

Unexpected neonatal herpes simplex virus infection in a premature newborn baby
In this article, we describe a case of neonatal herpes simplex virus infection with CNS involvement in an extremely premature infant delivered to a COVID-19 positive mother who had no history or symptoms of genital herpes infection. The infant completed a planned six-month course of acyclovir treatment and then prophylaxis but following discontinuation, he developed skin symptoms. Prophylaxis was resumed and continues at 24 months of age with several subsequent skin outbreaks. The difficulties from the mother’s perspective are also presented.
Mahmoud Koritena
Neonatal Clinical Fellow
Jennifer McGrath
Consultant Neonatologist
jennifer.mcgrath@nhs.net
St Peter's Hospital, Chertsey, Surrey
Koritena M., McGrath J.
Unexpected neonatal herpes simplex virus infection in a premature newborn baby. Infant 2023; 19(4): 141-44.
Background
Neonatal herpes simplex virus (HSV) is a rare but devastating condition, which can lead to significant morbidity and death. HSV infection should be considered in the differential diagnosis of the acutely unwell neonate.1
HSV type 1 (HSV-1) is a highly infectious virus that is primarily trans-mitted by oral-oral contact and causes orolabial herpes (notably ‘cold sores’) in those infected. HSV-2, by contrast, is almost entirely sexually transmitted and is therefore most closely associated with genital herpes.2
Although sexually transmitted herpes infections remain rare, they have increased in the last decade and it seems that neonatal herpes is also increasing. The number of cases of neonatal herpes in the UK has almost doubled since the first British Paediatric Surveillance Unit (BPSU) study (1986-1991) to the second (2004-2006).3 Also, a recent study from Nottingham4 (2006-2013) showed rates ten times higher than the first BPSU study, and served as a reminder of the devastating consequences of the disease.
Neonatal HSV infection can result from exposure to the virus in utero, perinatally or postnatally. In utero transmission is rare, resulting in around 5% of infections.5 Perinatal transmission (delivery through an infected genital tract or ascending infection due to ruptured membranes) is responsible for the majority of infections (around 85%). The remaining 10% of infections relate to postnatal acquisition from an infected caregiver.
Neonatal HSV infection can be classified into three main types:6,7
- Localised vesicular lesions of the skin, eye and/or mouth (SEM).
- Central nervous system (CNS) involvement (lethargy, poor feeding, tremor, seizures), with or without SEM.
- Disseminated infection – multiple organ involvement (lung and liver, coagulopathy).
It is important to consider the disseminated type of HSV infection when a neonate presents with a culture-negative septic picture associated with coagulopathy and/or hepatic impairment.8
The case presentation
We present the case of a male neonate, born to a primigravida mother extremely prematurely at 26+4 weeks’ gestation and weighing 1,030g. He was born by spontaneous vaginal delivery following prolonged rupture of membrane for 76 hours and reduced fetal movement.
The mother tested negative for hepatitis B, HIV and syphilis but was COVID-19 positive at the time of delivery, therefore, neonatal stabilisation was performed with the neonatal and obstetric team wearing full personal protective equipment (PPE). The baby was born with footling breech presentation in a poor condition, requiring intubation in the delivery room. Apgar scores were 2, 4 and 7 at one, five and 10 minutes of age, respectively. He was admitted to an isolation room in our level 3 neonatal intensive care unit (NICU) due to his mother’s COVID-19 status.
The infant had a relatively complicated neonatal journey and required a variety of specialist input. He was screened for sepsis on admission and started on first line antibiotics. The blood culture grew Escherichia coli on day 2 of life with C-reactive protein (CRP) rising to 19mg/L, therefore antibiotic cover was adjusted and continued until day 16 of life (TABLE 1). Due to the maternal COVID-19 status, SARS-CoV-2 RNA testing was performed on the baby on days 1, 3, 7 and 10 of life; the results were negative throughout and the infant never showed any clinical signs of COVID-19.
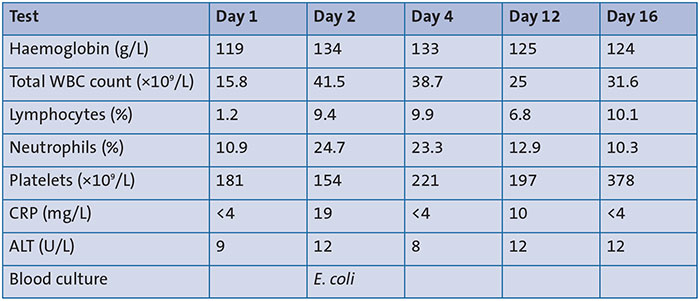
TABLE 1 Results of investigations carried out on days 1 to 16 of life. Key: WBC=white blood cell; CRP= C-reactive protein; ALT= alanine transaminase.
On day 6, the baby was felt to be clinically stable enough for a lumbar puncture in light of the E coli sepsis. His cerebrospinal fluid (CSF) was clotted and unexpectedly HSV-2 was detected in the CSF by a polymerase chain reaction (PCR) test, which is routinely performed on neonatal CSF in our trust. Consequently, intravenous (IV) administration of acyclovir was commenced. A PCR test on blood was positive for HSV-2 on day 10 of life. As per the tertiary paediatric infectious disease (PID) team advice to determine length of treatment, lumbar punctures were repeated on day 23 and day 30 of life (TABLE 2). HSV-2 was persistently detected and therefore IV acyclovir treatment was continued.
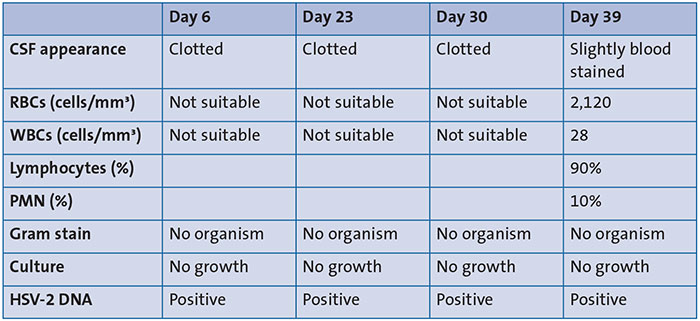
TABLE 2 CSF findings from lumbar punctures on days 6 to 39. Key: CSF=cerebrospinal fluid; RBC=red blood cell; PMN=polymorphonuclear leukocyte (polymorph).
On day 39, the CSF tested negative for HSV-2, the IV acyclovir was stopped and prophylactic oral acyclovir was commenced until six months of age, as per the PID team advice.
Other clinical observations
The infant was intubated and ventilated at delivery and received an initial dose of surfactant in the labour ward. He was ventilated until day 18 of life when he was successfully extubated to high flow nasal cannula. This was slowly weaned over his stay on the neonatal unit and he was discharged home on low flow nasal cannula oxygen at 0.2L/min. This was weaned and discontinued in the community.
Serial cranial ultrasounds showed bilateral intraventricular haemorrhage (IVH) with subsequent organisation and resolution of the blood clots. Brain magnetic resonance imaging (MRI) was carried out at 39 weeks’ corrected age, which showed mild dolichocephaly and changes in keeping with prematurity and resolved IVH. His subsequent development has been appropriate and he has achieved milestones on target.
During his stay on the NICU, he developed persistent hypernatremia and polyuria. His case was discussed with a paediatrician with endocrine expertise (both locally and with a tertiary specialist). He required an increased fluid intake of up to 200mL/kg/day to compensate for his persistent increased urinary output. The results of his baseline and provoked hormone levels suggested a working diagnosis of acquired diabetes insipidus. This was felt likely to be secondary to his acquired brain insults from the postnatal period (bilateral IVH and HSV-2 meningitis). Treatment with desmopressin was considered but eventually not required as his fluid requirement and urinary output gradually normalised along with his serum electrolyte levels by day 36 of life.
Discharge
The infant was discharged home at five months of age on nasal cannula oxygen, a combination of nasogastric tube feeding and bottle feeds due to pharyngeal dysphagia, and prophylactic oral acyclovir for at least six months.
The acyclovir was discontinued after completing the six months but two weeks later, the infant was admitted to the paediatric ward with fever and the development of herpetic skin lesions.
HSV-2 was isolated on viral skin swabs. He otherwise remained systemically well. He was treated with seven days of therapeutic IV acyclovir before he was discharged home on prophylactic oral acyclovir to continue for another six months, as per the PID team advice. He progressed to have intermittent subsequent episodes of purely cutaneous HSV outbreaks, which were successfully treated with short increases to treatment dose acyclovir (TABLE 3).

TABLE 3 HSV outbreaks between day 10 and 16 months of age.
Follow up
The infant has been followed-up as an outpatient by a consultant neonatologist, according to local guidelines for babies born extremely preterm. There has been input from the outpatient speech and language therapy, physiotherapy and tertiary PID teams. He is now two years old and progressing nicely. He has demonstrated appropriate neurodevelopment, has been fully orally fed since soon after discharge (fluid thickener has been weaned and stopped) and he continues to take prophylactic acyclovir. He will be undergoing a full neurodevelopmental assessment at two years corrected gestational age and his ongoing care will be transferred to a general paediatrician.
Discussion
In this article, we describe the case of a male preterm infant born at 26+4 weeks’ gestation who was delivered after spontaneous onset of preterm birth by normal vaginal delivery to a COVID-19 positive mother with no history or symptoms of maternal genital herpes infection. The infant was admitted to the NICU due to prematurity and underwent a septic screen that detected E. coli in blood cultures on day 2 and HSV-2 in CSF on day 6.
Recognition of maternal genital and neonatal HSV infection is important as it can be associated with significant adverse outcomes such as spontaneous abortion, stillbirth, intrauterine growth restriction, preterm birth, neonatal death and significant neurodevelopmental impair-ment.9 Approximately 95% of neonatal HSV infections are acquired during the peripartum or postpartum periods.5
Identifying at-risk infants can be challenging. 85% of neonatal HSV infections are acquired during the peripartum period, however, 60-80% of women who deliver an infant that develops HSV infection have no active evidence of, nor history of genital herpes, nor a sexual partner that reports a history.11 In our report, the baby's mother had neither a positive history nor evidence of active herpes infection, however preterm prolonged rupture of membranes is a significant factor in this case.
Current guidelines for diagnosis recommend virus culture and/or PCR assays on multiple samples, including surface samples (eye, mouth, nasopharynx and anus), skin lesions, blood and CSF samples.12
Early initiation of acyclovir treatment for the neonate is crucial in the treatment of congenitally-acquired HSV infection – particularly when suspicious skin lesions are present within the first 48 hours of life. Unfortunately, treatment cannot reverse any damage that may have already been sustained in utero; rather, it is aimed at prevention of progression to CNS disease.9
Current recommendations are for a neonate with CNS involvement to undergo further CSF sampling prior to the discontinuation of antiviral treatment. In the majority of neonates, the CSF will be negative and treatment can be safely discontinued. When HSV DNA remains detectable, treatment should be continued until the CSF tests negative.13 A further six months of oral suppressive antiviral treatment has been associated with improved neurodevelopmental outcomes in those infants surviving neonatal HSV disease with CNS involvement.14
Conclusion
This case demonstrates the importance of routinely testing septic newborns for HSV, the need for prompt initiation of antiviral therapy and consideration of longer-term prophylactic therapy for these infants, and the value of close collaboration between neonatologists and paediatric infectious diseases teams in the care of these infants.
Parental consent
The authors obtained written consent from the child’s mother for publication of the case history.
Or read this article in our
Tablet/iPad edition
- HSV infection in a newborn baby can be associated with significant morbidity and mortality.
- HSV infection should be considered in a sick neonate, even when an alternative diagnosis is made. When appropriate, an investigation for HSV and prompt treatment should be instigated.
- Appropriate diagnosis and treatment with antiviral therapy can significantly improve the outcome of these infants.
- Infants with neonatal HSV disease should receive at least six months of oral acyclovir suppressive therapy.
Also published in Infant:
