

Evidence base for a care bundle to reduce IVH in preterm neonates
Intraventricular haemorrhage (IVH) is a significant complication of premature birth occurring in 20-25% of neonates born before 30 weeks of gestation or with a birth weight of <1,500g. It carries a risk of adverse long-term neurodevelopment outcomes in very low birth weight infants. Multiple strategies are indicated in the literature to reduce the rate of IVH in preterm infants. A systematic literature review was performed and an evidence-based IVH care bundle was developed based on the best available evidence from the literature search.
Aesha Mohammedi
Consultant in Neonatal Medicine
aesha.mohammedi@nhs.net
Lawrence Miall
Consultant in Neonatal Medicine
Leeds Teaching Hospitals NHS Trust
Mohammedi A., Miall L. Evidence base for a care bundle to reduce IVH in preterm neonates. Infant 2023; 19(3): 94-99.
IVH is a major cause of brain injury in preterm neonates. It poses an ongoing challenge worldwide, especially in premature infants born at <30 weeks of gestational age. Global studies have reported the incidence of IVH as occurring in 20-25% of preterm neonates.1 IVH remains a threat to preterm neonates that are undergoing intensive care and is a frequent cause of death and morbidity.2-4 IVH decreases the chances of survival of a premature infant5 and contributes to multiple risk factors in the neurological sequelae associated with prematurity. A higher mortality rate has been reported among premature infants with IVH, compared to those without.2
Aetiopathogenesis of IVH
As a complication of prematurity, IVH can occur due to:
- germinal matrix vasculature fragility
- impairment of cerebral blood flow
- changes in cerebral perfusion
- coagulation disorders
- genetic factors
- oxygen toxicity.
IVH typically originates in the germinal matrix, a vascularised collection of neuronal-glial precursor cells that form part of the developing brain.6 It is characterised by a complex aetiopatho-genesis involving weakening of the capillaries in the germinal matrix, making it crucially vulnerable to anoxia. The severity of IVH is classified according to the amount of blood in the germinal matrix and lateral ventricles, as demonstrated by cranial ultrasound. Germinal matrix bleeding that is limited to the cerebral parenchyma is classified as grade I IVH. Accumulation of blood inside the ventricles falls under grades II and III; ventricular dilatation/enlargement is classified as grade III. Extensive bleeding (haemorrhagic venous infarction) in the parenchyma is classified as grade IV.6 Grades I and II are defined as mild IVH; grades III and IV as severe.
One of the major concerns with IVH is that it places infants at a higher risk of long-term neurodevelopmental complications. The majority of premature neonates with IVH suffer neurological sequelae.1,6 Approximately 50-75% of preterm survivors with IVH develop learning disabilities, cerebral palsy, and/or hydrocephalus.7,8 The US Census Bureau and the US National Institute of Child Health and Human Development Neonatal Research Network report over 3,600 new cases of intellectual disability each year in premature children affected by IVH.9,10 IVH and its consequent neurological sequelae continue to be a public health concern worldwide. Based on the available current evidence, there is no definitive treatment for IVH and the most effective strategy for prevention of IVH is prevention of preterm birth; an objective that has not yet been achieved. Hence, there is need to focus on appropriate measures to prevent the incidence of IVH.
Care bundles
A lot of modifiable factors that may contribute towards developing an IVH have been indicated in the literature, yet appropriate standardised recommend-ations for managing them are still needed. Such modifiable factors include:
- identification and treatment of maternal chorioamnionitis
- use of antenatal corticosteroids and magnesium sulphate
- delayed (optimal) cord clamping for at least a minute
- optimising thermoregulation and ventilation strategies
- early surfactant administration
- respiratory and cardiovascular care
- minimal handling
- slow IV boluses
- midline head positioning.
Implementation of an evidence-based care bundle as a standardised approach could improve the quality of care for these vulnerable preterm infants,11 improve their chances of survival and minimise neurological sequelae. Such a care bundle might also contribute to better and more focused evidence-based healthcare practices, not only to reduce IVH, but also to minimise other sequelae of prematurity.
The evidence base for IVH reduction
Despite the global emphasis on reducing IVH, there are relatively few published studies demonstrating the effects of using a standardised IVH care bundle. Some studies have suggested that a care bundle can reduce the incidence of IVH in a tertiary neonatal unit for preterm neonates born at <30 weeks’ gestation.12-18
Aims and methodology
This article sets out to address the following questions:
Question 1: Is there an evidence base to support a care bundle of interventions or measures to reduce the incidence of IVH in very low birth weight (VLBW) preterm neonates?
Question 2: What are the key practical, modifiable risk factors that should be included in a care bundle aimed at reducing IVH in VLBW preterm neonates in the UK setting?
An explorative literature search including English and non-English languages was conducted through Ovid MEDLINE 1996 to January 23rd, 2019; Embase 1996 to 2019 Week 03; EBM Reviews – Cochrane Database of Systematic Reviews 2005 to January 23, 2019; and EBM Reviews – ACP Journal Club 1991 to December 2018.
The following key words were used: ‘infant’, ‘newborn’, ‘preterm’, ‘premature infant’, ‘neonat*’, ‘neonatal’, ‘low birth weight infant’, ‘premature bab*’, ‘premature’, ‘intraventricular or intracranial adj2 (h*emorrhage* or bleed*)’, ‘intracranial hemorrhages/ or cerebral hemorrhage/ or leukomalacia or periventricular’, ‘patient care bundle*’, ‘care adj2 (bundle* or package*)’, ‘bundle adj2 (intervention* or measure*)’, ‘evidence based care adj2 (bundle* or package*)’, ‘reduc* or decreas* or lower*’, ‘risk factor’ ‘key modifiable risk factor*’, ‘intervention*’, ‘key measure*’, ‘non-invasive measure*’. Search terms were combined using Boolean words ‘and’, ‘or’. To enhance the search, asterisk (*) truncation, adj2 for proximity searching and speech marks for phrase searching were used.
Other search engines and websites were utilised including: NICE (National Institute for Health and Care Excellence) Evidence, Google Scholar, Google, UpToDate (an evidence-based clinical resource), Vermont Oxford Network data, Royal College of Paediatrics and Child Health, and the British Association of Perinatal Medicine. Reference lists within the articles generated in the original search were also reviewed.
Search results
The search yielded 11 articles pertaining to question 1 and 10 articles for question 2. The combination of question 1 and 2 results yielded 10 results in total, of which four met the aims of the study.
Relevant studies were included. Review articles were excluded from the final list. Authors of included studies were contacted via email in an attempt to identify further information on any absent data (published or unpublished).
The review of the literature
The studies identified by the literature search looked at measures to reduce IVH incidence rates. They included two quality improvement (QI) studies, one prospective cohort study and a systematic review article.
Question 1
Is there an evidence base to support a care bundle of interventions or measures to reduce the incidence of IVH in VLBW preterm neonates? The studies in TABLE 1 show that it is highly desirable to establish a standard evidence-based IVH care bundle to prevent IVH in preterm infants.6,19-21 Kubickav et al19 showed that a standard evidence-based respiratory care bundle significantly reduced rates of severe IVH and chronic lung disease in infants with a birth weight of <1,500g. We contacted these authors but unfortunately failed to receive more information regarding their future studies. The QI study by Arora et al21 showed that the rates of culture proven sepsis and the duration of mechanical ventilation were significantly reduced but the study failed to show any effect on mortality or other co-morbidities, including IVH.
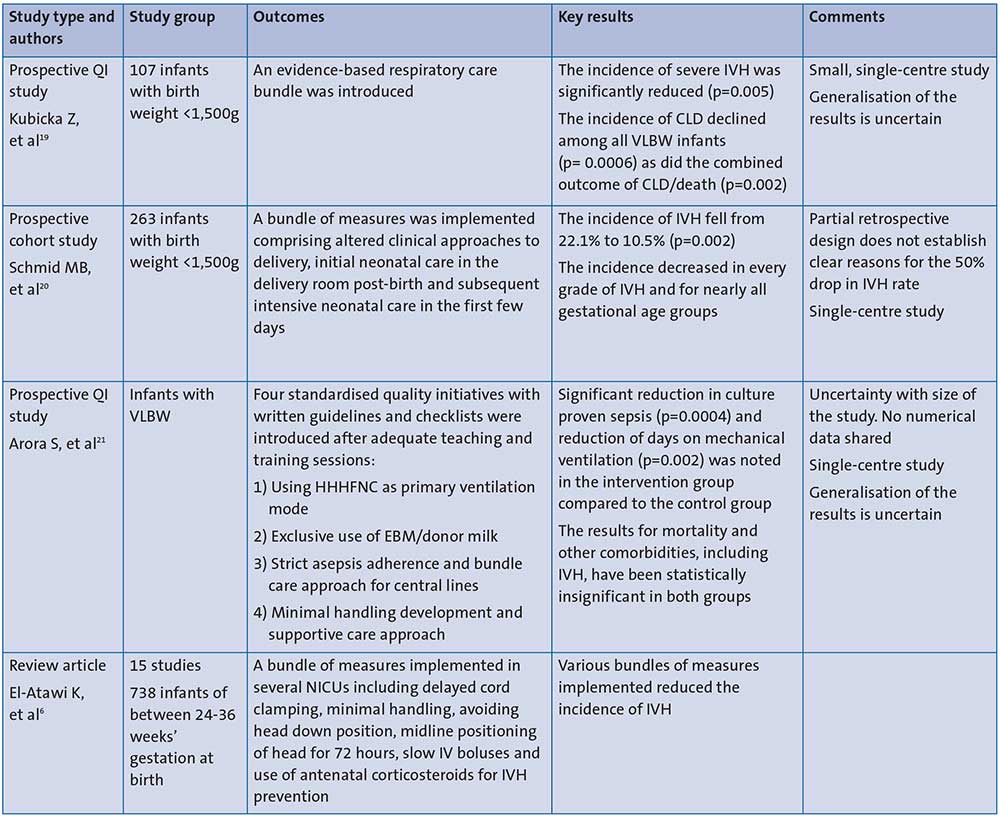
TABLE 1 Is there an evidence-base to support a care bundle of interventions or measures to reduce the incidence of IVH in VLBW preterm neonates? Key: CLD=chronic lung disease; HHHFNC=humidified and heated high flow nasal cannula; EBM=expressed breast milk; NICU=neonatal intensive care unit.
Interestingly, Schmid et al20 proved that by strict adherence to a bundle of measures and with regular evaluation, the incidence rate of all grades of IVH was reduced for almost all gestational age groups studied. El-Atawi6 also demonstrated that a standar-dised evidence-based care bundle to reduce IVH in preterm infants is warranted.
Question 2
What are the key practical, modifiable risk factors that should be included in a care bundle aimed at reducing IVH in VLBW preterm neonates in the UK setting?
The systematic review of the modifiable risk factors for IVH revealed that various studies have been conducted with the rationale of reducing morbidity and mortality rates arising from IVH (TABLE 2).
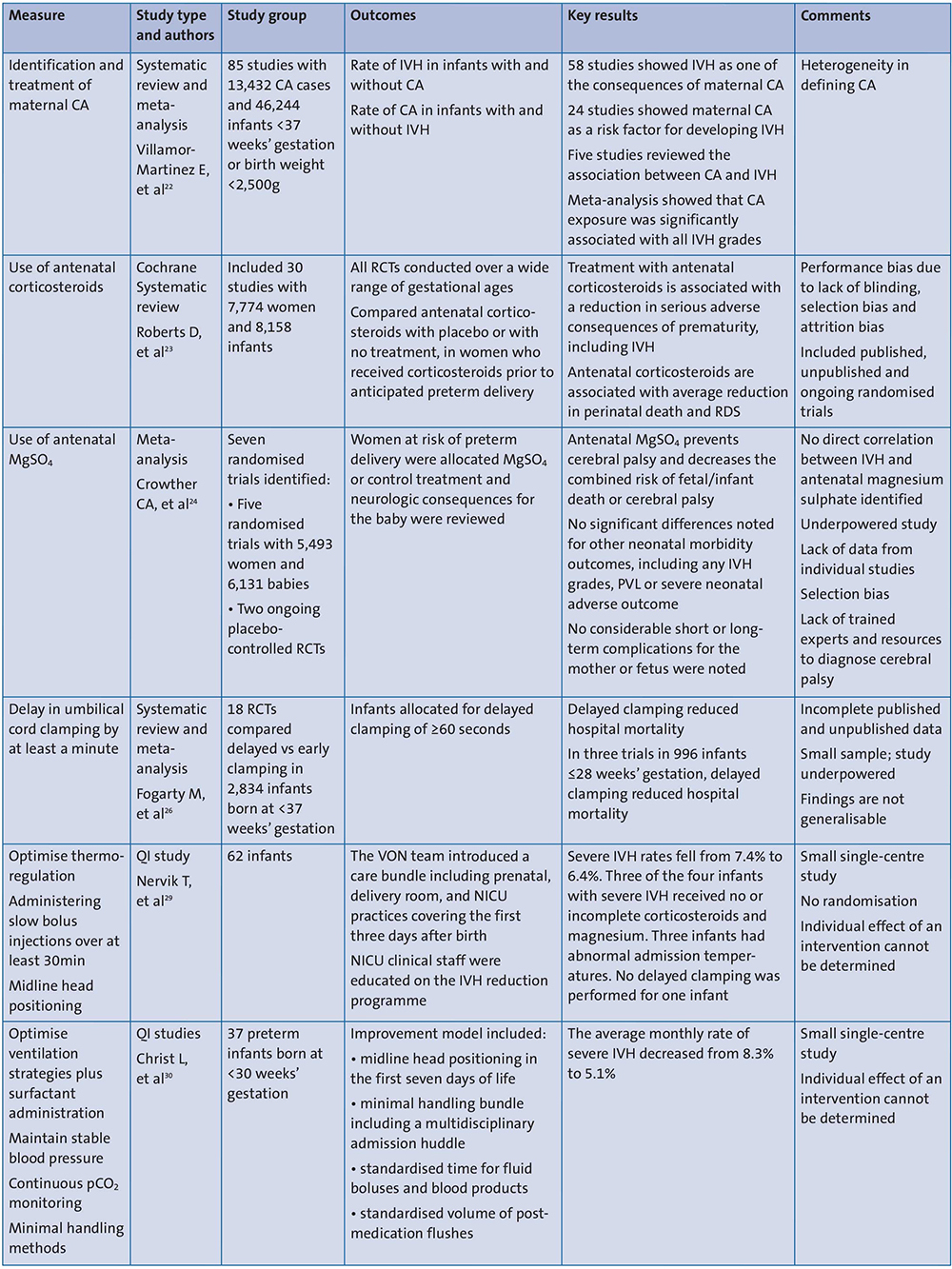
TABLE 2 What are the key practical, modifiable risk factors that should be included in a care bundle aimed at reducing IVH in VLBW preterm neonates in the UK setting? Key: RCT=randomised controlled trial; CA=chorioamnionitis; RDS=respiratory distress syndrome; PVL=periventricular leukomalacia; VON=Vermont Oxford Network; MgSO4=magnesium sulphate.
The modifiable risk factors have been classified into three groups as follows:
1. Delivery room interventions
- Identification and treatment of maternal chorioamnionitis
- Use of antenatal corticosteroids
- Use of antenatal magnesium sulphate.
Villamor-Martinez et al22 and Roberts et al23 showed that treating maternal chorioamnionitis and using antenatal corticosteroids are strong modifiable risk factors for IVH in preterm infants. Further studies by Crowther et al24,25 showed that antenatal magnesium sulphate reduces the risk of cerebral palsy and is associated with a reduction in the risk of IVH and paediatric mortality. The individual participant data meta-analyses identified five randomised trials (ACTOMgSO4, PREMAG, MAGNET, MAGPIE and BEAM) including 5,493 women and 6,131 babies, and two placebo-controlled RCTs (MASP and MAGENTA).24 Antenatal magnesium sulphate prevented cerebral palsy and decreased the combined risk of fetal/infant death or cerebral palsy. No statistically significant differences were noted for other neonatal morbidity dichotomous outcomes, including Apgar score at five minutes <7, active resuscitation at birth, use of ongoing respiratory support after birth, any IVH grades, periventricular leukomalacia, or severe neonatal adverse outcomes (death, bronchopulmonary dysplasia, patent ductus arteriosus, retinopathy of prema-turity, stage 3 necrotising enterocolitis).
Evidence shows that antenatal use of magnesium sulphate reduces the risk of cerebral palsy rather than a direct correlation with IVH.24,25 Nevertheless, we pragmatically included this factor as part of an overall neuroprotective strategy.
2. Interventions at birth
- Delay umbilical cord clamping by at least a minute
- Optimise thermoregulation
- Optimise ventilation strategies plus surfactant administration.
According to Fogarty et al26 delayed cord clamping reduced preterm hospital mortality and IVH is a recognised cause of preterm mortality. In addition, Mercer et al27 showed that delayed cord clamping offers protection from IVH and late onset sepsis. Rabe et al concluded that delayed cord clamping was associated with a 17% reduction in the relative risk of any IVH (grades 1‐4).28
QI studies by Nervik et al29 and Christ et al30 have proved that optimising normo-thermia and prompt ventilatory strategies including early surfactant administration reduces severe IVH in preterm infants. In the article by Nervik et al,29 the Vermont Oxford Network team introduced a care bundle including prenatal, delivery room and NICU practices covering the first three days after birth. NICU clinical staff were educated on an IVH reduction programme including:
- antenatal corticosteroids and magnesium sulphate
- delayed cord clamping
- prevention of hypothermia in the delivery room
- midline head positioning for the first 72 hours
- minimal handling and stimulation (no daily weights)
- slow fluid injections.
Christ et al30 further looked at:
- maintaining stable blood pressure
- continuous pCO2 monitoring
- minimal handling methods.
A recent study by Anup et al31 has shown that cord milking increases the risk of IVH in preterm infants and should be avoided.
3. Stabilisation in neonatal intensive care
- Respiratory care including continuous pCO2 monitoring
- Cardiovascular care: administering slow bolus injections over at least 30 minutes, maintaining blood pressure in the normal range
- Minimal handling developmental care methods32
- Midline head positioning.33
Although the studies provide strong evidence for various measures, they have a potential for bias. None of the studies include all the modifiable risk factors for IVH in one standardised evidence-based care bundle. A multi-centred high-quality research study with a larger population is needed to demonstrate conclusive benefit.
Practice implications
The primary aim of the study was to develop an IVH care bundle based on the best available evidence. The systematic review of the literature enabled us to develop a draft of an IVH care bundle, which mainly included the modifiable risk factors. A regional team of expert clinicians including 247 neonatal healthcare professionals from different centres were then identified. They were requested to review the components of the care bundle and rate the evidence supporting them. This included the modifiable risk factors obtained from the literature review and some distractor sham components. In order to obtain a standard consensus from the expert panel, a Delphi process with two rounds of surveys was conducted using an online Survey Monkey questionnaire. Most of the panellists correctly identified the distractor questions that lacked evidence and rated their evidence base as low. Also, many centres were aware of the modifiable risk factors. The results of the Delphi consensus process were used to finalise an IVH reduction care bundle.
There is good evidence6,30,34 that developmental care methods have been shown to reduce the rate of IVH in preterm infants by helping to minimise fluctuation in cerebral blood flow, including minimising pain and stress, avoiding environmental triggers, maintaining midline head positioning in the first 72 hours and the use of minimal handling measures. Therefore, these developmental methods were adapted in the form of a ‘bubble’ strategy at Leeds (FIGURE 1).
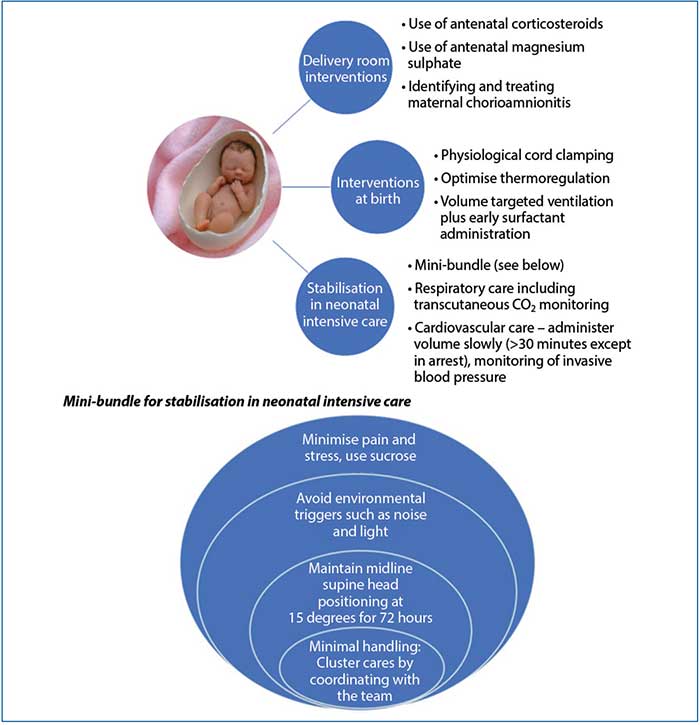
FIGURE 1 The IVH care bundle implemented at Leeds.
Following teaching and training of the multidisciplinary team with the standard best practice measures suggested in the bundle, a QI project with multiple PDSA (plan, do, study, act) cycles was implemented at Leeds in July 2020 to assess the clinical outcome measures in reducing the rate of incidence of IVH in VLBW preterm infants. The data are yet to be analysed.
Conclusion
IVH is an ongoing problem in preterm infants and it has contributed significantly to mortality and morbidity rates in many countries. From reviewing the current literature, where studies with the introduction of care bundles have been conducted to reduce the incidence of IVH, and with the results of the Delphi process, it is clear that some centres are aware of the modifiable risk factors for IVH. Despite this, there is a lack of a standardised approach to reducing IVH in preterm infants.
There are multiple possible strategies in the literature to reduce IVH yet it is impossible to identify the effect of a single measure in reducing IVH. Although there is no single preventive strategy for eliminating IVH, we can implement best practices from the developed IVH care bundle to reduce its sequelae of adverse outcomes.
A multidisciplinary team approach along with staff education is required to safely implement the care bundle. Consequently, we recommend that a standardised and appropriately evidence-based care bundle aimed at reducing IVH rates should be provided to all healthcare professionals working in NICUs, backed up by a specific programme of education. Conclusively, a QI study will help to assess if IVH is reduced post-implementation of the bundle.
Author contributions
Aesha Mohammedi: Study design, idea for the article, implementation, conducting the project, data analysis, writing. Lawrence Miall: Idea of the project, regular reviews, proof reading and suggestions.
Or read this article in our
Tablet/iPad edition
- 1. There is an ongoing need for a standardised evidence-based IVH care bundle.
- A systematic literature review was performed to inform development of an evidence-based IVH care bundle.
- A multidisciplinary team approach along with staff education and quality improvement (QI) methodology is needed to implement an IVH care bundle.
- A large multicentred research trial incorporating the best evidence-based preventative IVH measures is required.
Also published in Infant:
