

The role of simulation in preparing a response to the COVID-19 pandemic
In response to COVID-19, simulation has been used to embed practical skills such as donning and doffing of personal protective equipment and scenario-based logistics of proposed COVID-19 patient flows. We have developed small staff group training sessions, alongside larger scale multidisciplinary team sessions and used simulation to guide the development of our standard operating procedure. We have also created online training resources to reach a larger number of staff within the neonatal unit (NNU). In this article we share our experiences to help others develop their own ideas on the plethora of ways that simulation can aid a response to the COVID-19 outbreak and any other future advances within the NNU.
Jennifer Peterson
MBChB, MRCPCH, MA
Neonatal GRID ST6
jennifer.peterson@hotmail.co.uk
Ruth Gottstein
MBBCh, BAO, FRCPCH, MSc
Neonatal Consultant
Ranganath Ranganna
MBBS, MRCPCH
Neonatal Consultant
St Mary’s Hospital, Manchester University NHS Foundation Trust
Emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, COVID-19) has caused a worldwide pandemic. The response to this health crisis needs to be rapid and involve multidisciplinary team (MDT) working. The advice from the government and regulatory bodies can fluctuate and is ever-evolving. The challenges are numerous as departments and staff members may have clashing priorities, there are staff shortages and an even more variable staff rota than usual, unease with new working practices, unfamiliarity with personal protective equipment (PPE), and reduced time for staff training and dissemination of information.
Health care needs to implement complex training at ground level – fast and flexible solutions to practically implement COVID-19 prevention strategies and procedures. Our experience at St Mary’s Hospital, Manchester, has shown that simulation can help address these chall-enges through problem solving, logistical testing and building familiarisation of MDT working in novel circumstances.
COVID-19 and newborn services
At the time of writing, there is little evidence available regarding the impact of COVID-19 on newborn infants. The evidence to date would suggest little risk of vertical transmission (no evidence of virus RNA on placental swabs, amniotic fluid, cord blood) nor in breast milk.1,2 However, due to the rapid spread of COVID-19 and the novel nature of the virus, there is paucity of research in this area. In addition, the risks of transmission of COVID-19 to infants have to be balanced against the detriment of separation after birth.3 While leaving a newborn infant with its COVID-19 positive mother may increase the risk of postnatal virus transmission, there is also potential harm in terms of bonding and breastfeeding if the infant is completely isolated from its mother for a sustained period after birth. Based on this, our department has decided that infants born to COVID-19 suspected/positive mothers who are well will remain with their parents and we will only admit infants to the neonatal intensive care unit (NICU) if they require support.
Simulation at St Mary’s Hospital
The newborn service at St Mary’s Hospital is a large tertiary level medical and surgical neonatal unit that regularly uses simulation in a variety of ways to familiarise and improve technical and human factors skills in multiple contexts. The unit has a pre-existing positive simulation culture – simulation is embedded into the functioning of the unit with MDT in situ simulations occurring twice a week, alongside additional regular joint simulation sessions with obstetrics, midwifery and anaesthetics.
Simulation can be used in simple and very effective ways to ensure safe and robust patient care and staff safety. Ideally, the first time a system or flow process is tested should not be with a real patient. Use of simulation helps to promote patient safety without exposing a patient to risk. TABLE 1 shows the different applications of simulation in the context of COVID-19, which will be discussed in this article.
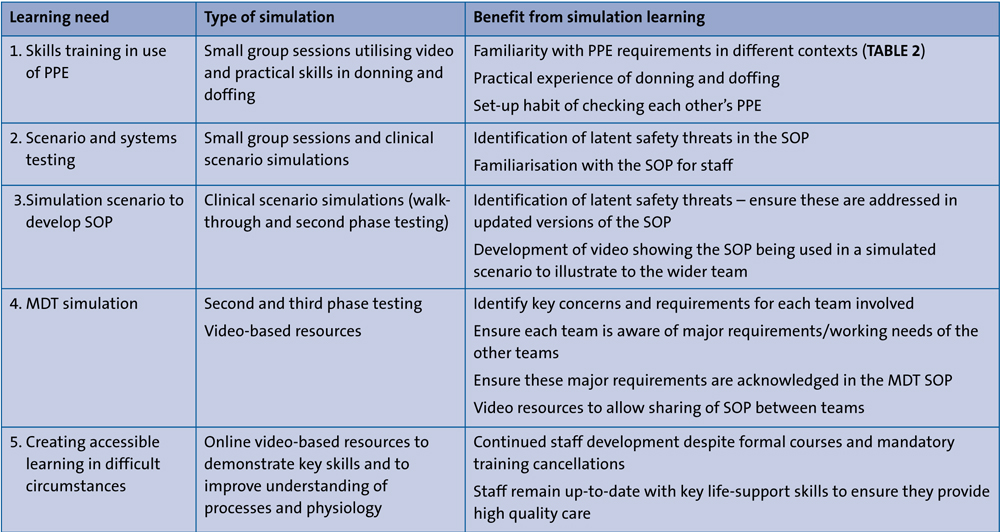
TABLE 1 Different applications of simulation in the context of COVID-19. Key: PPE= personal protective equipment, SOP=standard operating procedure, MDT=multidisciplinary team.
1. Skills training in use of PPE
PPE is utilised to varying extents on a daily basis and is familiar to the majority of healthcare workers; for example, aprons and gloves should be worn for blood taking. However, in the midst of a pandemic, risks may be more significant and staff may experience higher levels of anxiety regarding PPE including uncertainty over which type of PPE to wear and when. Familiarity does not equate to good practice and staff may not have sufficiently robust personal habits, in terms of applying/removing their usual PPE, to ensure they can do so correctly in the context of a pandemic pathogen. To further compound the issue, there have been numerous updates regarding the level of PPE to be worn in various situations with potential for confusion and/or misinterpretation.
Videos of donning and doffing procedures have been developed by numerous hospitals and trusts across the country. These videos are a helpful introduction; however, they should not be the only form of training that staff are able to access. Our experience of using these videos was that staff had often watched them prior to the session but when questioned, they struggled to remember the sequence of donning and doffing or would confidently proceed but with errors that could lead to self-contamination with a COVID-19 positive patient.
Over a one-week period, simulation sessions were run utilising pre-existing teaching slots on the unit. Staff watched the donning and doffing videos on the trust intranet and then had to physically don and doff PPE themselves. Two participants donned then doffed at a time. This ensured facilitators could monitor the process and check it was performed safely and correctly. The other participating staff members watched multiple times and acted as checkers for each other. This repetition meant each person had numerous encounters with the donning and doffing sequence, thus embedding the skills.
Over the initial one-week training period, 40 staff members were trained, including 80% of junior doctors (the 20% that were missed were self-isolating and not present at work) and reaching members of the 250+ neonatal nursing team. The sessions will continue through-out the COVID-19 outbreak. TABLE 2 and FIGURE 1 show the different PPE recommendations for neonatal teams in the context of COVID-19.
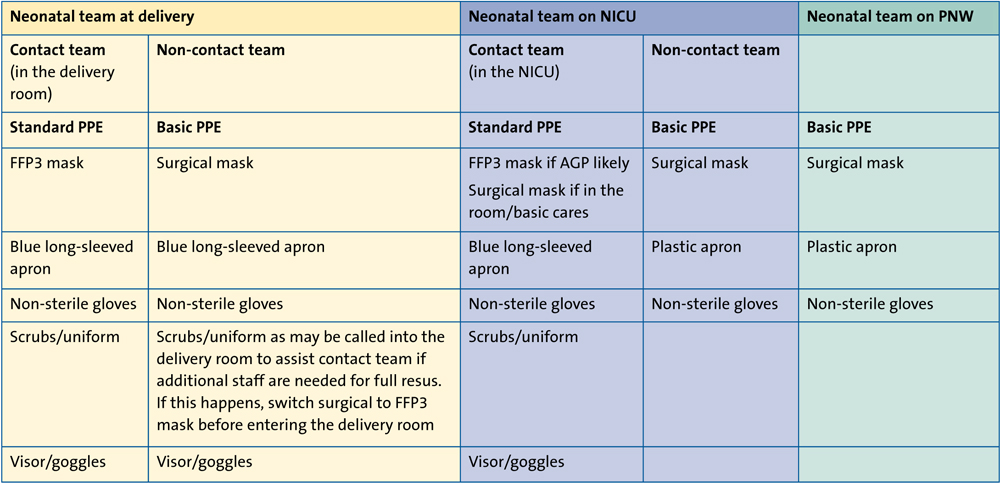
TABLE 2 PPE recommendations for neonatal teams (taken from our SOP version 3.10, 3 April 2020). Key: PNW=postnatal ward, FFP3= filtering face-piece particles mask type 3, AGP=aerosol generating procedures (include intubation, suctioning, continuous positive airway pressure, high-flow therapy).
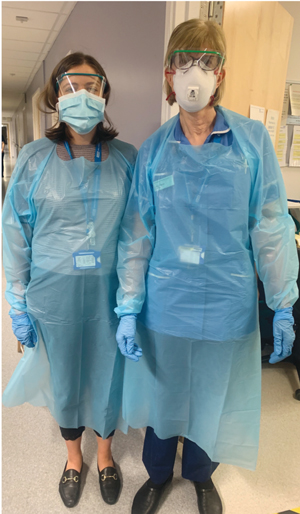
FIGURE 1 The different COVID-19 PPE recommendations for neonatal staff. Left: Non-contact staff remain outside the delivery room (or theatre or designated NICU room) and assist with equipment and medications for the contact team. Non-contact staff wear an apron, gloves, visor/goggles and a surgical mask. Right: Contact staff remain inside the delivery room and wear an FFP3 mask because of the risk of AGPs
2. Scenario and systems testing
The neonatal infection control lead, departmental lead and nursing leads met to discuss how to manage the delivery and potential resuscitation of infants born to COVID-19 suspected/positive mothers, and how to manage infants who require admission to the NICU. Advice from available research and guidance from relevant professional bodies (eg Royal College of Obstetricians and Gynaecologists and the British Association of Perinatal Medicine) was used to create a standard operating procedure (SOP).
The SOP was then tested using our own phase-structured simulation approach:
- First phase testing: The initial SOP was used while performing a walk-through (members of the SOP development team physically walked through the delivery and admission areas to ensure the proposed SOP would be practical). This process is simple, easy to perform and allows identification of more obvious and immediate issues.
- Second phase testing: The SOP is tested in a full simulation scenario using a low-fidelity infant manikin and physically performing each stage of the SOP. This involved senior members of the SOP development team (neonatal consultants and neonatal matrons).
- Third phase testing: Scenarios were run with NICU staff members to allow the SOP to be used in simulated clinical scenarios. This gave the SOP development team an opportunity to get feedback and make updates to ensure it is as clear as possible for users. This type of simulation will be ongoing throughout the COVID-19 pandemic.
3. Using simulation to develop a neonatal SOP: lessons learnt
Resuscitation at birth of an infant delivered to a COVID-19 suspected/positive mother
An SOP was developed for a variety of neonatal resuscitation scenarios, which attempted to minimise risks to staff through the creation of a contact and a non-contact team. The contact team would don PPE, including an FFP3 mask (TABLE 2), would be present in the delivery room and provide hands-on resuscitation if required. The non-contact team would don PPE involving a surgical face mask, as they would remain outside the room providing equipment and assistance as needed to the contact team. This ensured clear task allocation, minimisation of the number of staff members potentially exposed and minimal contamination of emergency equipment.
In the usual full neonatal resuscitation situation, a yellow emergency trolley laid out in an ‘ABCD’ structure is used. Through the simulated walk-through process we recognised that any equipment taken into a COVID-positive environment has to be discarded at the end of the resuscitation. Our labour ward has two emergency trolleys servicing 20 delivery rooms, in addition to one in the obstetric theatres. Therefore, concern was that if an emergency trolley was taken into a delivery room and used for an infant born to a COVID-19 positive mother, the destruc-tion of the remaining contents of that trolley and the decontamination and restocking process would be extensive, and the trolley would be unavailable for other possible resuscitations in the meantime.
By creating the contact and non-contact teams it was clear that in the event of a full resuscitation the non-contact team could usefully gather necessary equipment and draw up emergency medications outside the room. When simulating various scenarios using the contact and non-contact team approach, it was clear that a runner was needed within the room to pass requests from the contact team to the non-contact team. It was recognised that the midwife already in the delivery room would be in the most appropriate position to do this.
Transport to the neonatal intensive care isolation room
It was identified that if the usual transport incubator was used to move an infant born to a COVID-19 suspected/positive mother from the delivery suite to the NICU, again the extensive decontamination process could mean this incubator would be unavailable for some time for subsequent infants. This was highlighted through simulation and our SOP development team worked with NICU equipment technicians to create a specific COVID-19 transport incubator (FIGURE 2). Over the course of subsequent simulations the equipment that might be needed on this COVID transport incubator was refined. This included identification that the COVID incubator needed a dedicated thermometer as the newly designated dedicated COVID obstetric theatres were previous gynaecology theatres and did not have neonatal equipment.
In addition, simulation scenarios with the full MDT in theatres identified issues with PPE provision. When attending a delivery, the NICU team had been expecting PPE to be available at the MDT donning station by the theatres. Whereas, the theatre team was expecting the NICU team to bring its own supplies of PPE. We therefore modified our transport incubator to include provision of PPE for the entire NICU team, while agreeing with theatres that initial responders (the contact team) could utilise theatre PPE and be ready earlier.

FIGURE 2 Through simulation we discovered that we needed a specific COVID-19 transport incubator.

FIGURE 3 Simulating the admission process to the NICU.
Admission to NICU
We used a walk-through simulation on the admission process to the NICU for infants born to COVID-19 mothers, where members of the SOP development team physically walked through the delivery and admission areas to ensure the proposed SOP would be practical. We updated the SOP following the walk-through and then ran full simulated clinical scenarios using team members to test the logistics and practicalities. This process raised issues (such as the lack of a specific airway trolley for our COVID-19 isolation room), which were addressed by the SOP development team. Simulated scenarios were then repeated with our clinical medical and nursing teams.
4. MDT simulation
MDT working has been pivotal in the development of our neonatal SOP; neonatal care is inextricably linked to maternal care. Therefore, through each stage of the SOP development the neonatal SOP development team worked closely with the obstetric, midwifery and anaesthetic SOP development teams. A series of simulated clinical delivery scenarios were run with the entire MDT, allowing potential issues to be addressed, for example, when to call the neonatal team. Due to the process of donning before entering the room, the neonatal team requires additional advance warning time; having an MDT approach allowed the other teams to recognise and build this into their department’s SOP.
5. Creating accessible learning in difficult circumstances
To avoid spread of the COVID-19 virus many face-to-face mandatory and educational courses and conferences have been cancelled for the coming months. This includes Newborn Life Support (NLS) courses and in-house mandatory training courses, raising concern that staff are not being given the opportunity to have crucial skills reviewed and refreshed.
This is of particular concern in the current COVID-19 outbreak. For example, a midwife attending a COVID-19 positive mother may be left to initiate NLS alone for a longer period than usual while the neonatal resuscitation team dons PPE – donning PPE can take 3-5 minutes when done properly.
There is an ethical obligation to ensure that as many midwifery and neonatal staff as possible have the most up-to-date NLS skills and our simulation team created video-based resources to provide the same content as the cancelled face-to-face mandatory training. These videos allow staff to access NLS refresher sessions either remotely or in a one-to-one session with the midwifery or neonatal education team. The videos ensure content is consistently delivered by an expert NLS certified professional instructor. They contain a lecture-style overview of the physiology guiding newborn resuscitation and practical demonstrations of key NLS skills. The videos can be accessed via the staff intranet or staff email and can be downloaded onto education team computers/tablets to allow staff to easily watch and then practise on a manikin.
The videos were filmed using iPhones and then edited into the final teaching video using the freely available iMovie software, which is user-friendly and has easily accessible support via the Apple website.
Tips for successful simulation
Simulation does not require extensive experience to yield useful results. As illustrated in this article, simulation can be used effectively in systems and safety testing, and development and modification of a SOP. This type of simulation does not require prior experience, however, simulation of clinical scenarios should always be run by someone with experience of debriefing in order to manage the learning and psychological safety of the staff participating in the simulation.
In our experience, staff are enthusiastic and insightful following simulations to aid systems testing. However, it is vital to make it clear to participating staff that the key aim of the simulation is to test the system – not to covertly test the staff.
It is important to include a pre-brief; a conversation before the simulation begins between facilitators and participants outlining the set-up, scenario and providing reassurance that participants are helping test the proposed system/SOP.
It needs to be made clear to participants that any major concerns about aspects of observed care would be addressed privately afterwards. The focus of the debrief will be on gathering feedback about positive and negative aspects of the system tested, rather than commenting on an individual participant’s skills or performance.
Conclusion
Simulation has played an important role in developing a COVID-19 specific neonatal SOP for safe and effective care at St Mary’s Hospital. TABLE 3 summarises the learning points contributing to this. Our SOP and training videos are available for others to use – please direct any questions or comments to the corresponding author.
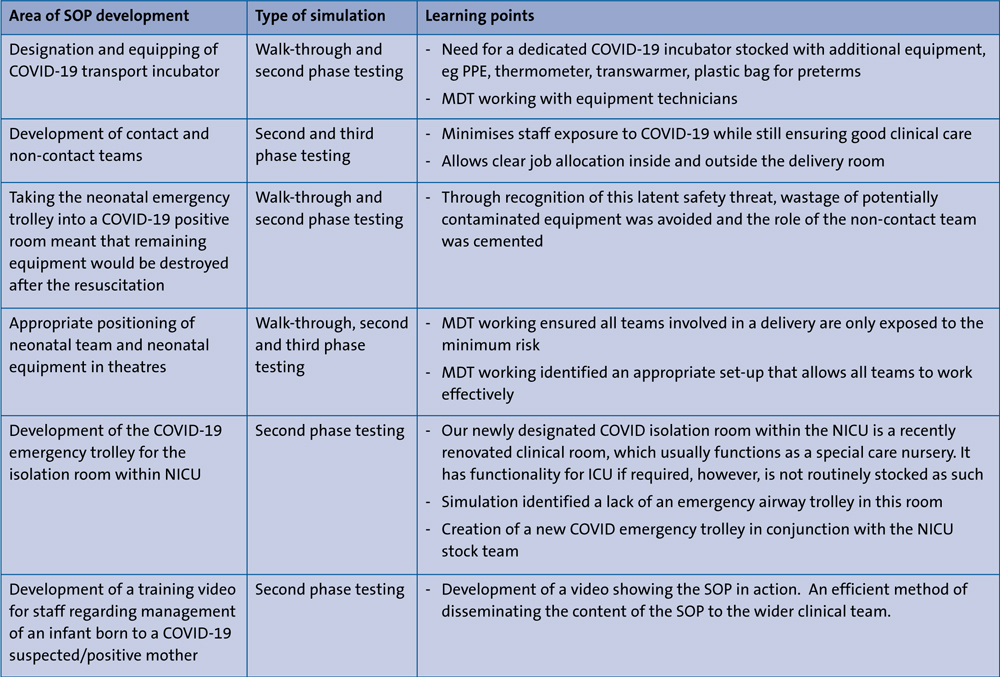
TABLE 3 The role of simulation in development of a COVID-19 specific neonatal SOP for safe and effective care.
Acknowledgement
The authors are grateful for the contributions of: Tracey Bibbi and Penelope Heap, NICU Information Goverance Team; Dr Gasiorowski, NICU Infection Control Lead; Dr Edi-Osagie, NICU Clinical Head of Division; Alison Smith and the NICU Education Team.
Or read this article in our
Tablet/iPad edition
- The current COVID-19 outbreak has raised concern about providing high quality neonatal care while minimising risk to staff.
- Simulation can help address these challenges by promoting teamwork and testing logistics in novel situations.
Also published in Infant:
