

Development of better teamwork on a NICU using the TeamSTEPPS concept
Many transfers of care occur on a neonatal unit with the potential for conflict of opinion, which could create a challenging working environment and impact on patient safety. Using the TeamSTEPPS programme, we set out to explore the prevailing consultant culture and its impact on team members with the objective of creating a no-blame culture and promoting a supportive environment. Through the TeamSTEPPS programme and various other interventions we have achieved a strong sense of teamwork and a setting of supportive behaviour.
Sadaf BhayatMD, MRCPCH, PGcert Med Ed
Neonatal Trainee
Jennifer Birch
MbChB, MPCPCH
Consultant in Neonatal Medicine and Neonatal Clinical Director
Claudia Chetcuti Ganado
MD, MRCP(UK), MRCPCH
Consultant in Neonatal Medicine
claudia.chetcutiganado@ldh.nhs.uk
Neonatal Intensive Care Unit, Luton and Dunstable Hospital
The neonatal intensive care unit (NICU) is a highly stressful environment where human error is possible. It has been shown that efforts to detect and then remove weaknesses and vulnerabilities in a healthcare system can reduce the impact of human error and help to create and maintain a robust safety culture.1,2 The importance of effective teamwork in improving patient safety was one of the main objectives of the American report, To Err Is Human: Building a Safer Health System, which concluded that medical errors cause up to 98,000 deaths annually in the US.3
Background
Our unit is a level 3 NICU undertaking around 2,700 days of intensive care activity per year. In a 24-hour period there are three handovers involving up to four different consultants.
Significant expansion in our NICU consultant team between 2008 and 2016 and the innovative introduction of two different models of working had enabled the achievement of on-site consultant cover on the NICU for an average of 22 hours per day. However, this expansion and the differing working patterns produced some unanticipated challenges to effective teamworking. There was a perception of a ‘two-tier’ system and multiple transfers of care between consultants created room for conflicts of opinion and sometimes unnecessary changes in management. There was feedback from nurses that management plans repeatedly changed during handovers. It was felt that this source of conflict could impact on patient experience as well as the team.
Our aim was to explore the prevailing culture and to understand how it impacted on our team members, and explore ways of improving teamwork. Our main focus was on mutual support and conflict resolution. We wanted to create a culture where:
- team members embrace the concept of mutual support and where task assistance is requested and offered
- team members feel psychologically safe to trust other members, are accepting of feedback and also open to have their decisions challenged
- mistakes are acknowledged and learnt from
- gratitude and positivity are expressed between team members and the hard work done by the team is visibly appreciated by peers.
Methods
Overview of methods
The TeamSTEPPS Teamwork Perceptions Questionnaire (T-TPQ) and a small group feedback session were used to explore different team members’ views in four domains: team structure, communication, situation monitoring and mutual support. The results highlighted poor performance in the areas of situational monitoring and mutual support. The trainees faced the problem of differing opinions between consultants leaving them with a feeling of awkwardness and inability to speak up.
A list of better practices was written up and the following interventions were undertaken: teambuilding consultant session, teaching sessions of TeamSTEPPS programme, mid-shift huddle, reintroduction of staff recognition awards, new team ethos, team focus of the month, and introduction of tools for conflict resolution. Change was evaluated through a post-implementation survey.
The project was run by a steering group led by a neonatal consultant with interest in human factors and teamwork. The steering group consisted of a small group of neonatal consultants, neonatal nurses and neonatal trainees. The aim of the group was to understand team members’ perceptions of the current team climate using qualitative and quantitative approaches by use of a questionnaire and focus group to enable a working group to formulate potentially better practices, to disseminate the teaching and support the changes on the ground. The impact of the programme was assessed after a period of around 18 months to allow time for the learning to be embedded and to understand whether changes to practice had been sustainable. The questionnaire was repeated and other sources of feedback data, such as portfolio entries and trainee feedback surveys, were used to understand the impact on the culture.
Assessment of the teamwork climate
There are several existing tools that can be used to examine teamwork climate. We used the T-TPQ, a validated tool that has been shown to have a total survey reliability of 0.93.4 The survey was sent out to all team members working in the NICU including the administrative staff, nursing staff, trainees and consultants in June 2017.
To qualitatively explore how the culture impacted on other colleagues we ran a small group feedback session for trainees facilitated by a consultant outside the department. Trainees are present during consultant handovers and grand rounds therefore trainees can provide informative feedback on consultant attitudes during such transfers of care. The feedback identified that consultants did not always appear to respect each other’s views, and this made the trainees feel awkward, made them unsure who to trust and confused about who is right. The trainees felt this did not impact on patient safety, but it impacted on their ability to speak up.
The T-TPQ survey was repeated 18 months following the implementation of the different elements of our project. Although the teaching and the away day were completed within two months, we recognised that for culture change to occur the teaching needs to be embedded. This is a longer process and it depends on the early adopters acting as role models. The rolling ‘team focus of the month’ helped as constant reminder of ‘this is what we do here’. It also helped to reach out to newly appointed staff.
The post-implementation questionnaire was sent out in February 2019 and December 2019. We did this in order to capture two intakes of trainees as these rotate on a six-monthly basis.
The role of the nurses in the post-implementation survey was more complex. Nurses are a large part of the work force in the NICU but their perception of team climate may be influenced more by their own nursing interactions and leadership. In order to assess the impact of this, we chose to change the introductory statement of the two surveys. The survey sent out in February 2019 asked the nurses to comment on the team climate. The introductory statement of the December 2019 survey asked the nurses to comment specifically on how they perceive interactions of the medical team.
The programme
The results from the pre-implementation survey highlighted better performance in the elements of team structure and communication than situation monitoring and mutual support. Following review of the results of the pre-implementation survey, the working group identified the areas that needed improvement and created a list of potentially better practices, which served as the baseline team-building principles for the required change:
- common purpose, goals and values – what are we here to do together?
- what is right, not who is right
- collaboration, trust and respect among the various team members
- task assistance
- staff gratitude and positivity
- acknowledging mistakes
- managing conflicts.
Team-building consultant session
In order to make the improvements identified by the survey and the qualitative feedback from trainees, a team-building session was organised by the NICU Clinical Director (JB) and the Project Lead (CCG) on the consultant team away day. The session was facilitated by a professional coach and at the end of the session the team agreed on ground rules that would help their journey from ‘good to great’ including:
- more use of the word ‘we’ rather than ‘I’ or ‘you’
- work towards feeling comfortable with the concept of not always being right
- seeking help and advice (without seeing this as a sign of incompetence)
- reaching out to colleagues for a second opinion.
Teaching curriculum
A curriculum of teaching was adapted from the TeamSTEPPS resources and focused on the concept of mutually supportive behaviour in the workplace and how over time this would foster team adaptability, mutual trust, and team orientation. The other concept focused on situational monitoring and awareness and the different ways of creating a shared mental model to reduce error. The teaching was delivered to paediatric trainees and consultants in their journal club meetings.
Mid-shift huddle
A daily safety huddle was introduced at 13:30 to foster situational awareness and
to promote more collaborative and supportive team working. The huddle was based on the TeamSTEPPS STEP model:
- Status of the patient
- Team factors
- Equipment
- Progress towards the goal.
It was agreed that the huddle would be attended by the service consultants covering the different areas, the trainees and the neonatal charge nurses. The nurse in charge was encouraged to go around the ward prior to the huddle to identify any safety concerns that the nurses may have had following the ward round plan. The team members would assess their goals set for the day, measure their progress against them and reassign resources if needed. Team members would be asked if they were comfortable with their responsibilities and workload and if they needed help. Pending procedures would be identified and allocated. Finally, the members of the huddle would be asked to share any risk issues or areas of excellence the team could learn from.
Staff recognition awards
We set out to promote a culture of appreciation of peers and also to encourage good behaviours by reintroducing staff recognition awards. The team would receive a monthly email to nominate a peer who went the extra mile and there was a box in the staffroom for nominations. Those nominated would then receive a certificate at the end of each month and receive the positive feedback from their peers. Their photos would be displayed on the staff engagement board for that month.
Team ethos
To further foster an environment where collaboration is valued and there is sensitivity to the interdependency among the different team members, we created our own team ethos that we have displayed on a feature wall in the staff room – SUPPORT:
- Safety for patients and team members
- Understanding each other’s needs
- Promoting each other’s strengths
- Patient and non-judgemental
- Others’ contributions highly valued
- Respectful
- Tolerant of others’ weaknesses.
Team focus of the month
Although the project was geared primarily at the consultant body, we wanted to disseminate the learning and improve-ments to the wider team. We hoped to capture some of the wider team through the ‘team focus of the month’, an inspirational quote coupled with a team operating principle, for example:
The quote: ‘The nice thing about teamwork is that you always have others by your side.’
The principle: Mutual support is referred to as back-up behaviour and is critical to team performance. It involves team members assisting one another, providing and receiving feedback, exerting assertive and advocacy behaviours when patient safety is threatened.
The message is communicated to the medical team at the start of the weekly grand round. Additionally, it is sent out by email to the entire NICU team and displayed as a poster on the quality board.
Tools for managing conflicts
Conflict is inevitable in a team, however, if well managed is not inherently bad. We advocated the TeamSTEPPS DESCript tool:
- Describe the specific situation
- Express your concerns about the action
- Suggest other alternatives
- Consequences should be stated.
We have found the DESCript tool a very effective way of managing conflict and giving feedback. Ground rules for use of the tool were established: work on a win-win basis; make sure the location is private; use I statements rather than blaming statements; focus on critique as opposed to criticism, and focus on what is right not who is right. The tool was promoted in the curriculum teaching and as a team focus of the month.
Results
The response rate to the surveys ranged from 40% among the nursing team to 81% among the consultant team. The lowest scoring element of the T-TPQ (FIGURE 1) was ‘staff monitor each other’s performance’. The highest scoring was ‘staff exchange relevant information as it becomes available’.
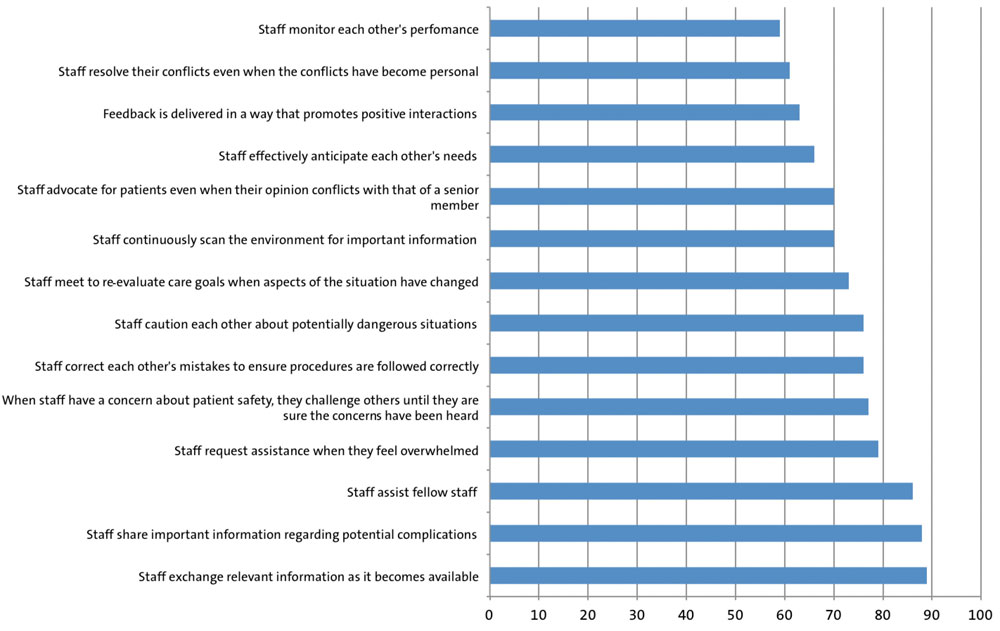
FIGURE 1 The range of positive responses in increasing order by question type (February 2019), n=31 (nurses 19, consultants 5, trainees 7).
As can be seen in FIGURE 2 the junior doctors tend to have the most positive perceptions among all elements apart from ‘staff exchanging relevant information as it becomes available’ and ‘staff advocate for patients even when their opinion conflicts with that of a senior member of the unit’.
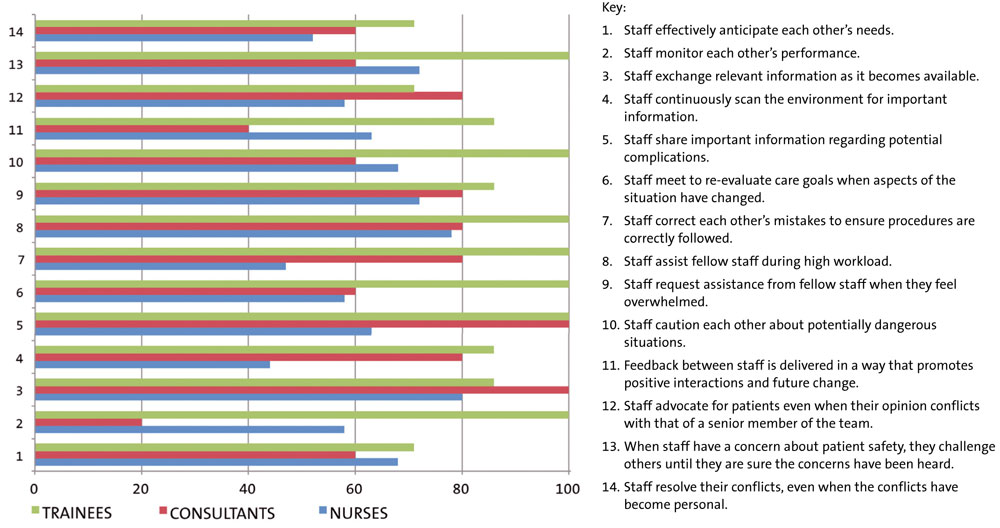
FIGURE 2 The range of perceptions by role.
TABLE 1 shows the perceptions of nurses on team climate. There was no significant difference in their perception of the overall team climate on the unit, but the results show that the nurses perceive an improvement in the interactions of the medical team around the areas of information exchange, huddling and staff assistance.
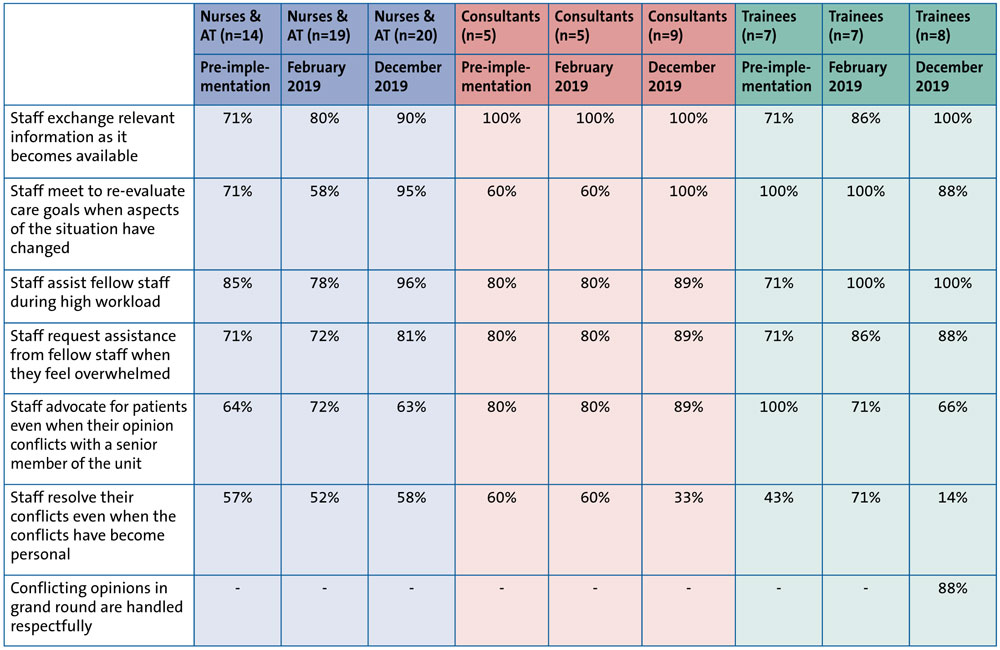
TABLE 1 The percentages of positive responses from the nursing/administrative team (AT), consultants and trainees over the course of the study. Note, the nurses/AT were asked about overall team climate at pre-implementation and the February 2019 timepoint. In December 2019 the questions referred to the medical team climate post-implementation.
The trainees’ responses show consistent and progressive improvement in the areas of information exchange and staff assistance (TABLE 1). The perception of conflict resolution was different in the group of trainees surveyed in February 2019, who perceived it as being 28% better than in the pre-implementation survey, as compared to the December 2019 survey group who perceived it to be slightly worse than the pre-implementation group. However, 88% of trainees felt that conflicting opinions in grand round are handled respectfully. Trainees scored ‘staff advocate for patients even when their opinion conflicts with that of a senior member of the unit’ low. This is likely to arise from their perceived perception that they should not question consultant management.
The consultants’ responses also showed consistent improvements in the areas of information exchange and staff assistance and patient advocacy. Conflict resolution, however, showed a variable response with an improvement in the first and a worsening in the second questionnaire (TABLE 1).
Mid-shift huddle
The huddle is well embedded and continues to occur daily. We have created a comprehensive checklist to support it, which has been adapted as each huddle led to opportunities to communicate better. The following four statements of the T-TPQ provided insight into whether the mid-shift huddle had met its aims.
- staff assist fellow staff during high workload
- staff request assistance from fellow staff when they feel overwhelmed
- staff exchange relevant information as it becomes available
- staff meet to re-evaluate care goals when aspects of the situation have changed.
Each of these four survey areas showed improvements among all staff groups by the December 2019 survey.
Conflict resolution
The statements from the T-TPQ that helped in assessing the elements of conflict and psychological safety were:
- staff advocate for patients even when their opinion conflicts with that of a senior member of the unit
- staff resolve their conflicts even when their conflicts have become personal.
Trainees were also asked an additional question to find out how consultants managed conflicts during grand round: are conflicting opinions in grand round handled respectfully?
Conflict resolution was one of the lower scoring and most concerning items on the pre-implementation survey. This item scored low among all different roles and staff grades. Staff advocating for patients is considered fundamental in creating a culture of empowerment where people feel able to raise their concerns no matter what their degree of experience and this is fundamental to promoting a safety culture on the unit. In this context, psychological safety is also critical. If someone feels intimidated by other members of the team he/she is unlikely to raise a concern even if that concern is about a patient.
Discussion
Overall, through this teamwork project we were able to improve mutual support and situation monitoring among the consultant team, which was generally reflected in perceptions of the staff. The trainees rated most elements more positively than the wider nursing team, a trend also found nationally in the SCORE survey carried out in the MatNeo project in 2018. This project was a national quality improvement programme undertaken as a Maternal and Neonatal Health Safety Collaborative working with maternal and neonatal services across England where 87 trusts carried out safety culture surveys. Overall we found a consistent improvement in the areas of information exchange, meeting to re-evaluate goals and staff assistance among the medical team, as assessed by the whole team. This finding is also consistent with our MatNeo survey, which showed that our teamwork climate as assessed by consultants and junior doctors (n=9) was close to the 75th percentile of the national benchmark at 44% (50th percentile 33%; 75th percentile 47%).5
It was clear throughout this project that leadership is vitally important to a culture of change and the leaders need to support those in the front line of this process. The engagement of the clinical lead had a significant impact in ensuring that the consultants engaged in this project.
Despite the difficulties in demonstrable improvements in conflict resolution we have shown that handover conflicts are handled respectfully at grand round, where 88% of trainees responded positively to the statement ‘conflicting opinions in grand round are handled respectfully’. Our findings imply that although conflicts are tangible in everyday handovers, the team has learnt how to handle these respectfully and consider the impact on the receiver.
Our group project was primarily qualitative. The biggest threat throughout this process was loss of objectivity and the length of time to see results. Another challenge was to capture the whole team. Further challenges were related to resistance to change – we encountered initial resistance to the mid-shift huddle due to worry that it might turn into another handover. We overcame this by ensuring that we kept strictly to the time cap of 10 minutes. The huddle has been embraced by both the medical and the nursing team.
The strength of our intervention was that it addressed both the social and task reflexivity of our team. We have achieved a strong sense of teamwork in a setting of supportive behaviour in addition to effective use of resources, collaboration and effective task completion, all of which can contribute to the patient safety climate.
We recognise that teamwork culture is a dynamic and ongoing journey and we are all ‘learning as we go’. This intervention was led by a motivated steering group willing to put in time and effort and thus had no monetary cost impact. Moving forward we recognise the need to train more nurse champions to be able to deliver the teaching curriculum to the nursing team and to embed the team focus of the month in the nursing handovers. We have also developed conflicting communication scenarios for use during simulation sessions, which will help us embed the more challenging tools such as the DESCript tool. We have now developed a teaching package to capture trainees during the early weeks of induction.
Conclusion
The TeamSTEPPS programme has been used in multiple healthcare settings, including one reported intervention that included NICU providers and showed an improvement in perceptions of teamwork.6-8 This project has further demonstrated that TeamSTEPPS can have a positive impact in a NICU environment and that these interventions could be applied to any NICU setting.
Or read this article in our
Tablet/iPad edition
- We set out to improve our teamwork with the main focus on mutual support and conflict resolution.
- We successfully implemented the TeamSTEPPS programme and a number of other practical interventions.
- Progress towards being a supportive environment was demonstrated through the team’s perceptions of attitudes utilising pre- and post-implementation surveys.
