

Practical considerations for deferred cord clamping with intact cord stabilisation
Deferred cord clamping (DCC) has been shown to significantly reduce mortality in preterm infants. It is therefore recommended as a standard practice in all preterm infants for a minimum duration of 60 seconds. Currently, this has been shown to be poorly implemented across all UK neonatal units. In addition to various factors underpinning this, there are practical difficulties in stabilising extreme preterm infants with an intact cord during DCC. In this article, we hope to provide some practical tips from our experience in successfully implementing this practice in our unit over the last 18 months.
Vennila PonnusamyConsultant Neonatologist, Neonatal Intensive Care Unit, St Peter’s Hospital, Chertsey, Surrey
vennilaponnusamy@nhs.net
On behalf of St Peter’s Neonatal and Maternity team
Background
It has been shown that optimal cord management (OCM) significantly reduces mortality and is likely to reduce morbidity in preterm infants.1,2 The British Association of Perinatal Medicine (BAPM) framework on OCM3 has recommended physiological delayed or deferred cord clamping (DCC) as the preferred method when compared to umbilical cord milking (UCM) to enhance placental transfusion and physiological transition at birth in preterm infants. Additionally, recently updated guidelines on newborn resuscitation from the UK and European Resuscitation Councils do not recommend UCM for preterm infants of <28 weeks’ gestation in view of possible risks due to intraventricular haemorrhage.4,5 Furthermore, data on DCC for babies <32 weeks’ gestation has been added as a measure for the 2021 National Neonatal Audit Programme (NNAP) to promote OCM across all units in the UK.6
Nevertheless, there are variations in practice, particularly for extreme preterm infants of <28 weeks’ gestation, where it is practically difficult to provide DCC alongside delivery room stabilisation/resuscitation at birth. This is due to these infants needing additional measures at birth for maintaining thermoregulation and initiating breathing. In term neonates not needing resuscitation, the recommended duration for cord clamping is longer, to allow for the majority of placental transfusion that occurs in the first three minutes.7 There is still lack of evidence on the recommended duration of DCC in preterm infants. Although DCC was defined in most studies as >30 seconds, the current recommended minimum duration of DCC in preterm babies is one minute, as it can be safely achieved alongside initial stabilisation in most preterm babies. However, data from a meta-analysis2 has shown an almost linear relationship between survival to discharge and duration of DCC from <1 minute to >2 minutes when compared to immediate cord clamping, although not statistically significant due to the small numbers in the sub-group analysis. Therefore, it is likely that a longer duration of DCC for a few minutes may be more beneficial than the minimum duration of 60 seconds to allow adequate placental transfusion,5 as the cord clamping should ideally be based on physiological factors rather than time based.8
While the benefits of resuscitation with an intact cord have not yet been proven, it is pragmatic to initiate stabilisation of all neonates including preterm babies before cord clamping happens at one minute.9 Intact cord stabilisation (ICS) allows effective stabilisation of all preterm infants, including extreme preterm infants of <28 weeks’ gestation, while the cord is unclamped for a longer duration of >1 minute. While there is lack of consensus and evidence on the benefits of ICS, this has been shown to be beneficial in animal studies, as it allows for lung aeration before cord clamping.8,10 A recent survey of all neonatal intensive care units in the UK11 has highlighted that, although only 6% of units (3 out of 48 units) are currently practising ICS as a standard, the majority of units are either trying to provide this where feasible or are currently working on implementing ICS in the near future. At birth, in addition to keeping preterm infants covered and warm, gentle stimulation and respiratory support can also be provided for up to a few minutes as needed with appropriate set up, while the baby is attached to the cord. This requires joint team working between midwifery, obstetrics, anaesthetists, theatre staff and neonatal staff to ensure all babies are safely assessed and appropriately supported while maintaining normothermia.
Therefore, in order, to ensure extreme preterm infants benefit further from OCM, we implemented ICS for a minimum of 60 seconds (30 seconds in the beginning when we started the project) to a maximum of three minutes at St Peter’s Hospital in November 2019. Through this article, we share our set up and practical tips on implementing ICS, which we have learnt through experience in order to help other units in the process of considering this. These suggestions will also be useful for units planning to implement DCC for just one minute without ICS, with required modifications.
Principles of ICS
In line with the BAPM OCM toolkit,3 all preterm babies should have their umbilical cord clamped after 60 seconds from birth. There are very few circumstances where this might be difficult to perform, eg complete placental abruption, snapping of umbilical cord or massive acute maternal haemorrhage needing resuscitation. In such circumstances, BAPM recommends use of UCM to facilitate placental transfusion.
In all other circumstances, the aim of ICS would be to allow physiological transition of breathing and circulation to be established during stabilisation/resuscitation for a minimum of 60 seconds to a maximum of three minutes in all preterm infants of <37 weeks’ gestation. We call this the ‘new ABC approach’, which stands for keeping the airway patent, allowing/promoting the baby to establish breathing by themselves where possible using gentle, but deliberate stimulation and then clamping the cord.
During stabilisation with DCC, most preterm babies will start to establish spontaneous breathing before 60 seconds with minimal assistance.4 Therefore, for a longer duration of DCC with ICS, most preterm babies will only need to be kept warm alongside provision of positive end expiratory pressure (PEEP) to continue to support their breathing. Very few babies, particularly those <27 weeks’ and those born in poor condition, would need further support in the form of positive pressure ventilation (PPV) using peak inspiratory pressures (PIP) and PEEP using a facemask in the first three minutes.
Equipment
DCC with ICS can be facilitated either on the mum’s lap or on any platform between the mother’s legs. Having a resuscitaire closer to the mother12 or having a purpose-built stabilisation platform such as LifeStartTM (Inspiration Healthcare, UK)13 would help to provide additional respiratory support as needed in the first few minutes. LifeStart has particular advantage in caesarean sections, as it can be covered completely with sterile drapes, unlike resuscitaires. Another option includes the use of a mobile nasal high flow delivery device such as Vapotherm Precision FlowTM (Vapotherm, UK),14 as used in our unit.
In addition to the major equipment, the following basic equipment would be useful to support the onset of spontaneous breathing and/or lung inflation while performing DCC on the mother’s lap/abdomen or on her bed between her legs, especially in preterm babies:
- a plastic bag/plastic wrap/thermal suit for preterm and intrauterine growth restriction babies, as per local guideline
- a heat source to aid thermoregulation in the absence of an overhead heater for the first few minutes, eg a transwarmer for extreme preterm or growth restricted babies, warm towels, hats
- saturation probes and monitor
- temperature monitoring equipment.
When a preterm baby is delivered by caesarean section, a sterile drape to cover the platform and sterile plastic bags to cover the baby with the intact cord are needed. Use of a sterile polyethylene suit known as a Neohelp™ bag (Vygon, UK) allows the cord to be kept intact using the velcro adhesion while still covering the baby well enough, including the head to keep it warm.
Set-up/understanding your environment
It is important to consider various factors, such as the size of the delivery room/theatre, availability of equipment including piped gas (oxygen and air) supply, number of staff present at a preterm delivery, etc, before deciding on the preferred set-up for each unit. One of the most effective ways to do this would be to simulate various scenarios in the delivery room and theatre using resuscitaires and LifeStart. From our experience, LifeStart can be obtained on loan from Inspiration Healthcare for a trial period along with training to facilitate this. Discussing with other neonatal units who are using LifeStart would also help to identify the practical aspects relating to the care/maintenance/use of the equipment. Following simulation, agreeing a layout for each unit’s own delivery room and theatre is helpful. An example of the layout used in our unit is shown in FIGURE 1.
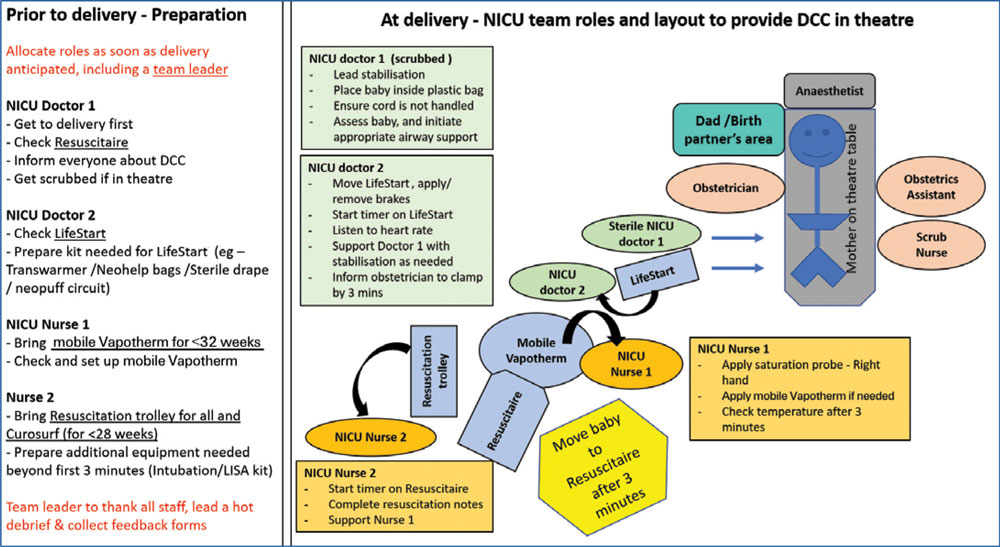
FIGURE 1 A model for equipment and MDT set up in theatre for facilitating DCC during intact cord stabilisation. Key: NICU=neonatal intensive care unit; DCC=deferred cord clamping; LISA=less invasive surfactant administration.
Communication
It is fundamental to have clear communication between the multidisciplinary staff members and the parents when providing initial stabilisation of preterm infants with the intact cord attached to the mother. Parents have reported that they feel positive and reassured when present at the stabilisation of infants with intact cord due to improved communication in those settings.15
The following elements should be covered for effective communication with the whole team:
- Provide written information on DCC during antenatal visits and encourage parents to include this in the birth plan.
- The midwife should discuss the plan for DCC with the parents in the pre-delivery counselling for babies of all gestations.
- For babies of <34 weeks’ gestation, there should be a pre-delivery huddle with the perinatal team (obstetricians/midwives) to discuss the birth plan in line with the BAPM Preterm Optimisation Care bundle.16 A template to undertake the pre-delivery huddle is shown in FIGURE 2.
- At delivery, use specific reminders to perform DCC in line with local guidance (eg WHO checklist for theatres or STEPP card for all high risk deliveries).3
- Allocate roles to the team members prior to delivery, including a team leader.
- Neonatal team leader to discuss the clinical situation with the team and confirm the likely mode of respiratory stabilisation.
- Prepare adequate equipment based on the type of delivery (vaginal/caesarean) and the gestation of the baby.
- Allocate a member of staff to scribe for the stabilisation/resuscitation records. Use a well-designed stabilisation sheet with simple tick boxes and reminders to aid completion by the scribe (FIGURE 3).
- Ensure there is a member of staff to communicate with parents if ongoing resuscitation is required or to assist in taking pictures/videos for parents, in line with their wishes.
- Once the baby has been stabilised, consider a delivery room cuddle with the parents for all gestational ages.

FIGURE 2 The preterm delivery checklist to facilitate DCC to be commenced on admission to the labour ward.
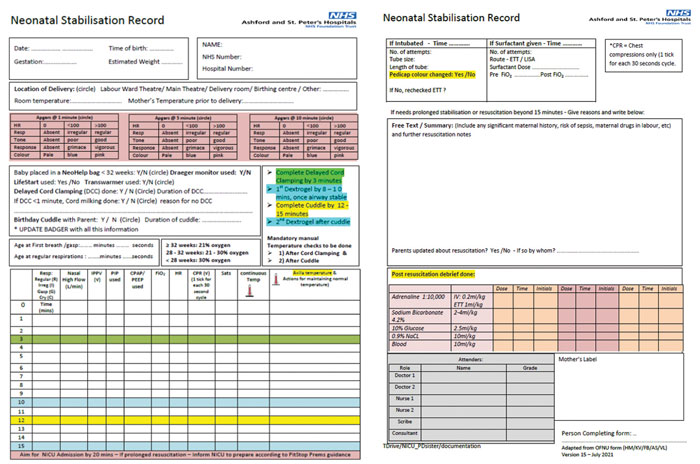
FIGURE 3 The neonatal stabilisation record sheet to improve documentation of DCC.
Multidisciplinary team (MDT) working
Specific role allocation alongside excellent communication can aid successful implementation of OCM. This will need to be tailored to fit each specific team depending on the level of neonatal unit and staff availability and experience. Use of simulation helps to identify the advantages and limitations of each set up and team dynamics.
As with any complex situation, it is crucial to have clear roles and responsibilities for the various team members involved in attending a preterm delivery to ensure successful team working. This is even more important given the changes in the traditional role for various members to provide DCC with ICS and the use of additional equipment. Generally, a minimum of two neonatal nurses and two doctors attend the delivery of extreme preterm babies of <28 weeks’ gestation in most neonatal units. A suggested template defining roles/responsibilities for team members as used in our unit is shown in FIGURE 1. This could be adapted to suit different units based on the equipment used for stabilisation and personnel available to attend the deliveries. The doctor 1 and nurse 1 usually provide ‘hands on’ stabilisation for the preterm baby and therefore could be a junior or senior person depending on the expected complexity of the delivery. Doctor 2 and nurse 2 provide ‘hands off’ assistance by leadership management and assisting with ongoing prolonged stabilisation, as required. The role of doctor 1 and 2 can also be performed by an advanced neonatal nurse practitioner. It is essential to ensure clear roles are assigned to the midwife/obstetrician and theatre scrub nurse to ensure a true multidisciplinary approach. In our unit, the midwife ensures the resuscitaire, LifeStart and clean suction equipment are in the room prior to delivery; informs the neonatal team when the baby is born; helps place the baby inside the bag, and is ready to clamp and cut the cord at three minutes or earlier if requested. The scrub nurse positions the diathermy wires so that the LifeStart can come closer to the table; has sterile paper towel if needed to wipe the baby; ensures the cord is not handled by anyone, and makes sure that neonatal team members do not contaminate the maternal sterile field.
Incorporating DCC into the newborn stabilisation guideline
It is useful to incorporate this change in practice alongside various other elements of newborn stabilisation, including further stabilisation beyond the first few minutes, maintenance of effective thermoregulation, and providing delivery room cuddles to parents. This ensures that the team is clear with the full approach to stabilisation of preterm infants in the delivery room. FIGURE 4 outlines a model for producing a simple standard operating procedure based on the guideline, as used in our neonatal unit. Having this laminated and displayed in prominent locations would allow the team to quickly refresh the guideline before delivery.
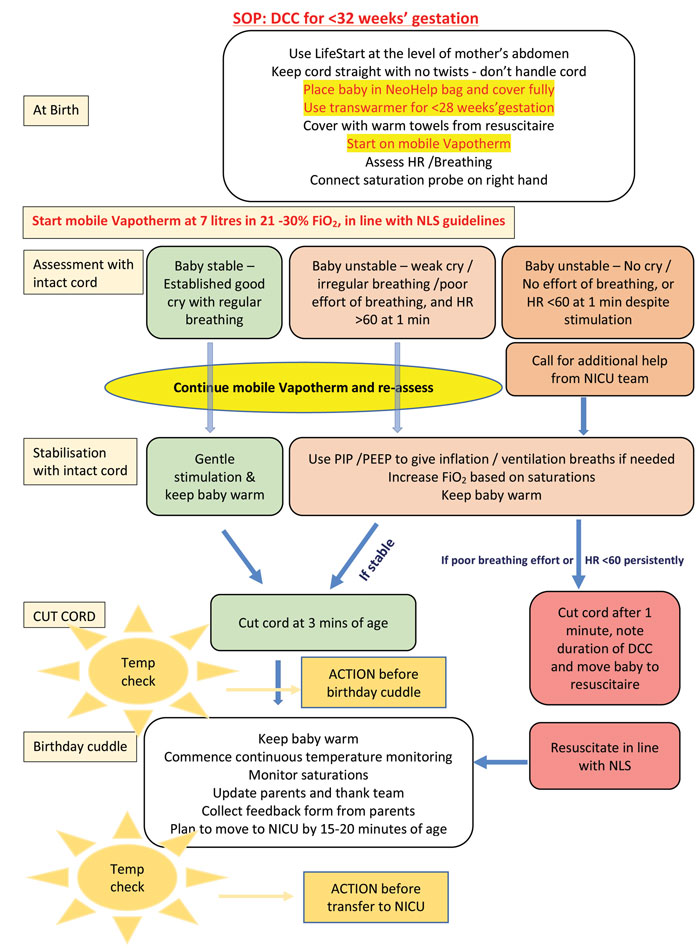
FIGURE 4 An example of a standard operating procedure to incorporate DCC in the unit’s delivery room stabilisation guideline.
Thermoregulation during DCC
Hypothermia has a direct link to mortality and morbidity in preterm and low birth weight babies.17 Therefore, it is crucial that a member of staff is allocated to monitor temperature closely throughout stabilisation/resuscitation and provide active intervention, as necessary. Use of the BAPM Normothermia Toolkit18 would help to review practice and improve thermoregulation in all preterm deliveries. Effective planning pre-delivery and active manage-ment post-delivery using continuous monitoring is the key to success.
Prior to delivery
There are certain elements of temperature control that should be considered prior to delivery.
- Ensure a warm draught-free environment of 24-26°C. This may require temporary elevation of the theatre temperature in anticipation of OCM. This may be uncomfortable for those scrubbed up. Prior discussion with the obstetric team would help to implement this practice.
- Ensure warm towels (sterile, if in theatre) are available for holding the baby during OCM and for later transfer to the stabilisation area. Use of towel warmers could facilitate availability of warm towels at all times.
- Ensure (sterile, if in theatre) a plastic bag or thermal suit is available for use for preterm babies, as per unit guideline.
- Ensure that the heat source is activated on the resuscitaire.
- Ensure that a transwarmer or another thermal mattress is available and activated. Do not use a transwarmer on the heated resuscitaire, as it can overheat the baby.
At delivery
- Depending on birth weight and gestation, place the baby into a plastic bag/thermal suit immediately at birth and from the onset of OCM.
- Otherwise use warm towels to dry and stimulate the baby.
- Cover the baby’s head with a hat as soon as possible.
- Monitor the baby’s temperature after OCM, ideally with continuous temperature monitoring.
- Promote active thermoregulation at all times during ongoing stabilisation/resuscitation to maintain normothermia.
- Once clinically stable, facilitate a birthday cuddle with the mother prior to transfer to the neonatal unit.
- Ensure the mother’s body temperature is normal for the delivery room cuddle and use warm towels as required.
- Check the baby’s temperature after the delivery room cuddle, to ensure it is within the normal range prior to transfer to the neonatal unit.
Quality improvement tools
There are a number of quality improvement tools available to facilitate the introduction of DCC through the BAPM Optimal Cord Management Toolkit.3 Once the new practice is set up to be implemented, it is extremely important to ensure that data are accurately captured through NNAP to allow a regular review of practice. In order to sustain the change, adequate training should be provided to all groups of staff involved in the delivery of neonates, including theatre staff in each hospital. This should be on an ongoing basis due to the rotational work pattern of staff. The use of teaching videos, simulation videos and newsletters will help towards regular training.
Most importantly, engaging parents with information and teaching about OCM in antenatal classes and the use of a parent information leaflet would help to inform parents of the benefits of OCM prior to birth and encourage them to incorporate OCM in their birth plan at booking.
Summary of the practical considerations
- Early cord clamping is contraindicated, as it causes harm. Even in a precipitate delivery where the neonatal team is not present, the cord should not be clamped early to initiate resuscitation. The midwifery team should start gentle stimulation of the baby with an intact cord, while keeping the baby warm for one minute. Only clamp the cord after one minute to move the baby to the resuscitaire.
- Preterm babies should not be delivered on to the resuscitaire with an intact sac. Splitting the sac results in a large amniotic fluid spill and increased difficulty in keeping the baby warm inside the plastic bag. The obstetrician should incise the sac at delivery and place only the baby inside the bag.
- The cord should not be handled; assessing for an arterial pulse is not required as DCC is about placental venous return to the baby and not arterial blood supply.
- An active approach to thermoregulation with the use of continuous temperature monitoring in all preterm and growth restricted babies is necessary throughout the stabilisation, including the duration of OCM.
- If implementing ICS, aim to maintain a patent airway to allow the baby to breathe spontaneously or assist with gentle ventilation as required before cord clamping to promote physiological transition.
- Successful implementation of OCM requires excellent team work and communication within the MDT, including the parents.
- Having set allocated roles for team members and a clear layout may be beneficial to the success of OCM. These will vary depending on the unit setting and staffing.
- Ongoing audit and quality improvement projects will help to improve the implementation rates of OCM.
Conclusion
Using the methods described in this article, we were able to introduce DCC successfully in our unit over a period of 12 months. However, this required changes in practice with the set up at delivery, equipment, different roles and responsibilities for various team members, improving our ways of MDT communication using pre-delivery huddles, and empowering families to incorporate DCC in their birth plan. It is also important to sustain this change through ongoing teaching, training and audits. We hope this article provides a few practical tips for units working towards implementing DCC, particularly in extreme preterm infants where stabilisation with an intact cord is considered.
Acknowledgement
The author would like to thank all the multidisciplinary members of St Peter’s neonatal, maternity, anaesthetic and theatre scrub teams for embracing the change positively and to the simulation team for all the hard work with training and set-up. Special thanks to Sarah Shadbolt from Inspiration Healthcare for the loan of the LifeStart equipment and support at all times. With gratitude to Little Roo Neonatal Charity Fund for helping with all the equipment costs to implement this practice in the unit.
Or read this article in our
Tablet/iPad edition
- DCC should be provided to all preterm infants as a standard care at birth.
- Effective planning, team working and communication would facilitate the teams to provide DCC alongside stabilisation in extreme preterm infants.
- Use of simulation, quality improvement tools, regular teaching and training will
Also published in Infant:
