

Practical considerations for the emergency delivery of babies from mothers with confirmed or suspected COVID-19
Maternity and neonatal departments must be prepared for the delivery of babies from COVID-19 positive women. We describe a guideline developed at the North Middlesex University Hospital maternity unit, for multidisciplinary team members attending an emergency caesarean section of mothers with confirmed or suspected COVID-19. Anticipated staff actions and personal protective equipment were considered to optimise staff safety and reduce transmission of SARS-CoV-2. We recommend units generate individualised guidance suitable to their settings.
Patricia Wells1
MBChB, MSc
Paediatric SHO
patricia.wells6@nhs.net
Amy Taylor1
MRCPCH, MBBS, MA
Paediatric Registrar
Cheryl Battersby2
PhD, FRCPCH
Honorary Consultant Neonatologist and Senior Clinical Lecturer in Neonatal Medicine
Cheentan Singh1
MD, FRCPCH
Consultant Neonatologist and Paediatrician
1North Middlesex University Hospital NHS Trust, London
2Faculty of Medicine, Imperial College London
The SARS-CoV-2 virus global outbreak has resulted in a significant challenge to healthcare systems globally. Clinical presentation ranges from asymptomatic to severe coronavirus disease 2019 (COVID-19) pneumonia, respiratory failure and death.1,2 More severe symptoms are widely described in those populations who have long-term conditions, are older and the immunocompromised.1,2 The morbidity in children and neonates is currently believed to be very minimal.3 Pregnancy alters the body’s immune system and it is known from experience with other viruses that this can result in more severe symptoms, particularly towards the end of pregnancy.4 As of the end of April 2020 the UK had 177,454 confirmed cases and 27,510 deaths.5 Over 700,000 births are recorded each year in the UK.6 It is likely that at least some of these deliveries will be affected by the SARS-CoV-2 virus.
Evidence relating to the effect of SARS-CoV-2 viral infection on the mother and fetus is currently evolving. In a recent rapid review by Mullins et al, of the 32 pregnant women affected with COVID-19, only two women (6%) required care in the intensive care unit; however, strikingly 47% (n=15) resulted in preterm delivery.7 The question of vertical transmission remains unanswered. Evidence is lacking and although in a small cohort the SARS-CoV-2 virus was not detected in amniotic fluid, cord blood, breast milk and neonatal throat swabs,8 there are some indications that vertical transmission may occur. In two separate reports from China, a total of three babies born to mothers affected by COVID-19 were found to have a raised SARS-CoV-2 IgM after delivery, despite a negative real-time reverse transcriptase-polymerase chain reaction (RT-PCR) nasal pharyngeal swab for SARS-CoV-2.9-11 Furthermore there are reports of neonates testing RT-PCR nasal pharyngeal swab positive for SARS-CoV-2 within a week of delivery.12
Maternity and neonatal departments must be prepared for the delivery of babies from COVID-19 positive women. Healthcare staff looking after such patients are at risk of contracting SARS-CoV-2. It is therefore vital that preparations include the planning and adoption of management steps to prevent transmission of virus to healthcare workers present at the delivery and, potentially, to the baby.
The transmission of SARS-CoV-2 is thought to occur largely via respiratory droplets generated by coughing or sneezing or through contact with a contaminated surface.13 The current guidance by Public Health England (PHE) indicates different personal protective equipment (PPE) should be worn by staff managing patients with suspected or confirmed COVID-19 in different settings (TABLE 1).14 Endotracheal intubation for general anaesthesia (GA) at an emergency caesarean section (CS) as well as intubation of the newborn and positive pressure ventilation are considered aerosol generating procedures (AGP) and carry a higher risk of transmission of infection (FIGURE 1).3,5,14
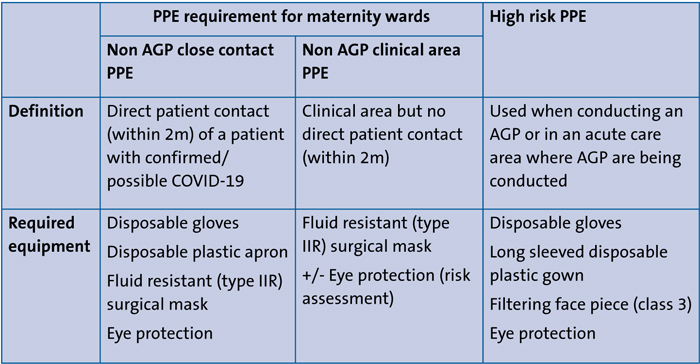
TABLE 1 Recommended PPE, adapted from advice by Public Health England.14,15
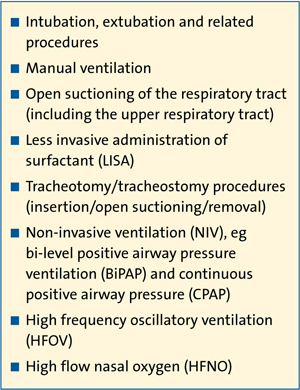
FIGURE 1 Aerosol generating procedures, compiled from RCPCH guidance.3
Intrapartum care and the safe delivery of babies involves multiple teams and a large number of personnel. Maintaining stringent infection control procedures in such emergencies, to protect staff and patients, is a logistical challenge that requires prior consideration to minimise exposure. In addition to appropriate PPE, it is also important for ‘contact’ and ‘non-contact’ members of staff to be identified. These non-contact team members are important to facilitate actions outside of the delivery room to minimise movement to and from the delivery room, and reduce risk of transmission.
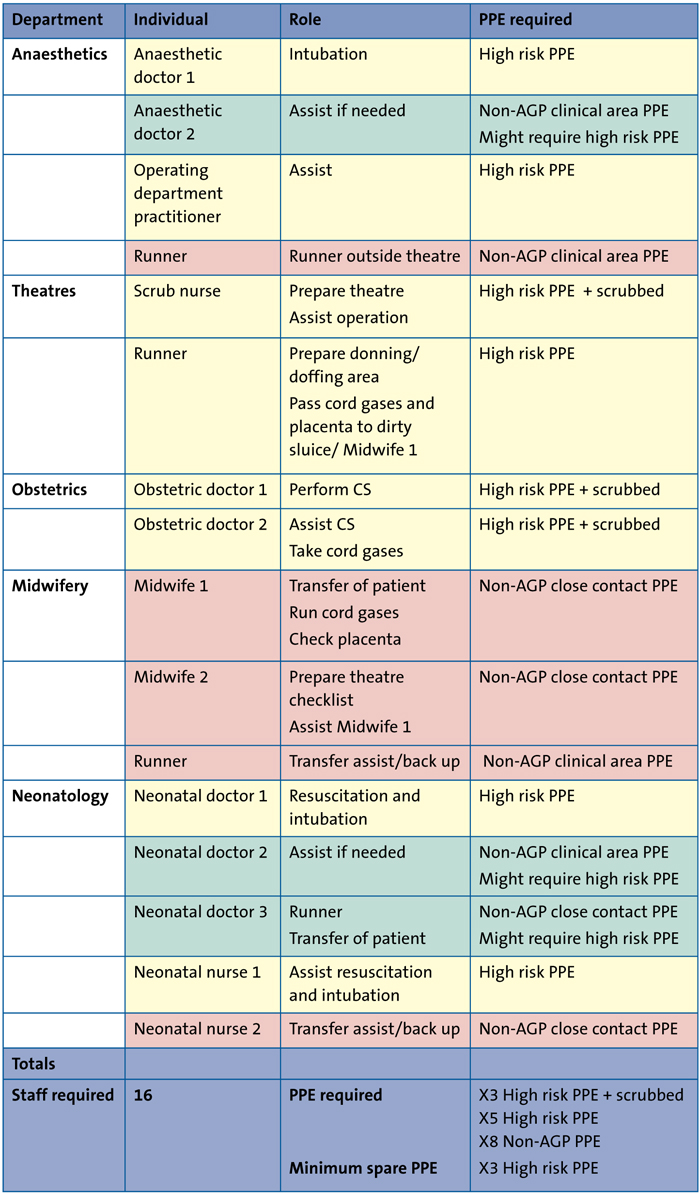
TABLE 2 Staff required for emergency CS alongside anticipated role and required PPE. Contact team members (shaded yellow ) are those present within theatre during a CS. Non-contact team members (shaded red) facilitate actions outside of the theatre. Other team members may be required to join the contact team where necessary (shaded green ).
Methods
The North Middlesex University Hospital recognised the need for a pathway for deliveries of COVID-19 positive mothers. We consulted the most up-to-date guidance published by PHE, the Royal College of Obstetricians and Gynaecologists (RCOG), the Royal College of Paediatrics and Child Health (RCPCH) and the British Association of Perinatal Medicine (BAPM).3,4,13,14 The guidance was applied to a draft practical pathway for emergency CS. Revisions were made following feedback from simulations with the multidisciplinary team and consultation with our local infection control team. Further modifications were incorporated as guidance from PHE, RCOG, RCPCH and BAPM evolved and subsequent statements were released by the UK Resuscitation Council.15
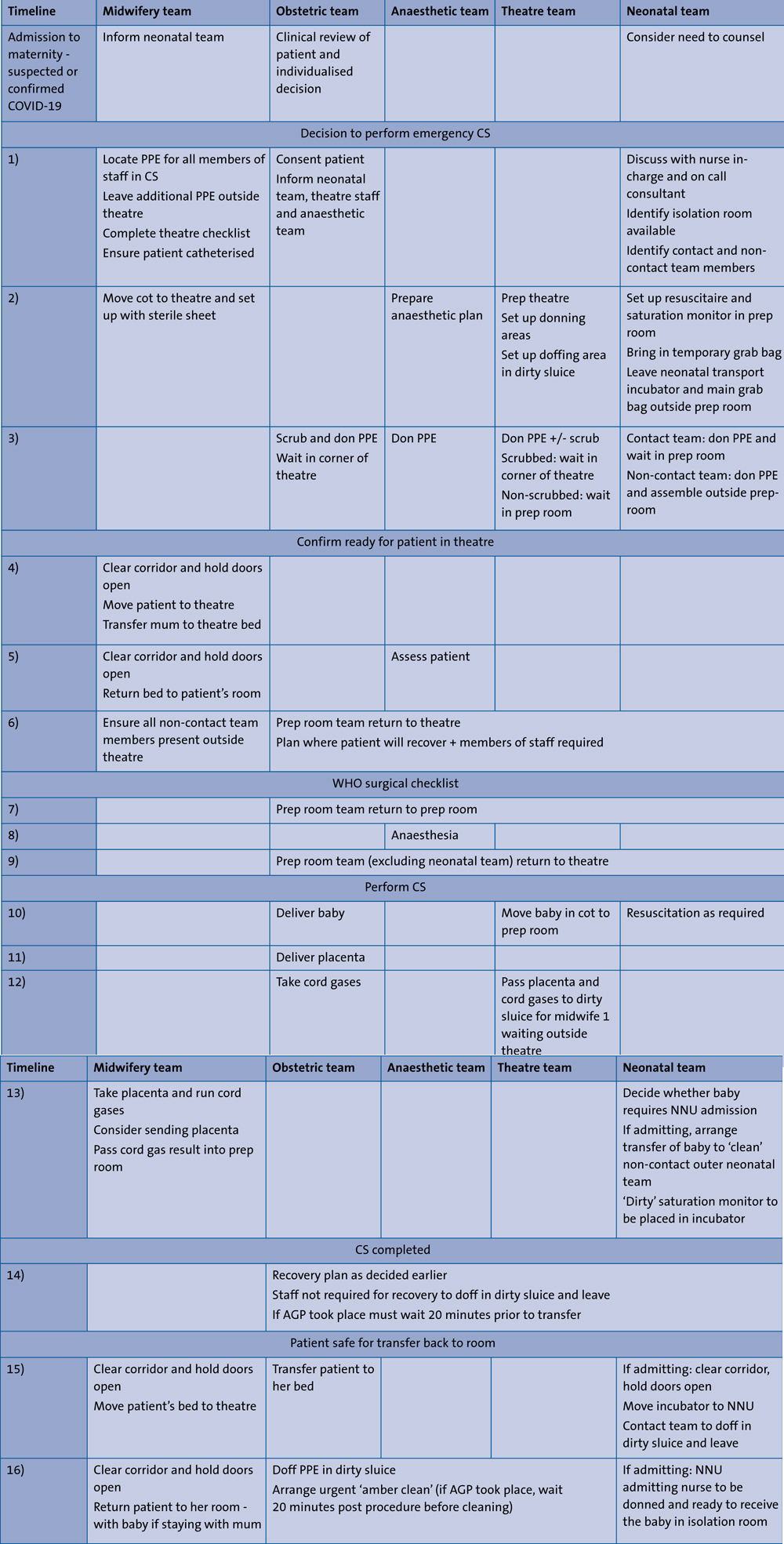
TABLE 3 Timeline of anticipated team movements and decisions during an emergency CS.
Practical guidance
The required personnel from five different teams and appropriate PPE for each member of the team were considered. The obstetric theatre layout was considered (FIGURE 2A). Neonatal resuscitation was designated to occur in a sideroom, termed the prep room. This was agreed so that staff exposure to AGP completed on the mother or the baby would be minimised. The PPE ‘donning’ area was designated as inside theatre or the prep room prior to patient arrival. The PPE ‘doffing’ area was identified as the dirty sluice, given it was an anteroom containing a sink.
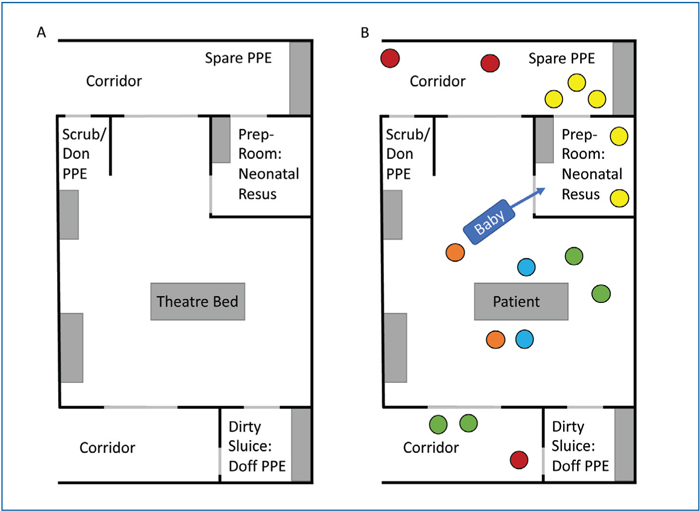
FIGURE 2 Theatre layout. A) Theatre layout and areas designated for donning PPE, doffing PPE, keeping spare PPE and neonatal resuscitation. B) Demonstration of team positions during emergency CS prior to delivery of baby. Key: red=midwifery, yellow=neonatology, green=anaesthetics, blue=obstetrics, orange=theatre staff.
The emergency CS was divided into 16 key steps and key roles of team members were identified. High risk PPE and infection control measures are crucial and anticipated staff actions and location were designated to help minimise transmission (FIGURE 2B, TABLES 2 and 3). Individual emergency cards were produced for each staff member involved, documenting their responsibilities, considerations and anticipated PPE (FIGURE 3).
Similar guidance was generated for CS under spinal anaesthetic and vaginal delivery requiring neonatal presence (available on request from the authors). Neonatal resuscitation and commonly used interventions such as suction, and endotracheal intubation are considered AGPs (FIGURE 1). Although evidence for vertical transmission is not currently conclusive, the recommendation is that the neonatal team should wear AGP PPE during neonatal resuscitation, or if within 2m of neonatal resuscitation to optimise staff safety and minimise interruption to the resuscitation.3,15
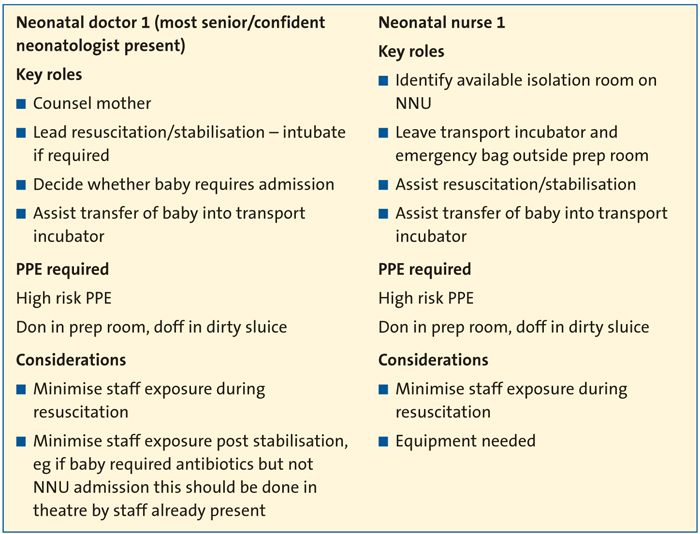
FIGURE 3 An example of emergency personnel briefing cards.
Conclusion
Maternity areas have a high flow of patients and more mothers with COVID-19 should be anticipated in light of the ongoing pandemic. Multiple professionals from various teams are involved in the safe delivery of babies from pregnant mothers. An emergency CS is a high intensity event with multiple clinical and practical considerations for reducing transmission of SARS-CoV-2, for patient and staff. This guidance was generated to provide a clear framework for multidisciplinary team members and has been useful at the North Middlesex University Hospital maternity unit. The authors recommend that all units should develop their own individualised guidance based on theatre and building layout, staffing, skill mix and PPE availability. The areas to be used for donning and doffing of PPE, neonatal resuscitation, and the number of staff required should be planned prior to the event. Simulations of different scenarios is crucial in ensuring local logistics are considered and to familiarise staff with additional PPE considerations.
Contributions and conflict of interest
PW, AT, CS: involved in development and implementation of guideline at North Middlesex University Hospital.
CB: critical review of article.
No conflicts of interest to declare.
Or read this article in our
Tablet/iPad edition
- Healthcare staff must be prepared for the delivery of babies from COVID-19 positive women.
- Preparations should include planning of logistical steps to prevent transmission of the virus.
Also published in Infant:
