

Bacterial colonisation in a neonatal intensive care unit
Newborn infants admitted to the neonatal intensive care unit (NICU) are highly vulnerable to colonisation and infection by multidrug-resistant bacteria (MDRB). Healthcare-associated infections due to MDRB are an emerging threat, associated with significant morbidity and mortality. This article analyses the MDRB colonisation rate in a level 3 NICU and its associated risk factors, as well as the subsequent development of infection.
Carolina Oliveira Gonçalves
Pediatric Resident, Child and Youth Department
carolinaoliveiragoncalves@gmail.com
Catarina Garcia
Consultant Neonatologist, NICU
Elzara Aliyeva
Clinical Pathologist
Marta Ferreira
Consultant Neonatologist, NICU
Consultant Neonatologist, NICU
Hospital Professor Doutor Fernando Fonseca, Amadora, Lisbon, Portugal
Gonçalves CO., Garcia C., Aliyeva E., Ferreira M., Barroso R. Bacterial colonisation in a neonatal intensive care unit. Infant 2023; 19(6): 222-26.
Newborn infants admitted to the neonatal intensive care unit (NICU) are highly vulnerable to colonisation and infection by multidrug-resistant (MDR) pathogens due to the immaturity of their innate and adaptive immune system and altered gut microbiota.1-4
Healthcare-associated infections due to multidrug-resistant bacteria (MDRB), such as methicillin-resistant Staphylococcus aureus (MRSA), extended-spectrum beta-lactamases (ESBL) and carbapenemase-producing Enterobacteriaceae (CPE), Serratia marcescens and vancomycin-resistant Enterococcus faecium (VRE) are an emerging threat, associated with significant morbidity and mortality.2,5-8
The colonisation of the skin and mucous membranes by a MDRB is a demonstrated risk factor for subsequent development of infection;7,9,10 however, only a subset of colonised infants develops symptomatic infection.1,5 Several studies have identified a variety of other risk factors that predispose neonates to colonisation with MDRB, such as low gestational age, low birth weight, type of delivery, length of stay, use of antibiotics, invasive devices, surgery and vertical transmission.1-3,5-7,9-12
Aims, methods and materials
The aim of this study was to analyse the MDRB colonisation rate, the risk factors associated with colonisation by MDRB and the subsequent development of infection in neonates admitted to the NICU.
We conducted a case review of the clinical files of all newborns admitted to the level 3 NICU of Hospital Professor Doutor Fernando Fonseca in Lisbon’s metropolitan area between November 2018 and November 2019. The NICU admits patients of all gestational ages and has a capacity of 20. The newborn data analysed included:
- birth location (inborn/outborn)
- type of delivery
- gestational age
- birth weight
- a neonate’s colonisation status at admission and during the NICU stay
- antibiotic therapy upon admission
- use of a central line and mechanical ventilation
- development of infection (day of infection)
- day of initiation of enteric feeding.
We also analysed the mothers’ hospital length of stay and antibiotic therapy before delivery.
The studied cohort was divided into two groups:
- Group A – colonised infants. Group A was further subdivided into:
i) colonised and infected infants
ii) colonised and non-infected infants.
- Group B – non-colonised infants.
In group A, we also assessed the volume of mother’s own milk (MOM) administered. In the colonised and infected infants, we assessed the volume of MOM from admission until the day of infection. In the colonised but not infected infants, we assessed the volume of MOM from admission until day 9 (the average day on which colonised neonates became infected).
Definitions
Prematurity was considered as birth at <37 weeks’ gestation and extreme prematurity as <28 weeks’ gestation.
Early-onset sepsis (EOS) was defined as a bloodstream infection in the first 72 hours of life and late-onset sepsis (LOS) as a bloodstream infection after the first 72 hours. Both culture-proven and culture-negative cases (ie, those with clinical features of LOS and suggestive laboratory alterations but sterile blood cultures) were counted. Infants were considered as Group A(i) ‘colonised and infected’ if they developed LOS during their hospital stay. LOS was considered infection by the same pathogen of colonisation if the infection was diagnosed after positive colonisation status and if the same microorganism was identified in blood cultures.
Swab testing
In 2018 a colonisation screening protocol was adopted in which three samples were collected from each patient: a nasal swab for MRSA and two rectal swabs for ESBL and CPE, and S. marcescens. Samples were collected upon admission and once a week during the hospital stay. Once a MDRB was isolated, screening for that pathogen was no longer repeated and, importantly, contact isolation measures and cohorting of colonised newborns was implemented until discharge.
Nasal swab specimens were inoculated on CNA agar, and rectal swabs were inoculated on a CHROMID CARBA SMART selective chromogenic media bi-plate and on CHROMID ESBL selective chromogenic media. Rapid immuno-chromatographic assays were also performed: CLEARVIEW PBP2a SA culture colony test for the detection of penicillin-binding protein 2a (PB2a) in the presence of MRSA, and RESIST-5 OKNVI for the detection of CPE-producing specimens (Klebsiella pneumoniae carbapenemase, oxacillin-hydrolysing lactamase, New Delhi metallo-β-lactamase, Verona integron-encoded metallo-β-lactamase and imipenemase). Suspected colonies of S. marcescens and ESBL-producing bacteria were identified through VITEK2 for ID Cards and AST Cards.
Results
Neonate data
A total of 358 newborns were admitted to the NICU during the study period. Of these, 294 neonates were analysed and 64 were excluded due to lack of data. There was a slight predominance of males (58.2%). Cohort data can be seen in TABLE 1.
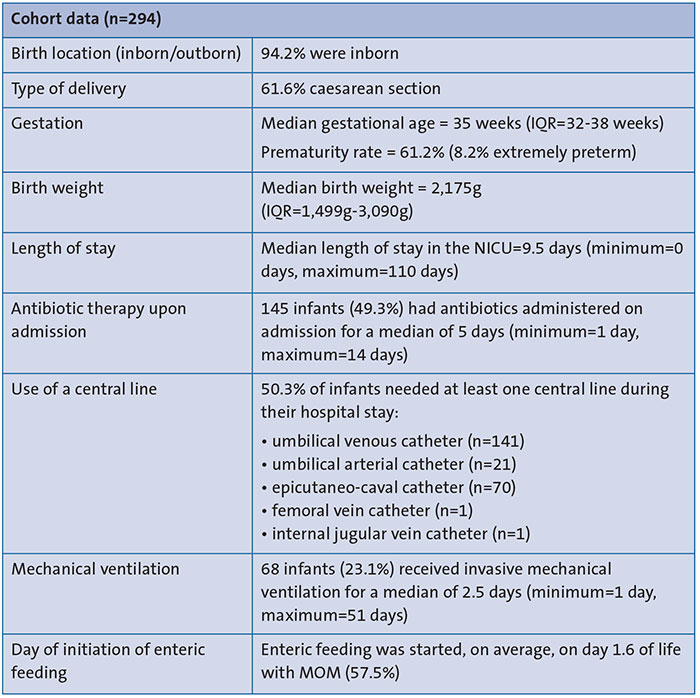
TABLE 1 Data analysis for the study period. A total of 358 newborns were admitted to the NICU. Of these, 294 neonates were analysed and 64 were excluded due to lack of data. Key: IQR=interquartile range.
Maternal data
2.8% of mothers received antibiotics prior to childbirth. The main indications were:
- confirmed or highly suspected maternal infection (31.5%)
- preterm premature rupture of membranes (31.5%)
- group B Streptococcus (GBS) colonisation (15.7%).
The most common antibiotic administered was ampicillin, either in monotherapy (37.1%) or in association with other antibiotics, such as erythromycin (18.0%), gentamicin (7.9%) and clarithromycin (4.5%). Over one-fifth of the mothers (21.8%) were admitted more than one week prior to childbirth. The most frequent hospital admission causes were:
- risk of preterm birth (28.8%)
- pre-eclampsia/HELLP syndrome (17.0%)
- preterm premature rupture of membranes (15.3%)
- vaginal bleeding (11.9%)
- intrauterine growth restriction (8.5%).
Swab testing
During the study period, 896 nasal swabs and 1,637 rectal swabs were performed. A total of 83 infants (28.2%) were found to be colonised during their hospital stay (Group A). From the 83 colonised neonates, 73.5% were colonised by one MDRB, 20.5% by two MDRB and 6% by three (TABLE 2). The most frequent overall MDR colonisation agent was ESBL-producing Enterobacteriaceae (n=48), followed by MRSA (n=28), S. marcescens (n=25) and CPE (n=9).
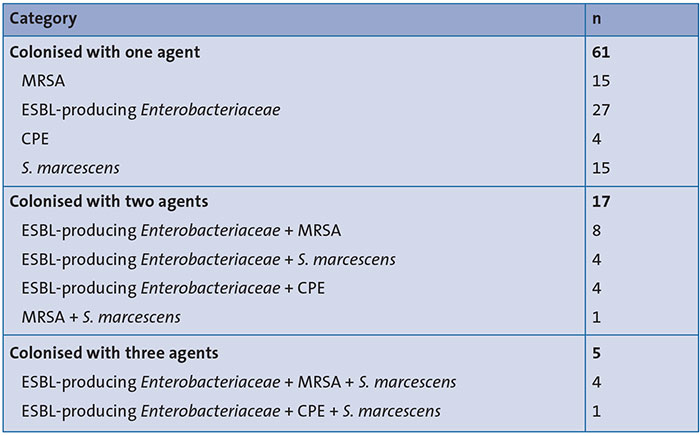
TABLE 2 Group A: distribution of MDR colonisation agents (n=83).
Colonisation
The median time from admission to colonisation was 10 days (minimum=0 days, maximum=50 days). Among the colonised neonates, 12% were colonised upon admission to the NICU. In this subgroup, the median time between birth and admission to the NICU was 1 day (minimum=0 days, maximum=5 days). The most frequent MDR colonising agent was ESBL-producing Enterobacteriaceae (n=8), followed by MRSA (n=1), S. marcescens (n=1) and CPE (n=1).
Their median gestational age and mean birth weight were, respectively, 37.5 weeks and 2,908g. Most (60%) were born by vaginal birth, 90% were inborn and initially admitted with their mothers to the obstetric ward. Only one was born at home and later admitted to the NICU in the first 24 hours of life. None of these neonates were subsequently found to be infected.
Colonised infants (Group A) vs non-colonised infants (Group B)
When comparing Groups A (colonised infants, n=83) and B (non-colonised infants, n=211), the colonised infants had a lower gestational age (median of 31 vs 36 weeks, p<0.001) and a lower birth weight (median of 1,490g vs 2,445g, p<0.001). Also, the colonised infants were more likely to be born via caesarean delivery (69.9% vs 58.3%, p=0.660) and had a longer hospitalisation in the NICU (median of 31 vs 6 days, p<0.001). The mothers of Group A infants were more likely to have received antibiotics (39.8% vs 31.8%, p=0.235) and to have been admitted at least one week prior to delivery (34.9% vs 19.4%, p=0.009).
Upon admission to the NICU, many Group A infants received antibiotic therapy (68.7% vs 41.7%, p<0.001); were more likely to have had invasive ventilation (39.8% vs 16.6%, p<0.001), and a central line (78.3% vs 39.3%, p<0.001). Enteric feeding was started later in Group A infants (mean 2.2 vs 1.3 days). In both groups, most newborns started with MOM (Group A 66.3% vs Group B 54.0%, p=0.056). TABLE 3 displays the frequency of colonised and non-colonised newborns, with or without symptomatic infection.
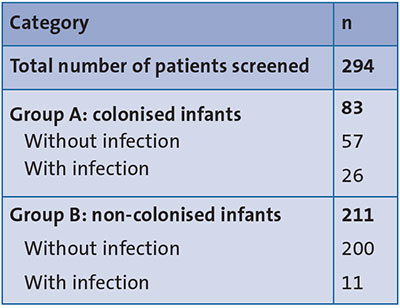
TABLE 3 Distribution of infants according to their colonisation and infection status.
Group A: colonised infants
For further analysis, the Group A colonised infants were subdivided into Group A(i) ‘colonised and infected’ and Group A(ii) ‘colonised-only’.
When comparing the Group A(i) ‘colonised and infected’ with Group A(ii) ‘colonised-only’ (non-infected) infants, we found that they had a lower gestational age (median of 28 vs 33 weeks, p<0.001), a lower birth weight (942.5g vs 1,680g, p<0.001), and a longer hospitalisation (54.5 vs 25 days, p<0.001). Furthermore, they were more likely to be born via caesarean delivery (76.9% vs 66.7%, p=0.345) and their mothers were more likely to have received antibiotics (46.2% vs 36.8%, p=0.457) and to have been admitted at least one week prior to delivery (38.5% vs 33.3%, p=0.649).
Group A(i) ‘colonised and infected’ infants were also more likely to have received invasive ventilation (69.2% vs 26.3%, p<0.001) and to have had a central line inserted (100% vs 68.4%, p=0.001).
Colonised and infected infants
Among the colonised infants, 31.3% (26 out of 83) developed LOS, occurring at a median of 9 days of life. During the hospital stays, 30 episodes of LOS were diagnosed in 26 infected infants (four patients had two episodes of LOS). In 13 of these, the agent was the same as the colonisation agent. Therefore out of 26 colonised infants, 13 infants developed a LOS concordant with the colonising pathogen (50%) (TABLE 4).
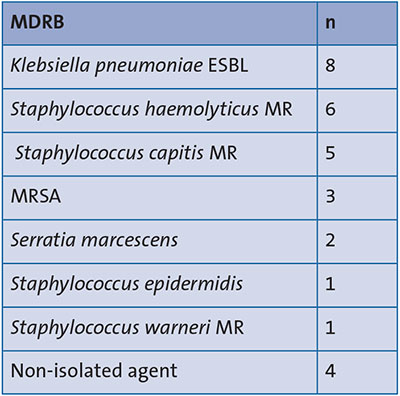
TABLE 4 Frequency of organisms causing LOS in Group A infants, n=30 (30 episodes of LOS were diagnosed in 26 infected infants – four patients had two episodes of LOS).
Colonised infants: enteric feeding
Group A colonised infants began enteric feeding later than Group B non-colonised infants.
Group A(i) ‘colonised and infected’ infants started enteral feeding on average on day 3.3 of life, in contrast with the Group A(ii) colonised but non-infected infants, which started on day 1.8. Enteric feeding was started with MOM in most newborns of both subgroups (88.5% in Group A(i) ‘colonised and infected’ and 57.9% in Group A(ii) ‘colonised non-infected’ newborns).
When comparing the volume of ingested MOM between the colonised infants, we found that:
- at the time of sepsis, 80.8% of the Group A(i) ‘colonised and infected’ infants’ intake was with at least 50% of MOM
- 61.4% of Group A(ii) colonised-only infants at day 9 of life (or at discharge where stay was <9 days of life), had at least 50% of MOM comprising total fluid intake (80.8% vs 61.4%, p=0.81).
Whole cohort
Regarding the whole cohort, 11 infants (3.7%) died in the NICU during their hospital stay:
- eight infants died from LOS, three being colonised by the same MDRB pathogen responsible for the sepsis (Klebsiella pneumoniae ESBL n=2 and S. marcescens n=1)
- one died from multiorgan failure in the context of symptomatic congenital syphilis
- the remaining two infants died in the first 72 hours of life, non-colonised and with EOS.
The mortality rate was similar between Groups A (3 out of 83 = 3.6%) and B (8 out of 211 = 3.8%).
Discussion
Early microbial colonisation of the newborn is crucial for immune and gastrointestinal development. Occasionally, these colonising agents may become opportunistic pathogens. Neonates, especially those born preterm, are particularly vulnerable to colonisation and infection by MDRB.1,13,14
In our setting, the prevalence of MDRB colonisation was 28.2%, similar to others reported in Germany (26.2%)12 and Italy (28.8%)3 Much higher rates have been reported in lower-income countries such as the Philippines (55%),15 Serbia (59.2%)16 and India (88.7%).1 However, the heterogeneity in the local epidemiology and the differences in surveillance policies and hygiene measures, make it complex to compare data from different NICUs.3
Gestational age, birth weight, length of stay, use of central lines and mechanical ventilation are identified risk factors for colonisation. Furthermore, colonised infants in our sample had a significantly higher frequency of antibiotic therapy on admission than non-colonised ones. This may predispose infants to colonisation, since treatment with antibiotics frequently leads to gut colonisation with MDRB by selecting resistant gut microbiota.1-3,5-7,9-12 Delivery by caesarean section, associated with increased risk of carriage of hospital-related pathogens compared to vaginal delivery, was higher in Group A (69.8% vs 58.3%); however, this was not statistically significant.13
Hospital admission of the mother at least one week prior to birth, was also a risk factor for colonisation, with statistical significance. Additionally, among the Group A neonates, 10 (12%) were already colonised on admission to our NICU, most by ESBL-producing Enterobacteriaceae. We hypothesise that the colonisation agents were acquired by vertical transmission or during rooming-in at the obstetric ward. It could be useful to screen for the mothers’ carriage of ESBL-producing Enterobacteriaceae, especially in those admitted to the hospital more than 48 hours prior to delivery. This might help detect early colonisation and to implement earlier neonatal isolation measures.16,17
The median time from admission to colonisation was 10 days, which suggests that hospital stay is an important risk factor for colonisation. Several studies corroborate the role of length of stay in the NICU as a prominent factor in the colonisation by a MDRB.1,7,12,18 Therefore, premature newborns, who generally require a longer NICU stay, are at a higher risk of MDRB colonisation during their hospital stay.19 Thus, establishing screening procedures allows prompt identification of asymptomatic colonised infants and appropriate control measures to prevent infection.20
Alongside hand hygiene and universal screening upon admission (and weekly, thereafter), we implement contact isolation precautions and cohorting of newborns whenever a colonised infant is detected in our NICU. Since healthcare professionals are the first line of defence against healthcare-associated infections and the cross-transmission of MDRB in healthcare settings, frequent infection prevention and control training actions are key.
Colonisation with MDRB is considered an important risk factor for subsequent infection.7,9,10 and our results are in line with these findings as the frequency of LOS observed in colonised infants was significantly higher than in non-colonised ones (31.3% vs 5.2%, p<0.001). The rate of LOS following colonisation in a systematic review was lower than in our cohort and varied from 0 to 19.8%.18 However, since most studies only took blood culture positive sepsis into account, this might have led to an underestimation of the true burden of hospital-acquired sepsis and may explain the higher rates that we found.21
In our ward, the MDRB responsible for LOS were the same as the colonisation agent in 50% of cases. Other studies have presented a low overall concordance of colonisation organisms and invasive infectious agents. A retrospective study of neonates with suspected sepsis in Haiti found a 20.6% concordance of rectal swab isolates and blood cultures for gram-negative bacteria isolates.22 A systematic review that analysed the results of 27 studies found 7.9% concordant blood-stream infections with gram-negative bacteria in colonised infants18 and a retrospective study in India reported 7% concordance. Despite the low concordance of colonising pathogens and infectious agents, a knowledge of colonisation and surveillance of sepsis is useful for guiding infection control measures.12
Regarding enteral nutrition, our hospital is a part of Unicef’s Baby-Friendly Hospital Initiative and breastfeeding is highly recommended and encouraged in our NICU. Remarkably, in our cohort, enteral feeding with MOM was started on average on day 1.6 of life (57.5%). Every day of delayed enteral feeding increases the risk of nosocomial infections.23 In our cohort, enteral feeding was delayed in the colonised infants (2.2 vs 1.3 days). Since starting enteral feeding with MOM is a priority in our NICU, and colonised infants had a lower gestational age and a lower birth weight, enteral feeding might be delayed by up to 72 hours in order to prevent the use of formula feeding.
When comparing the two subgroups of colonised infants (infected vs non-infected), enteral feeding with at least 50% of MOM comprising total fluid intake was reported in higher frequencies in the colonised and infected newborns (80.8% vs. 61.4%, with no statistical significance). Although our results do not support the well-established protective effect of MOM regarding infection in colonised infants, we are pleased with our high frequency of enteral feeding with MOM, especially in high-risk neonates.
Conclusions
The increase of MDRB in NICUs is a growing concern as they have become an important cause of nosocomial infections, associated with significant morbidity and mortality. Most of the colonisers found in our cohort were gram-negative bacteria, with ESBL-producing Enterobacteriaceae being the most frequent MDRB isolated. Therefore, screening mothers admitted to our hospital prior to delivery for ESBL-producing Enterobacteriaceae could allow us to identify and establish strict infection control measures earlier and therefore prevent infection.
Limiting antibiotic therapy and implementing isolation of colonised infants is pertinent but we should also introduce staff cohorting on our NICU. Continued training for healthcare professionals remains a key element for preventing and controlling infection by hospital-acquired MDRB.
Author contributions
COG: study design, implementation, conducting the project, data analysis, drafting the article and final approval of the published version. CG: study design, data analysis, critical review of the article, final approval of the published version.
EA: critical review of the article and final approval of the published version.
MF: critical review of the article and final approval of the published version. RB: idea for the article, critical review of the article and final approval of the published version.
Or read this article in our
Tablet/iPad edition
- Newborns in the NICU are highly vulnerable to colonisation and infection by multidrug-resistant bacteria.
- Implementation of colonisation screening in mothers prior to delivery would permit earlier infection control measures.
- Limiting antibiotic therapy and implementing isolation measures and staff cohorting in NICUs remains a key element for infection control.
Also published in Infant:
