

Current use of probiotics in neonatal units in England
Recent studies and meta-analyses suggest that probiotic supplementation in very preterm and very low birth weight babies has beneficial effects. We conducted a survey to shed light on the current use of probiotics across neonatal units in England, in light of recent recommendations. To our knowledge this is the first comprehensive survey of probiotic use covering all levels of neonatal units in England.
Ashok Karupaiah
Consultant Paediatrician and Neonatal Clinical Lead, Department of Paediatrics and Neonates, Walsall Manor Hospital NHS Trust
ashok.karupaiah@nhs.net
Abdulhakim Abdurrazaq
Locum Consultant, Department of Paediatrics, Walsall Manor Hospital
NHS Trust
Josephine Quaynor
Specialty Trainee in Paediatrics,
West Midlands Deanery
Karupaiah A., Abdurrazaq A., Quaynor J. Current use of probiotics in neonatal units in England. Infant 2023; 19(3): 84-86.
Necrotising enterocolitis (NEC) is a leading cause of mortality and morbidity in premature very low birth weight infants (<1,500g).1 Recent studies2-5 and a meta-analysis6 suggest that probiotic intervention can have beneficial effects. A Cochrane review from 2020 showed that giving probiotics to very preterm and very low birth weight infants may reduce the risk of developing NEC, and probably reduces the risk of serious infection and death.2 Probiotic use in a single neonatal unit in Newcastle, UK, did not reduce overall mortality or rates of NEC, late-onset sepsis (LOS) or focal intestinal perforation (FIP) but subgroup analysis identified NEC risk reduction in infants born at >28 weeks’ gestation, and LOS reduction in infants born at <28 weeks’ gestation.5
There is uncertainty around which specific strains of bacteria in probiotics might potentially be used for preterm infants and which strains should not be used; some appear to be more beneficial than others. Similarly, information on dosage and how long to supplement is not consistent. The most recent recommendations from the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) provide advice on specific strains, either singly or in combination, and address several safety issues for probiotic supplementation in preterm infants.3
Probiotics brands
The probiotic brands commonly available in the UK include:7,8
Labinic (Biofloratech Ltd, UK)
Lactobacillus acidophilus, Bifidobacterium infantis, Bifidobacterium bifidum. Liquid preparation. Dose = 5 drops (0.2mL) once daily via naso- or oro-gastric tube.
ProPrems (Neobiomics AB, Sweden)
Bifidobacterium infantis, Bifidobacterium lactis, Streptococcus thermophilus. Powder sachet (0.5g) once daily, mix with 1-3mL maternal expressed breast milk (MEBM) and administer via naso- or oro-gastric tube.
Infloran (Desma Healthcare, Switzerland)
Bifidobacterium bifidum, Lactobacillus acidophilus. Powder capsule (250mg),
1 capsule once daily, dissolve in 1mL MEBM, administer via naso- or oro-gastric tube.
Acidophilus Extra 4 (Lamberts Healthcare Ltd, UK)
Lactobacillus acidophilus, Bifidobacterium bifidum.
The products currently available are disparate in terms of their cost and administration. During the course of the survey and our observations across the region, we noted that as some probiotic brands were more expensive than others (as much as a seven-fold price difference), hospital trusts found it easier to get approval for use of the brands that cost less.
Introducing probiotics to our neonatal unit
In February 2022 we introduced probiotics to our neonatal unit in Walsall Manor Hospital. We are a local neonatal unit (LNU) in the West Midlands Neonatal Operational Delivery Network. Prior to the introduction of probiotics, we tried to find out probiotic implementation experience across the West Midlands region. To our surprise, we found it difficult to get a clear picture of the extent of probiotic use; the strains used and the decision-making process behind the choice of probiotics. This led us to carry out a survey of the current use of probiotics in neonatal units in the region and in the whole of England.
We identified that many units had probiotic implementation in their trust improvement agenda but were dealing with more urgent issues. Some were not convinced of the safety of probiotics and were awaiting more conclusive studies. The units that had already established use of probiotics continued to use them, even though the strains were different from the most recent recommendations from ESPGHAN.3 We felt that some trusts were grappling with uncertainties around the selection of optimal probiotic strains.
We proceeded to introduce ProPrems to our unit, as per the ESPGHAN recommendation on probiotic strain selection.3 We commence probiotics after obtaining informed consent from a parent.
Surveying probiotic use
On review of the literature, the last published survey on probiotic use in neonatal intensive care units (NICUs) was conducted in 2018, which reported that 17% of UK NICUs use probiotics.1 However, this study did not include LNUs or special care baby units (SCBUs). Since then, we have seen publication of the Cochrane review,2 the ESPGHAN recommendations3 and various meta-analyses.4-6 We wondered if this might have resulted in a change of practice in neonatal units, although a recent editorial (2022) noted that uncertainty on optimum probiotic strain selection could affect unit uptake.9
We conducted this survey to shed light on the current use of probiotics across neonatal units in England, especially in light of recent recommendations.2-4,6 To our knowledge, this is the first comprehensive survey of probiotic use covering all levels of neonatal units in England.
Methodology
We conducted a telephone survey of neonatal units in England on the use of probiotics. We contacted all of the 155 neonatal units in England (48 NICUs, 74 LNUs and 33 SCBUs) directly by telephone between July and September 2022. We followed up phone calls if we were advised to call back later. We paged the neonatal registrar if there was repeated difficulty in contacting a team member. We asked the respondent if they used probiotics in their units and the brand they used. We also asked how long they had used probiotics. If the unit did not use probiotics, we asked if there was any plan to introduce them in the future.
We had a good response to our calls; about 70% of calls were answered first time, while others needed further contact. We obtained responses from all units. More than two thirds of the responses (106) were from a neonatal staff nurse, 31 responses came from registrars, 11 from charge nurses, three from advanced neonatal nurse practitioners, two from the onsite consultant, one from the unit coordinator and one from the lead pharmacist (neonatal). We stored the information in our database; we did not record any conversations.
Results
We discovered that 65 out of 155 (41.9%) neonatal units in England use probiotics. 90 neonatal units (58.1%) do not use probiotics (TABLE 1 and FIGURE 1). 30% of SCBUs and 35% of LNUs in England use probiotics (FIGURES 2 and 3). The majority (60%) of NICUs currently use probiotics (FIGURE 4). 66% of neonatal units use Labinic (FIGURE 5).

TABLE 1 Probiotic use in England across the three levels of neonatal units.
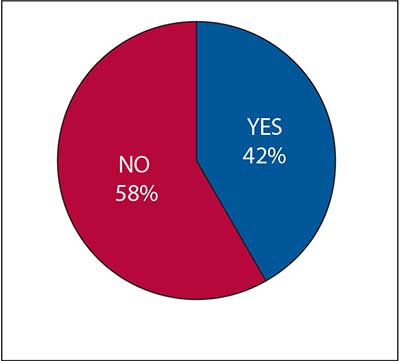
FIGURE 1 Probiotic use in neonatal units in England.
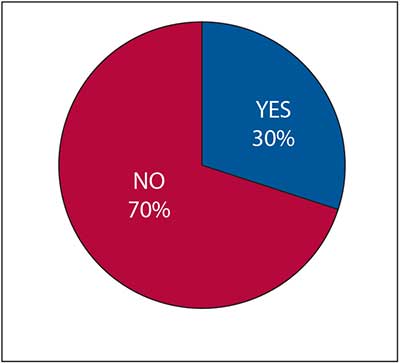
FIGURE 2 Probiotic use in SCBUs in England.
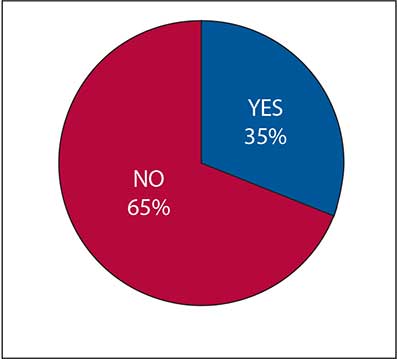
FIGURE 3 Probiotic use in LNUs in England.
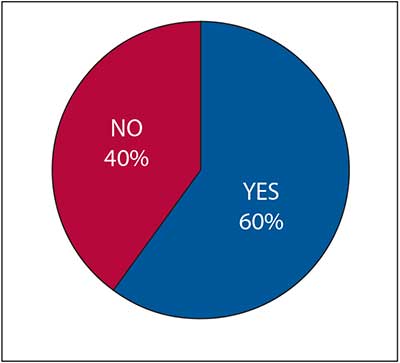
FIGURE 4 Probiotic use in NICUs in England.
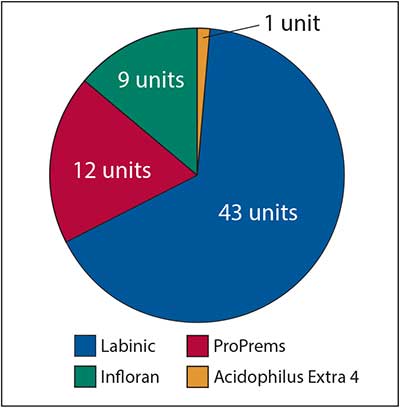
FIGURE 5 Probiotic brands used in neonatal units across England.
Among those units that use probiotics, 27 units (41.5%) have used them for less than one year, 30 neonatal units (46.1%) between one and five years, and only eight units (12.3%) have used probiotics for more than five years. Among the units not using probiotics, five have plans to commence soon (two units are currently drawing up guidelines, one has probiotics on trial and two are set to start, awaiting probiotic supplies).
Next steps
We plan to complete a UK-wide survey that will include neonatal units in Scotland, Wales and Northern Ireland.
Conclusions
The survey findings may help units to evaluate their stance on the use of probiotics. They may also help to inform appropriate agencies of the need to formulate guidance at a national level. Getting It Right First Time (GIRFT) - Neonatology identifies the use of probiotics in neonatal units as good practice.10 As far as we can ascertain, there are no guidelines or a position paper on probiotics from the British Association of Perinatal Medicine (BAPM).
From the conversations we had with neonatal unit staff during the survey, we identified that it is possible that uncertainties surrounding strain selection and lack of national guidance could be contributing to poor uptake in some units.
What was already known on this topic:
- The benefits of probiotics in neonates have been extensively investigated for nearly 30 years.
- Many recent studies have shown that probiotics may reduce the risk of NEC, LOS and mortality.
- It is likely that probiotic use in neonatal units has increased recently, but there are no data on current use in England.
What this study adds:
- Probiotic use in English neonatal units is still low; only 65 out of 155 neonatal units (42%) in England use probiotics.
- Probiotic uptake is better in NICUs (60%) compared to LNUs (35%) and SCBUs (30%).
- There is wide variation in the brand and strains used.
- Uncertainty about optimum strain selection and a lack of national guidance may be hindering uptake in neonatal units.

Walsall Manor neonatal unit team members, from left: Consultant Paediatrician and Neonatal Clinical Lead Dr Ashok Karupaiah, Senior Sister Emma Hackwood, Senior Advanced Neonatal Nurse Practitioner Simone Baller-Ghent, Matron Lisa Poston and Locum Consultant Paediatrician Dr Abdulhakim Abdurrazaq.
Author contributions and acknowledgement
The authors would like to thank all colleagues who kindly responded to the survey and provided data on probiotic use in their units. Sincerest thanks to Dr Raghu Krishnamurthy and Dr Anurada Subramaniem for their assistance with reviewing the manuscript.
Author contributions: AK is the author of this paper and responsible for conceptualising the survey, writing, editing and reviewing the content. AK also contributed to the conduct of the survey. AA and JQ conducted the survey. AA analysed the results of the survey.
Or read this article in our
Tablet/iPad edition
- Uptake of probiotics in neonatal units across England continues to be low, especially in special care baby units and local neonatal units.
- It is possible that uncertainties around bacterial strain selection and a lack of national guidance could be contributing to poor uptake in some units.
Also published in Infant:
