

Achieving oxygen saturation targets in preterm infants at birth: does using an SpO2 target range help?
Neonatal resuscitation guidelines vary in their recommendations for oxygen saturation (SpO2) targets – some use a single SpO2 target, others use a target range. We conducted a prospective observational study collecting SpO2 data on preterm infants born at <34 weeks’ gestation. The objective of our study was to determine if using a range, rather than a single SpO2 target, would be more achievable during preterm infant resuscitation
Prakash Kannan Loganathan1,2,3
Consultant Neonatologist
pkannanloganathan@nhs.net
Paediatric Trainee
Vrinda Nair 1,2
Consultant Neonatologist
Difu Shi3,4
Postdoctoral Fellow in Data Science and Computational Cosmology
Carlton Baugh3,4
Professor in Data Science and Computational Cosmology
1Neonatal Unit, James Cook University Hospital, Middlesbrough
2Clinical Academic office, Faculty of Medical Sciences, Newcastle University
3Department of Physics, University of Durham
4Institute for Computational Cosmology, University of Durham
Loganathan PK., Bearn A., Nair V., Shi D., Baugh C. Achieving oxygen saturation targets in preterm infants at birth: does using an SpO2 target range help? Infant 2023; 19(6): 227-30.
Oxygen supplementation is often needed for preterm infants to maintain target oxygen saturation (SpO2) levels at the time of birth. In the UK, Resuscitation Council UK Newborn Life Support (NLS), recommends targeting a single SpO2 value (the 25th centile) for newborn resuscitation.1 On the other hand, the European Resuscitation Council, American Heart Association Neonatal Resuscitation Programme (NRP) and the Australian and New Zealand Resuscitation Council guidelines recommend a range of SpO2 values after birth.2-4 For example, NLS recommends targeting SpO2 of 85% at five minutes and NRP recommends targeting SpO2 between 80-85% at five minutes.
We suspect that following a SpO2 range would be easier and more achievable than targeting a single value of SpO2. There is also the possibility that targeting a single SpO2 target could lead to the inadvertent administration of excessive oxygen. For example, a preterm infant with SpO2 of 81% at five minutes is likely to receive more oxygen as they have not met the NLS SpO2 target of 85%. This would be avoided if we followed a recommended target range of SpO2 of 80-85%.
Recently, most resuscitation councils recommended the use of starting oxygen at levels from 21% to 30% for initial resuscitation of preterm infants at birth.1,2 The objective of our study was to find out whether using a target range (NRP) rather than a single SpO2 target (NLS) would help in better achieving SpO2 targets. We also report on the proportion of preterm infants (born at <34 weeks’ gestation) with recorded SpO2 below, above and within the target range during their first 10 minutes of life.
Methods
We conducted a prospective study over a period of 14 months (November 2019 to December 2020) in a single-centre neonatal intensive care unit. We did not recruit preterm infants with an antenatal diagnosis of major chromosomal or congenital abnormality. We followed the UK NLS manual for all newborn resuscitations and used starting oxygen from 21% to 30% titrated upwards to reach the oxygen saturation target.1 At the time of this study, delayed cord clamping was not routinely practiced in our unit. We used a T-piece resuscitator (Draeger Resuscitaire) to provide positive pressure breaths. In our setup, each of our delivery rooms are equipped with standard pulse oximeters, however, whenever possible, the attending neonatal team used the study pulse oximeter if the birth gestational age was <34 weeks. For our study, we used the Masimo Rad-97 pulse oximeter, chosen because of its resistance to movement artefacts and good performance in states of low perfusion.5,6 The pulse oximeter was set to normal sensitivity with two-second averaging times. All the pulse oximeter data were downloaded every two seconds directly into an Excel/CSV file. All demographic and resuscitation details were collected from the neonatal database. With limited documentation and dynamic changes, we could not collect information regarding oxygen supplementation.
With the prospective audit, we did not calculate a sample size and we continued recruitment until we reached a convenient sample of 50 preterm infants with at least 50% of the data from extreme preterm infants (ie birth gestational age of ≤27 weeks). We used descriptive statistics for population characteristics. Categorical variables were presented as proportions. Numerical variables were presented as a mean with standard deviation (SD) or as a median with interquartile range (IQR), as appropriate. Parametric and non-parametric statistical tests were applied based on the data distribution. Statistical analysis was performed using IBM SPSS Statistics (version 27; IBM Corp., Armonk, New York) and the figures were created using Python 3.6.9. This study was registered and approved by our local hospital audit department. As the study involved only data collection, we did not obtain ethics approval and informed consent. We used the Strengthening the Reporting of Observational Studies in Epidemiology statement (STROBE) guidelines for reporting of the study.7
Results
During the study period, there were a total of 5,426 deliveries with 270 babies born at <34 weeks’ gestation. Based on the availability of the attending neonatal team using the study pulse oximeter and excluding poor quality data (n=4), we obtained data for a total of 50 infants for our final analysis (18.5%). The cohort demographics were:
- mean birth gestational age = 28 ±3.2 weeks
- 25 infants (50%) were of gestational age <27 weeks
- 27 (54%) infants were male
- 36 (72%) infants were born by caesarean section
- the median Apgar scores were 9 (IQR=5-7) and 9 (IQR=7-9) at one and five minutes, respectively
- 46 infants (92%) received some form of resuscitation and 20 infants (40%) were intubated at delivery.
Oxygen saturations
Only 19 (38%) infants achieved SpO2 of 85% at five minutes and 30 (60%) infants achieved SpO2 of 90% at 10 minutes. The median time to reach SpO2 of 85% was 5.24 minutes (IQR=3.42-5.72); SpO2 of 90% was 6.06 minutes (IQR=4.28-8.03), and heart rate >100 beats/min was 1.46 minutes (IQR=0.14-3.56).
The median SpO2 at five minutes was 81% (IQR=68-90) and at 10 minutes 91% (IQR=84-94) (FIGURE 1). There is no dependence of the SpO2 on the sex of the infant or mode of delivery for those who achieved 85% SpO2 at five minutes and 90% SpO2 at 10 minutes, compared with infants who did not achieve these target saturations.
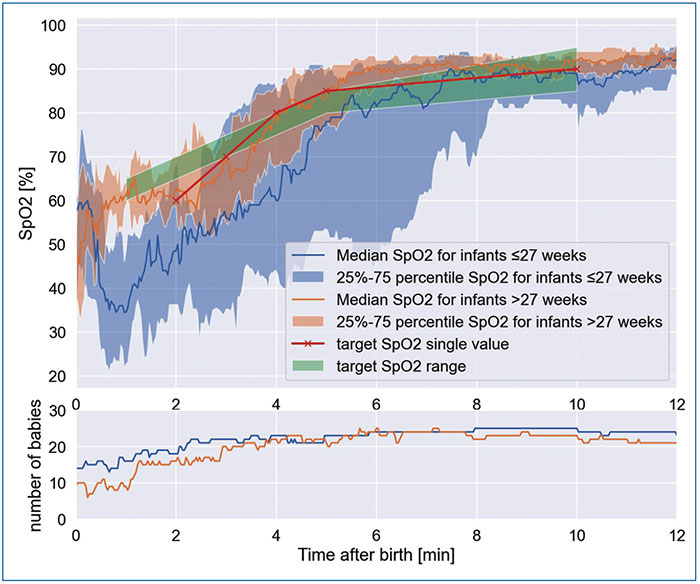
FIGURE 1 The achieved median SpO2 with 25-75th percentiles in the first 10 minutes of life.
Median heart rates during the first 10 minutes of life are provided in FIGURE 2. The number of preterm infants within, below and above the target SpO2 (as per NLS) and target SpO2 range (as per NRP) during the first 10 minutes of life can be seen in TABLE 1. As there were large amounts of missing data (>50%), we did not report the numbers during the first minute of life. There is no statistical difference in infants achieving the target using the NLS SpO2 single target compared with the NRP SpO2 range, except at 10 minutes where a higher proportion of infants achieved the SpO2 target using the NRP range (odds ratio=11.67; 95% confidence interval: 3.19 to 42.69; p≤0.001).
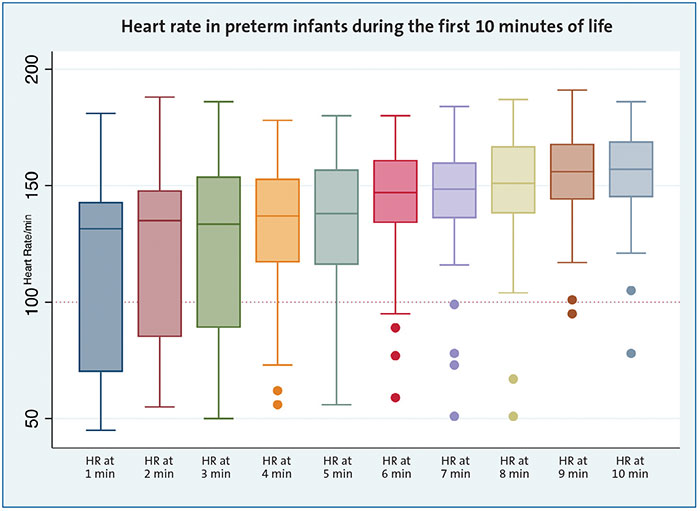
FIGURE 2 A boxplot of heart rate (HR) for the first 10 minutes of life.
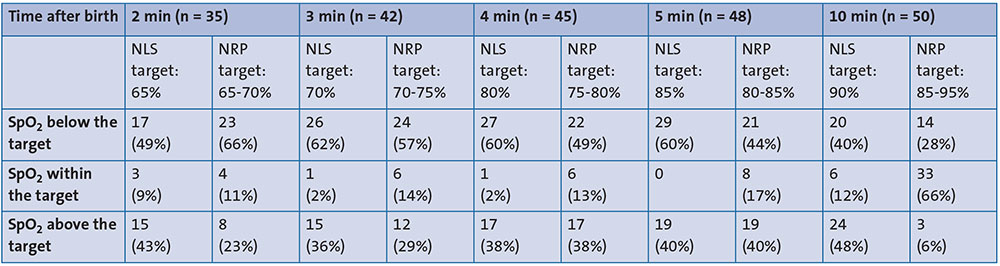
TABLE 1 The number of preterm infants with SpO2 above, below and within target.
Discussion
In our study, we have reported the achieved SpO2 and heart rate data for preterm infants during the first 10 minutes of life using both the single SpO2 target value (NLS) and the SpO2 target range (NRP). In our set-up, each of our delivery rooms is equipped with standard pulse oximeters (data not used for the study) and the neonatal team would normally use these devices as a default over the study pulse oximeter. The team was able to use the study pulse oximeter only if there was enough time to set up the device and this explains the reason for the large amount of excluded data.
Most infants achieve target SpO2 levels after five minutes, probably due to the many interventions and the technical limitations of pulse oximetery. Pulse oximetry takes a median time of 90 seconds to display valid data.1 Until then, there is no guide for oxygen titration. Initial resuscitation interventions need to clear the lung fluids and aerate the lungs, which happens during the first few minutes of life. Resuscitation Council UK recommends starting with minimal oxygen to avoid hyperoxia; hypoxia could be the countereffect of reducing hyperoxia.1 Moreover, most resuscitation interventions such as mask adjustment, suctioning and endotracheal tube placement, are likely to happen during the first five minutes after birth; this could increase the time taken to achieve target SpO2 levels. Similar results have been reported in other studies.8,9
The current recommended oxygen saturation percentile charts were created using data that included relatively healthy infants who did not require any resuscitation (56.5%), term infants (37%) and a small proportion of preterm infants born at <32 weeks’ gestation (4.7%).10 Use of automated oxygen control during preterm resuscitation11 and use of graphical display of the target real time SpO2 data, could potentially help in achieving the SpO2 targets.12 An unanswered question in this area is whether targeting a higher oxygen saturation percentile (>25th percentile) would achieve a better outcome.
Our study has some noteworthy strengths in that we collected data prospectively with direct downloading of data from the pulse oximeter and 50% of the data are from extreme preterm infants. However, we did not collect information on the amount of oxygen given and the titration strategy and although we collected details on resuscitative measures, we do not have timelines of interventions and their relationships with SpO2. Nevertheless, all members of the clinical team attending resuscitations are NLS trained and are expected to follow the algorithm without major variation in interventions.
We collected heart rate data for the first 10 minutes of life in 50 preterm infants. A study by Dawson et al provided data on the normal range of heart rate during the first minutes of life.13 In the Dawson study there were 160 preterm infants of <37 weeks’ gestation and none received any medical interventions at resuscitation. In our study, all of the infants were <34 weeks’ gestation and received some form of medical intervention.
From our study, we conclude that a significant proportion of preterm infants did not reach SpO2 targets during the first 10 minutes of life irrespective of using the currently recommended SpO2 targets (NLS) or a target range (NRP).
Conclusion
In our study, only a proportion of preterm infants achieved recommended SpO2 targets, with more infants achieving target SpO2 at 10 minutes than at five minutes after birth. In conclusion, the use of an SpO2 target range does not help to achieve an oxygen saturation target at birth, compared to use of a single value SpO2.
Acknowledgement
The authors would like to thank all the staff and parents from the neonatal unit at James Cook University Hospital and also Hugh Hanchard, Librarian, for his help with English language formatting and reviewing the manuscript.
Statement of ethics, author contributions and data availability
This study was registered as an audit and the protocol was approved by James Cook University Hospital, South Tees NHS Foundation Trust. As an audit, no written informed consent was obtained from the participants.
PL was responsible for concept, design, data collection, interpretation of data, drafting the initial manuscript and approving the final manuscript. AB was responsible for data collection, inter-pretation of data and approval of the final manuscript. VN was responsible for design, interpretation of data and approval of the final manuscript. DS was responsible for design, interpretation of data, data analysis and approval of the final manuscript. CB was responsible for design, interpretation of data, data analysis and approval of the final manuscript.
The data are available to researchers who provide a methodologically sound proposal and research ethics board approval. Proposals should be submitted to pkannanloganathan@nhs.net
Or read this article in our
Tablet/iPad edition
- We collected SpO2 and heart rate data for the first 10 minutes of life in 50 preterm infants.
- Irrespective of using an SpO2 target range or a single SpO2 target, only a proportion of preterm infants achieve target SpO2 during the first 10 minutes of life.
Also published in Infant:
