

Delivering NIPE screening: the application of human factor and quality improvement tools
The project analyses the delivery of the newborn and infant physical examination (NIPE). It aims to identify weaknesses in service delivery contributing to the human factor incidents and increased demands on the junior doctor, and to redesign the system to reduce risk, improve efficiency and reinforce resilience.
Samyar Siadati
Paediatric Specialty Trainee Doctor
Neonatal Unit, Watford General Hospital, West Hertfordshire Teaching Hospitals
NHS Trust
Claudia Chetcuti Ganado
Neonatal Consultant
Neonatal Unit, Luton and Dunstable Hospital, Bedfordshire Hospitals NHS Foundation Trust
claudia.chetcutiganado@ldh.nhs.uk
Background
The newborn and infant physical examination (NIPE) screening programme is a UK wide screening examination commissioned by NHS England (NHSE).1 The aim of the examination is to ensure timely detection of infant conditions that are time-critical, where missed opportunities lead to significant morbidity and mortality. The screening standards state that the examination should be undertaken within 72 hours of birth for all UK live births above 34 weeks’ gestation. For infants born prematurely, the screening examination should be undertaken at 34 weeks of corrected gestational age.
After 2017 NHSE introduced the NIPE S4N, a web-based system that can capture all livebirths and monitor adherence to the NIPE screening standards. Quarterly reports are generated through the system and trusts are required to provide assurance. Failure to meet the standards is considered a screening incident and reportable to NHSE.
The Luton and Dunstable University Hospital has a level 3 neonatal unit and maternity service with approximately 5,000 births annually. The NIPE examination is performed by junior paediatric trainees. Junior trainees on a daytime shift are allocated to undertake all NIPE examinations on the postnatal ward for births within the previous 72 hours. Mother/infant pairs are admitted to the postnatal wards from delivery suite and timely discharge is necessary for this flow to be maintained. Delays at the postnatal ward impact delivery suite capacity. Within the postnatal ward, the mother is cared for by obstetricians and the midwifery team while care of the baby is the remit of the neonatal nursing and paediatric teams, thus creating an inherent risk of ‘boundary weakness’.
Trainees allocated to postnatal ward shifts often left work two hours later than scheduled, creating the need to lengthen the daytime shift of junior trainees and employ an extra person on the weekends. Through a quality improvement initiative, the neonatal team introduced a mid-shift huddle aiming to monitor workload daily and reallocate resources to provide some help to the postnatal ward junior doctor.
The introduction of the NIPE S4N within our team highlighted significant weaknesses and this led to the need for a failsafe team to ensure we were meeting the NIPE standards.
Despite our failsafe processes and revising the rota, we continue to struggle to meet demand and often need additional junior doctors to manage the workload. We continue to see screening incidents ranging from a whole examination being missed to those where referrals are not processed or followed through. There continues to be a time lag between incidents happening and the failsafe picking it up, which poses risk. The types of incidents reported or picked up by the failsafe processes are reported in TABLE 1.
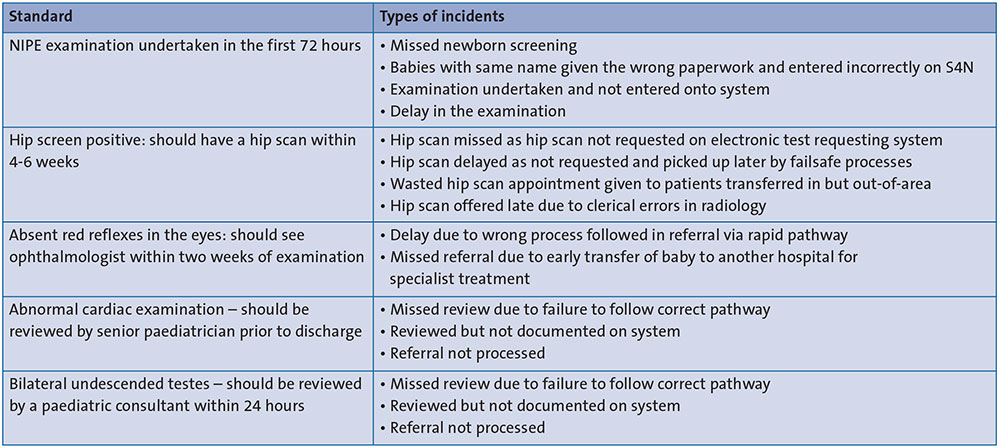
TABLE 1 Types of incidents in the NIPE processes highlighted by the failsafe monthly reports generated at departmental level.
This assessment follows the toolkit developed by Ward et al (2010)2 as it was specifically designed and evaluated for a healthcare context. We used a combination of human factors and quality improvement tools including the CARe resilience model as this can be extremely powerful for improvements in health care.3,4
System analysis
System mapping
To understand the work system for undertaking the NIPE examination we undertook a SEIPS system analysis, which is very effective at highlighting the interaction of the various people within a task/environment/resources/organisation in a healthcare-specific framework.5-7 The SEIPS analysis identified the junior doctor as central to the task, which led to focussing a risk analysis around the task and interactions of the junior doctor.
Hazard identification
We used SWIFT (Structured What If Technique) and STAMP (Systems-Theoretic Accident Model and Processes) hazard analysis techniques to help highlight what could go wrong and risk severity.8 The use of STAMP was effective in looking at the hierarchy of controls that can be put in place to act as a failsafe. Through our observation and system analysis we identified barriers and facilitators that could be eliminated or adopted to further strengthen our recommedations. For example, a consultant’s approachability can be a barrier if the consultant only goes to help when specifically asked but a compassionate consultant that assists with the workload is a facilitator.
The STAMP analysis highlighted weakness within our control loops, particularly the lack of a dedicated failsafe team and the time lag for failsafe processes. It identified the need for a real time failsafe process to pick up human factor cognitive challenges that could be reduced.
Understanding demand capacity mismatch
We used observation to complement our analysis and to understand ‘work as done’ using guidance from the NHSE Brief Guide to Conducting Observations.9 Part of this was timing the process for undertaking the task from start to finish observing four different junior doctors.
We formulated a questionnaire based on understanding how the day-to-day operation influenced completion of the task. The questionnaire explored the task, equipment, environment, information flow and impact on cognitive functioning. The findings from this survey are depicted in FIGURE 1.
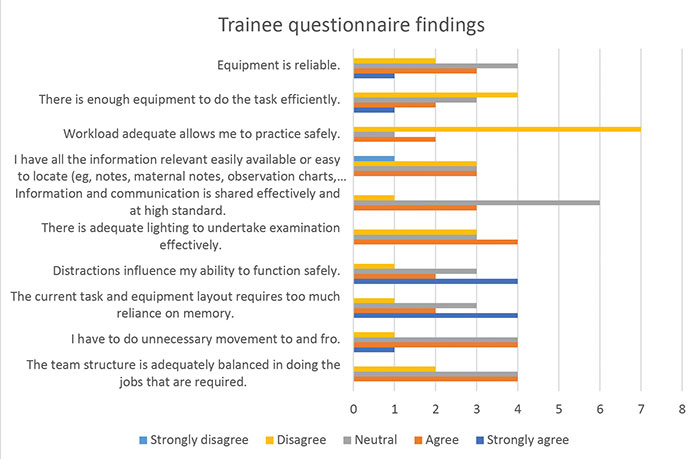
FIGURE 1 Results of a questionnaire survey of junior doctors undertaking the NIPE examination as part of their job role (n=11).
The observation helped to understand the trade-offs performed by trainees daily. Considerable time was spent travelling to and from the nursery as the workstation was in the nursery and the hospital policies dictated that the baby needed to be examined at the bedside. Although there was a printer in the nursery, the computer was connected to an adjacent room printer. When other trainees were available to support high workload, the presence of only one computer meant that the trainees had to wait their turn to be able to use the computer. The trainee had to log in separately to the S4N and the electronic test requesting system, which further reduced productivity. On occasion, the trainee used the log in of the previous trainee to save on time, which can introduce significant medicolegal risk.
As can be observed from the timed process map, the time from start to finish can vary between 10.5 to 54 minutes with a mean of 32.3 minutes (FIGURE 2).

FIGURE 2 Timed observation of four trainees undertaking the task from start to finish.
On average there are 15 examinations per day, which would require a mean of 8.1 hours. This depicts a significant demand/capacity mismatch. The doctor’s duties span more than just NIPE examinations, yet the time taken to go to and from the nursery to the bedside once can take up two hours of the working day. The time to perform the examination ranges from 4.9 minutes to 11.3 minutes.
If the baby is undressed and dressed by another team member while the doctor is gathering information and entering the documentation, we hypothesise that the time to undertake the examination will be reduced by half from a mean of 8.1 minutes to 4.05 minutes thus effectively saving another 60 minutes.
During busy times we noted established medical staff requesting the help of the neonatal nurse. The nurse undressed the baby while the doctor was gathering information and dressed the baby while the doctor documented the findings and made a plan. We observed that three neonatal nurses were on shift at any time who could be used more effectively. The examination can be delayed attempting manoeuvres to get the baby to open his/her eyes. Trainees needed the neonatal nurse to hold the baby’s eyes open. When senior and established staff were on shift, they had no problem getting one of the neonatal nurses to support in this way but more junior and temporary staff did not feel empowered to do so. There is no clear standard operating policy around the role of the neonatal nurse. We feel that suppor-ting this adaptation by including the neonatal nurse to support in the process, will significantly reduce the misalignment between demand and capacity and may eliminate the need to employ the neonatal doctor on a longer shift.10-12 Early discharge of patients will improve flow and capacity and will impact safety by reducing the cognitive workload on the neonatal doctor.13,14 The questionnaire highlighted that eight out of 11 trainees felt the work-load was not conducive to safe practice.
It is evident from the timed process map that a large amount of time is spent obtaining the information and walking to the nursery. Often this is because information and equipment are misplaced, out of battery or being used by someone else. The positioning of the tools did not support the policy of examining the baby at the maternal bedside. Examining the baby and then walking to the workstation with the possibility of interruption adds to the cognitive workload and may impact on safety. Alternating between tasks while waiting for the availability of the computer further increases the likelihood of error.13,14 Most neonatal doctors indicated that there is not enough equipment to do the job efficiently and the current task and equipment layout requires too much reliance on memory (FIGURE 1).
How can the work system be modified to reduce risk or improve performance?
We used the adapted HFIX (Human Factors Intervention Matrix) to make recommendations for the whole of the work system.15 This looks at areas for improvement that can be modified to reduce risk or improve performance at the level of:
- individuals
- tasks
- tools and technology
- internal environment
- organisation
- external environment.
Our analysis yielded 13 recommendations, which can be seen in TABLE 2. Our recommendations detail ways of anticipating, responding to, monitoring, co-ordinating and learning.3 Our recommendations all scored highly for feasibility, acceptability, cost effectiveness and potential to be sustained. The biggest feasibility challenge is recommendation 13, which relates to system interoperability.
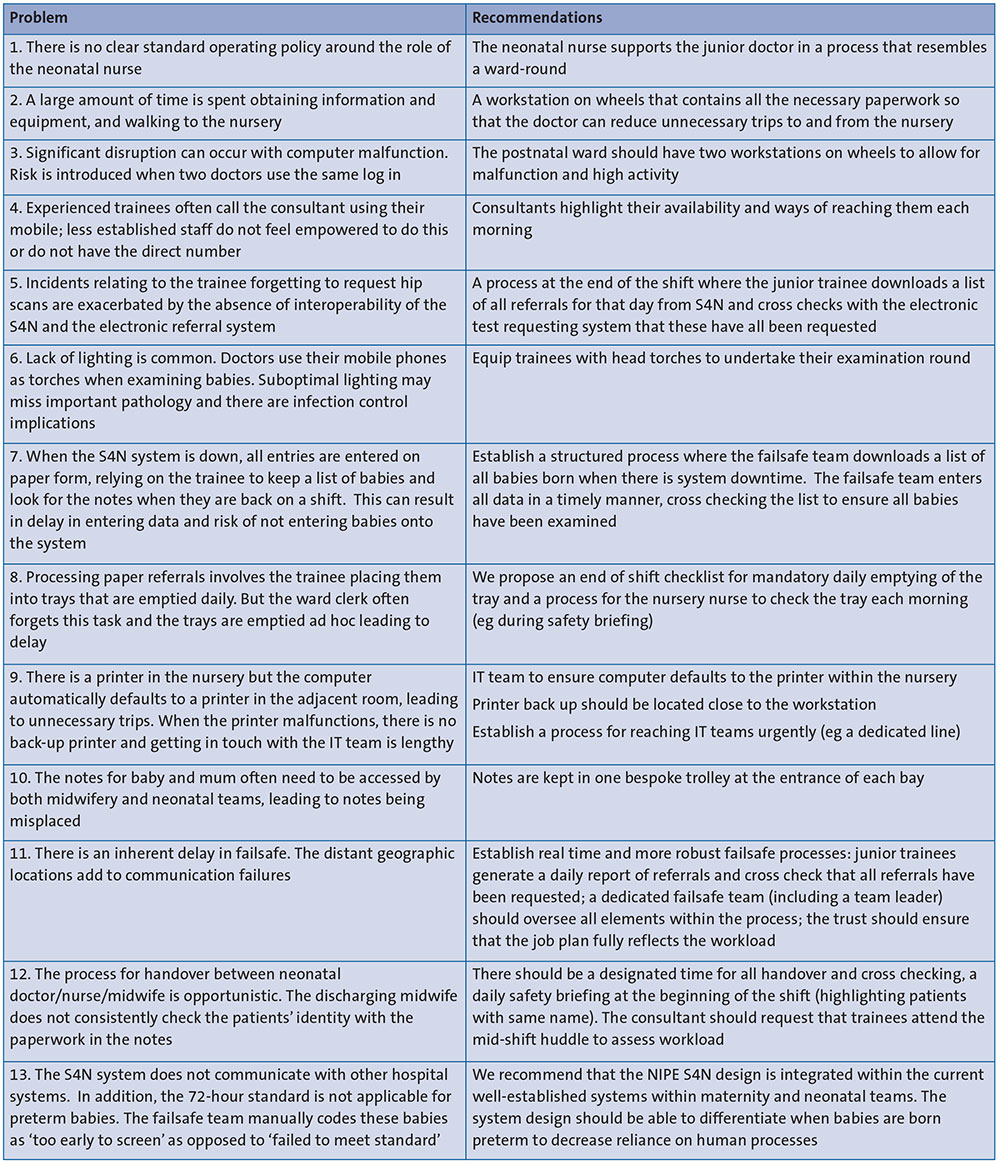
TABLE 2 The analysis yielded 13 recommendations.
Implementation, evaluation and sustainability
Many of our recommendations are centred to changes to team processes involving new ways of working and new responsibilities. Changes to the way a team functions can be very challenging – it takes time to fully embed change and often resistance is encountered from the people doing the work. Implementation can be done as plan-do-study-act (PDSA) cycles on a small-scale pilot and tested for further adaptations, acceptability, and effectiveness before implementing on a wider scale.16 The changes in the team processes can be made in parallel or in a sequential manner.
The recommendations relating to equipment will need a business case demonstrating the cost/benefit of reduc-tion in the work as shown by Chhokar et al (2005).17 The capital investment will need to be compared to the cost savings over time of paying extra doctors and cost of improved flow.
For evaluation, three types of measures can be used:
Outcome measures: these consider efficiency (eg length of time it takes to undertake examinations, average length of stay of well babies or the number of babies being sent to contingency wards) and safety (eg the number of screening incidents and number of missed referrals) and the effect the new processes have on staff (eg captured through interviews or questionnaires).
Process measures: adherence to the process is best measured through observations and interviews to look at whether safety briefing, consultant check-in and handover are carried out daily.
Balancing measures: It is likely that the new process will create unexpected or undesirable outcomes, eg it may impact the nursery nurse workload.
To ensure sustainability we need to establish quality standards that are representative of process benefits. A quality control run chart (eg monthly missed referrals) could be displayed in common areas to create team awareness of benefits.18 As with all new interventions, much work needs to be invested in changing culture through leadership, involvement, and champions.19-21
Conclusion
We have shown how combining human factor and quality improvement tools could complement each other to interrogate healthcare complexity and provide meaningful recommendations for improvement in system design. The input from patients and frontline staff can further augment service planning and redesign.
Or read this article in our
Tablet/iPad edition
- Human factor and quality improvement methodologies can be combined to provide meaningful recommendations for improvement in system design.
- This article describes how mismatch between policy and daily process operation can lead to human factor errors resulting from increased demand on healthcare staff.
Also published in Infant:
