot trial is 32 infants, which has been estimated from a local audit. The full trial protocol, study information leaflets and further information can be requested by contacting pairtrial@gmail.com or Twitter @PairTrial.
Or read this article in our
Tablet/iPad edition
- Paracetamol appears to have similar efficacy to ibuprofen in treating hsPDA but with an improved safety profile.
- The PAIR pilot trial compares paracetamol to ibuprofen in managing hsPDA in infants born at <32 weeks’ gestation or birth weight <1,500g.
Also published in Infant:
