

Is surfactant administration via a supraglottic airway device as effective and safe as via a thin catheter in the trachea?
Less invasive techniques for surfactant administration in preterm infants are known to reduce the need for mechanical ventilation, decrease the risk of bronchopulmonary dysplasia and improve outcomes for preterm infants. This study compares two methods of surfactant administration performed in a non-tertiary neonatal unit: surfactant administration via a supraglottic airway device and administration into the trachea via a thin catheter.
Adewale Owa
Specialty Doctor
adewale.owa@nhs.net
Olushola Tedimola
Specialty Doctor
Pauline Adiotomre
Consultant
Omobolaji Wilson
Consultant
Vijaya Hebbar
Consultant
Less invasive surfactant administration (LISA) has become a widely popular and effective way of administering surfactant to preterm babies with respiratory distress syndrome (RDS). It is well known and accepted that it reduces the need for mechanical ventilation and its associated risks in preterm babies.1-3
A few methods of LISA have been practised successfully in different locations worldwide and described in the literature. These techniques include:4
- surfactant administration via a thin catheter directly into the trachea
- surfactant administration through a supraglottic airway device
- aerosolised surfactant administration
- pharyngeal surfactant administration.
The most common of these methods is surfactant administration into the trachea using a fine catheter. Two of these methods of less invasive surfactant administration are practised routinely at our centre, namely:
1. Surfactant administration using a thin catheter – we have used the Chiesi LISACath (no longer available) and the Vygon Surfcath on our unit (FIGURE 1).
2. Surfactant administration through a supraglottic airway device (the i-gel supraglottic airway from Intersurgical, www.intersurgical.com/info/igel (FIGURE 1).

FIGURE 1 The Surfcath (Vygon) and the i-gel supraglottic airway device (Intersurgical).
Audits of these two methods have been carried out, each over a two-year period.
The aim of this study was to compare the outcome of the results obtained using these two methods of surfactant administration. To the best of our knowledge, this is the first study from a non-tertiary neonatal unit in the UK to compare both methods.
Methodology
LISA was introduced on our level 2 neonatal unit at Diana Princess of Wales Hospital, Grimsby, in January 2019. The first method introduced was surfactant administration into the trachea using a thin catheter. Staff training and awareness was carried out for medical and nursing staff before the introduction of this procedure. A guideline was developed, which included an audit form. Data were collected prospectively using this audit form.
Inclusion criteria for surfactant administration using a catheter included babies with surfactant deficiency, born at gestational age of 27 weeks and above if they were singletons or 28 weeks and above for multiple births, who did not require invasive ventilation or transfer to the tertiary centre and babies requiring ≥30% oxygen while on continuous positive airway pressure (CPAP) or nasal high flow therapy with increased work of breathing.
Exclusion criteria included babies who needed ventilation due to significant respiratory failure suggested by fractional inspired oxygen (FiO2) above 60%, capillary blood pH <7.2, significant apnoea/bradycardia or desaturations. Babies with meconium aspiration syndrome, significant pneumothorax and/or persistent pulmonary hypertension of the newborn were excluded.
All babies who met the inclusion criteria and who received surfactant administration using a catheter from January 2019 to December 2020 were included in this study.
The procedure for surfactant adminis-tration through the i-gel supraglottic airway device was introduced on the unit in March 2021 following staff training and awareness (FIGURE 2). A guideline for the administration of surfactant via i-gel was developed prior to the introduction of this procedure based on the NHS Greater Glasgow and Clyde (NHSGGC) Surfactant Administration via Laryngeal Mask Airway Standard Operating Procedure.5 A full description of the procedure is available on NHSGGC guidelines website and is not repeated here.5 Data were collected prospectively using an audit form.

FIGURE 2 The i-gel procedure in a manikin for staff training.
Inclusion criteria for surfactant administration via i-gel included babies with birth weight ≥1,200g, gestational age ≥28 weeks, RDS confirmed on chest X-ray, sustained FiO2 of ≥30% on CPAP and clinical signs of RDS.
Exclusion criteria included previous intubation, imminent intubation, large pneumothorax, previous failed attempts at i-gel surfactant administration, major congenital abnormalities (eg maxillofacial, tracheal or known pulmonary malfor-mations and confirmed or suspected congenital cardiac disease).
All babies who met the inclusion criteria and who had surfactant administration via i-gel from March 2021 to February 2023 were included in this study.
Both procedures were performed by middle grade doctors (with or without supervision, depending on their skills and confidence) and by consultants. A procedure of surfactant administration using a catheter was defined as being successful if there was evidence of improvement in the baby’s respiration, reduced oxygen requirement, visualisation of the surfactant being administered into the airway (if a video laryngoscope was used) and no documented aspiration of surfactant from the baby’s stomach.
A procedure of surfactant administration via i-gel was defined as being successful if less than 50% of given surfactant was aspirated from the stomach and if there was an improvement in the baby’s clinical condition, including reduction in oxygen requirements.
The success rates for both procedures were compared. The characteristics of babies in each group were compared and so were the number of babies needing mechanical ventilation after either procedure. Complications during and after either procedure, if any, were recorded and compared.
Results
The outcome of the prospective data collection following surfactant adminis-tration using a catheter from January 2019 to December 2020 was compared to that of surfactant administration via i-gel from March 2021 to February 2023.
Characteristics of the groups
A total of 39 babies had surfactant administration using a thin catheter with a total of 46 procedures, while 31 babies had surfactant administration via i-gel with a total of 36 procedures. Seven babies required a repeat dose of surfactant in the thin catheter group whereas five babies had a repeat dose of surfactant via i-gel. The dose of surfactant given was based on body weight and was similar in both groups, as per the unit protocol.
There were 29 males and 10 females in the thin catheter group, while there were 19 males and 12 females in the i-gel group, however this difference in gender was not statistically significant. Furthermore, both groups were similar in terms of gestational age, birth weight, age at first dose of surfactant and oxygen requirements before surfactant administration (TABLE 1).
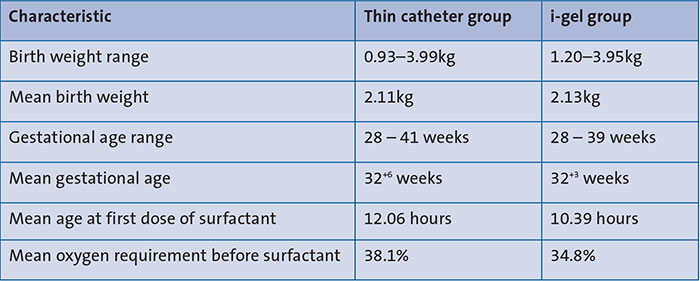
TABLE 1 Baseline characteristics.
Success rate of procedures
In the catheter group, 39 out of the 46 procedures were successful, giving a success rate of 84.8%, whereas in the i-gel group, there were 32 successful procedures out of the 36 with a success rate of 88.9%. The relative risk of a failed procedure in the catheter group when compared to the i-gel group was 1.37 (95% CI 0.43-4.32), although this was not statistically significant.
Complications
A comparison of the complications of the two procedures can be seen in TABLE 2. Desaturation occurred more frequently in the catheter group than the i-gel group. One baby in the i-gel group experienced apnoea; two babies in the catheter group experienced pneumothorax.
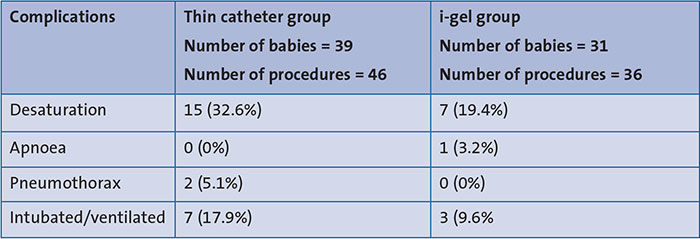
TABLE 2 Complications of the procedures.
Six babies in the catheter group required intubation and ventilation and one required INSURE (INtubation, SURfactant administration and Extubation) (17.9%) whereas three babies (9.6%) needed intubation and ventilation in the i-gel group. The percentage of babies that required intubation and ventilation in the catheter group was higher than in the i-gel group although this was not statistically significant (odds ratio = 1.97; 95% CI 0.47-8.25).
Discussion
For newborns with RDS requiring surfactant therapy, LISA via a fine catheter in the trachea reduces the need for mechanical ventilation and the risks associated with fragile lungs. 6,7 LISA is also associated with improved outcomes for preterm infants, and reduced risks of bronchopulmonary dysplasia (BPD) and intracranial haemorrhage. 6,7 Current European guidelines recommend LISA as the preferred mode of surfactant administration for spontaneously breathing babies on CPAP, if clinicians are experienced with this technique.8
Research into less invasive methods for surfactant administration begun in the eighties and early nineties. In 1992, there were two published reports on two methods: a report describing surfactant administration via intratracheal catheter by Verder et al9 and another that described surfactant administration through a laryngeal mask (Eschen et al).10 Since then, a lot of interest has been generated in finding less invasive methods of administering surfactant to spontaneously-breathing babies and avoiding the need for mechanical ventilation.
Initially, the uptake of LISA appeared low in neonatal units across the UK compared to European countries.11,12 However, more recent evidence suggests that uptake is increasing.13-18 LISA was introduced on our level 2 neonatal unit in January 2019 and our practice has continued to develop and evolve over the years. Initially we introduced the fine catheter in the trachea technique and more recently (March 2021) the i-gel supraglottic airway device.
We carried out a total of 46 LISA procedures by thin catheter over a two-year period, our numbers being relatively higher than those reported from other centres within the UK.13,14 The success rate of LISA through a thin catheter from our centre was 84.8% and this can be attributed to guideline development, staff training and awareness, which was carried out for medical and nursing staff before the introduction of the procedure on our unit. This success rate is comparable with that obtained from other units in the UK and Germany13,15,19 and higher than that reported by another unit in the UK14 and one from Hungary,20 although the cohort in Hungary consisted of babies born at relatively younger gestational ages.
Over a two-year period, we performed a total of 36 LISA procedures via i-gel with a success rate of 88.9%. Similar to the LISA by thin catheter procedure, our success rate can be attributed to guideline development, staff training and awareness before the introduction of the procedure. LISA by supraglottic airway devices such as the i-gel device, has been reported to be beneficial in the management of RDS in newborn babies.21-29 However, there is a paucity of data on surfactant administration via i-gel from the UK. Furthermore, most of the reports available elsewhere have been mainly from tertiary centres.21 LISA by supraglottic airway devices such as i-gel avoids the need for laryngoscopy and is relatively easier to perform.5,23 It has been proposed as a viable method for managing RDS that can be applied in low and middle-income countries.24,29
We have demonstrated successful outcomes from both methods of LISA from our centre, which can be replicated in other centres with adequate training. Few complications including desaturation, apnoea and pneumothorax were found in our cohort of patients. We found a better success rate and less complications in the i-gel group than in the thin catheter group. More babies in the thin catheter group ended up requiring mechanical ventilation than in the i-gel group, although these differences were not statistically significant.
Limitations
Our study is limited by the small sample sizes in the two comparison groups. Although we have compared two different procedures, this is not a randomised control trial and the data for the two groups were collected at different times.
Conclusion
We compared two methods of LISA practised at our centre. The results from our study show that surfactant administration via the i-gel supraglottic airway device is as effective and safe as surfactant via a fine catheter into the trachea. There was a better success rate and less complications from surfactant administration via i-gel than surfactant administration via the catheter, although this was not statistically significant.
Acknowledgement
The authors extend their gratitude to all the medical and nursing staff on the Neonatal Ward, Diana Princess of Wales Hospital, Grimsby, who have performed or assisted with the procedures and who have taken part in data collection for this study.
Or read this article in our
Tablet/iPad edition
- With proper training, less invasive surfactant administration through supraglottic airway devices can be performed successfully in non-tertiary neonatal units.
- Surfactant administration via the i-gel supraglottic airway device is as effective and safe as surfactant administration via a thin catheter in the trachea with a trend towards better success rate and fewer complications.
Also published in Infant:
