

Non-pharmacological management in neonatal abstinence syndrome: an overview
Substance misuse continues to be a significant problem during pregnancy and is on the increase. Consequently, neonatologists are encountering an increasing number of infants born with symptoms of neonatal abstinence syndrome (NAS). Non-pharmacological measures are an effective means of managing infants with NAS and should be used in the first instance, however, most neonatal units do not have a guideline describing the non-pharmacological pathway, which is centred around promoting maternal involvement in care, minimising stimuli and increasing staff education. We outline the important aspects of non-pharmacological management of infants with NAS to encourage soothing strategies prior to the use of medications.
Raju Sunderesan
Consultant Neonatologist
University Hospital Crosshouse,
Kilmarnock, Scotland
raju.sunderesan@aapct.scot.nhs.uk
Christopher Cox
Senior House Officer
Taranaki Base Hospital, New Plymouth,
New Zealand
Sunderesan R., Cox C. Non-pharmacological management in neonatal abstinence syndrome: an overview. Infant 2023; 19(3): 105-10.
Neonatal abstinence syndrome (NAS) is a multi-system constellation of symptoms in newborns withdrawing from physically addictive substances taken by their mother during pregnancy. This was first documented in 1969 by Loretta Finnegan, a paediatrician from Philadelphia who later went on to develop the original Finnegan scoring system.
NAS has become an ever-growing problem worldwide as the number of drug users has increased several-fold to an estimated 269 million. Opioid and cannabis use in pregnancy have quadrupled and doubled, respectively, in the USA in just 15 years.1 Patrick et al reported a NAS prevalence rate of 2.7 to 5.8 per 1,000 live births in the USA with
an overall estimated hospital cost of $1.5 billion.2
NAS rates have been increasing in developed countries. The UK has the largest reported opioid-using population in Europe and in Scotland, deaths from opiate overdose have doubled in the last decade.3 Between 2012 and 2017, the incidence of NAS across neonatal units in England increased from 1.49 to 1.91 per 1,000 live births resulting in an estimated cost of over £60 million during this period. Nearly half of infants with NAS received pharmacotherapy and their stay in the hospital was three times longer than the infants who did not require treatment.4
Non-pharmacological management of NAS is poorly standardised and many neonatal units do not have a guideline covering this aspect of care. Infants requiring pharmacological care are often nursed separately from their mothers in the busy environment of the neonatal unit, which places significant barriers to many of the simple measures to treat NAS.
Methods
We conducted a PubMed database and Cochrane Library search using combinations of the following terms: neonatal abstinence syndrome, rooming-in, lighting, skin-to-skin, swaddling, breastfeeding, sound and music. We also searched the reference lists of the relevant retrieved articles and local guidelines. Our search included papers examining the incidence of NAS, causative agents, non-pharmacological interventions and long-term outcomes.
What drugs cause NAS?
The association between NAS and opiate use is well documented and the majority of exposed infants will develop withdrawal symptoms, typically in the first 48-72 hours of life.5
Methadone programmes have been the standard of care in mothers with opioid use, though recent studies have shown that buprenorphine is also an effective treatment option.6 Buprenorphine has the advantage of being more cost effective and has less potential for abuse. However, it exerts a weaker effect at opioid receptor sites because it is a partial agonist. Methadone or buprenorphine treatments provide benefit in terms of better engagement with obstetric care, reduced polydrug use, decrease in intrauterine growth restriction and prematurity.
Studies have shown that high maternal methadone dose increases the risk of NAS symptoms with every 5mg increment increasing risk of symptoms by 17%.7 The severity and duration of withdrawal symptoms can also be influenced by exposure to other substances, including tobacco. A large cohort study of women showed that co-prescription of psycho-tropic medications (antidepressants, antipsychotics, gabapentin and benzodiazepines) alongside opiates increased the risk of NAS. Gabapentin had the greatest effect with a 1.61 relative risk ratio. Combination of two or more of these drugs increased the risk two-fold.8
There are many variables that impact the onset and duration of NAS symptoms including:
- type of substance
- dose
- time from administration to delivery
- concomitant use of other substances.
TABLE 1 shows common drugs implicated in NAS as well as the associated window of onset and length of symptoms.5
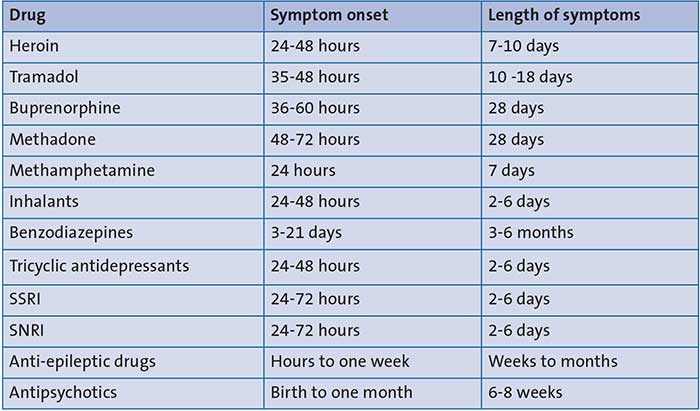
TABLE 1 Common drugs implicated in NAS, window of onset and length of symptoms.
Key: SSRI=selective serotonin reuptake inhibitors; SNRI=serotonin and noradrenaline reuptake inhibitors.
Selective serotonin reuptake inhibitors (SSRI) are the most common type of antidepressant used in the UK. They include fluoxetine, sertraline and citalopram. These inhibit reabsorption of the neurotransmitter serotonin into the presynaptic cleft and are preferred due to their limited side effect profile. Serotonin and noradrenaline reuptake inhibitors (SNRI) are similar to SSRIs but in addition block reuptake of noradrenaline, theoretically making them more effective. These include desvenlafaxine, duloxetine, levomilnacipran and venlafaxine. Both classes cross the placenta and NAS has been found in up to 30% of exposed infants.9 Symptoms are thought to be caused by serotonin excess and prevalence is similar in both drug classes despite the dual-blockade of SNRIs.
Symptoms
The many symptoms of NAS are caused by dysfunction of the central and autonomic nervous systems and can be broadly categorised as shown in FIGURE 1.
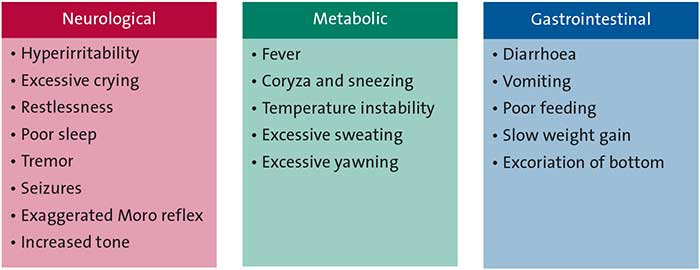
FIGURE 1 Symptoms of NAS.
Scoring
Although there are multiple scoring systems available, the modified Lipsitz and modified Finnegan scores are commonly used in the UK. The modified Finnegan score is a more complex and resource-intensive method as it is scored every 2-4 hours. Scoring commences two hours after birth and is performed 30 minutes after feeding. Infants scoring >8 on two or more occasions or more than 12 on one occasion, are considered for pharmacological treatment.
Modified Lipsitz scoring is relatively simple and is first carried out 12 hours after birth and every 12 hours thereafter with scoring taking place one hour after feeding. A baby scoring >5 on two or more occasions meets the criteria for pharmacological treatment.
Due to the qualitative nature of NAS scoring systems, it is not uncommon to find discrepancies in the scores from the maternity ward to the neonatal unit. Hence, educating staff and having a consistent method of scoring is crucial.
Management
Diagnosis of NAS can be stressful for the parents as there is worry that they may be seen as unsuitable guardians and lose custody of their child. Poor communication can cause parents to feel excluded, thus leading to anxiety and further disconnection with staff. It is important that parents are well aware of the diagnosis and are a part of the management plan. It is also important that the initial management of infants showing signs of withdrawal focuses on supportive care. The goal is to facilitate positive parenting, mother-baby bonding and nursing in a low stimulus environment. Effective non-pharmacological care offers the potential to reduce the need for medications, minimise separation of mother and infant and reduce the length of their hospital stay.
There is a lack of well-designed randomised clinical trials (RCTs) examining non-pharmacological management. A 2017 prospective study of 287 infants demonstrated a sustained reduction in average length of stay by implementing a bundle of non-pharmacological measures.10 A summary of interventions is shown in FIGURE 2 and explored in the following sections.

FIGURE 2 Non-pharmacological interventions.
Rooming-in/family-integrated care: the mother as part of treatment
Empowering the mother as principal caregiver and building her confidence is key to success in managing babies without medications. However, this is very much dependent on infrastructure as the neonatal unit may not have the capacity to accommodate both mother and baby in a single room. Even in an open bay setting, every effort should be made to offer privacy. The strategy of ‘mothers as treatment’ not only benefits the baby but also boosts the mother's self-esteem.
Rooming-in is not a new approach to the management of NAS; this model of care has been successfully deployed in Vancouver since 2001. It was designed to increase family involvement and is becoming more recognised as a standard of care. Maternal presence alone has been shown to decrease severity of NAS and result in fewer treatment days.11 A study by Newman et al showed that infants who roomed-in with their mothers had a decreased need for pharmacological treatment; down from 88.3% to 14.3%.12
It has also been found that breastfeeding increases following rooming-in and maternal custody is more likely.13
Supporting and encouraging the parents to take a prominent role in learning and caring for their babies with NAS will enable parents to be better prepared for the transition to home life and is essential for family-centred care. Wachman et al emphasise the importance of the parents’ presence for consoling their baby, rather than starting pharmacological treatment.14
Lighting
The visual system is the last sensory system to develop in infants and it is not accelerated following preterm birth. Before 32 weeks’ gestation, the eyelids are thin and there is little or no pupillary constriction to control the amount of light entering the eye. The pathways from the retina to the visual cortex become functional at 39-40 weeks.
The American Academy of Pediatrics recommends that ambient illuminance levels in the neonatal intensive care unit (NICU) are maintained between 107-215 lux. For tasks requiring greater detail, light levels should be increased only for that infant and should not exceed 2,000 lux for greater than 2% of the time. Light levels inside incubators can be reduced as low as 9 lux when an opaque cover is placed across the top. Studies have shown that ambient lighting reduces stress and cortisol levels as well as promoting extended sleep.15
Current practice varies between neonatal units, ranging from cyclical 12-hour day/night regimes, continuously dimmed lighting and extended phases of dim lighting. Most studies into the outcomes of lighting in the NICU are on preterm infants. There is growing evidence of the importance of circadian rhythms for short- and long-term neonatal health, although studies into cycled light vs continuous dimming have been equivocal.16 Bright lights can be uncomfortable and can further unsettle babies with NAS, which in turn can translate into higher NAS scores necessitating pharmacological treatment. The current consensus for management of infants with NAS is to reduce stimuli by nursing in a quiet, dark space. Strategies to reduce light exposure include individualised lighting at each cot space, dimmer switch control, incubator covers, cot canopies and eye bands (FIGURE 3).

FIGURE 3 Neonatal unit lighting – note the individualised lighting and large, thick incubator covers to reduce ceiling light exposure and prevent direct light reaching the baby’s face.
Breastfeeding
Breastfeeding is another key component of non-pharmacological care. We are all well aware that breastfeeding has multiple benefits for both the mother and infant, including improved maternal and infant bonding, reduced severity of withdrawal from drugs and decreased use of pharmacological therapy. The main challenge healthcare professionals face is the lack of evidence-based guidelines for mothers with substance use who wish to breastfeed. Hale’s Drugs and Lactation Database17 is a good resource to ascertain the safety of substances taken during pregnancy.
NAS occurs due to sudden cessation of the supply of psychoactive substances from the placenta. Most causative substances are secreted in breast milk, hence breastfeeding leads to continued exposure for the infant after birth. Studies have shown that breastfeeding in opioid-dependent mothers reduces the need for treatment.18 As discussed, methadone maintenance has been the treatment of choice for pregnant women with opioid dependence. There is evidence to support that there is a reduction in the severity of symptoms and duration of treatment of NAS when mothers on methadone maintain breastfeeding.19 Studies have shown that methadone concentrations found in breast milk are low and the American Academy of Pediatrics encourages breastfeeding for mothers on stable doses of methadone.18
Although the terms cannabis and marijuana are used interchangeably, they do not mean exactly the same thing. Cannabis refers to all products derived from the plant Cannabis sativa, however marijuana refers to parts of or products from the plant C. sativa that contain substantial amounts of tetrahydro-cannabinol (THC). Although THC is excreted into breast milk in small quantities, it has a long half-life and can remain in breast milk for up to six weeks. When cannabis is smoked, levels of THC peak at around 1-4 hours, however, the amount of THC the baby gets is very variable and can be up to about 10% of the weight-adjusted maternal dosage.17,20
Bertrand et al analysed breast milk samples for THC from 50 women who reported using cannabis in the previous 14 days. Although THC was detectable in 66% of the breast milk, no adverse outcomes were noted in postnatal growth or neurodevelopment of the infants.21
Cocaine, on the other hand, is one of the few drugs that is regarded as a relative contraindication to breastfeeding.22 Mothers who regularly use cocaine should not breastfeed; however, mothers who occasionally use cocaine should leave at least 24 hours (pumping and discarding breast milk) between the last use of cocaine and either breastfeeding or expressing breast milk.17,18
The UK guidance on drug misuse and dependence, published in 2017, encourages breastfeeding even if the mother continues to use drugs, except where she uses cocaine or crack cocaine, or a very high dose of benzodiazepines.20,22
Skin-to-skin kangaroo care
Skin-to-skin care is a readily available non-pharmacologic intervention for managing NAS, with the potential to reduce symptoms and encourage a positive parent-infant bond. Studies have shown the effectiveness of skin-to-skin care in improving physiologic stability and sleep when skin-to-skin care is initiated one hour post feed.23
A Cochrane review pooled 46 randomised trials from 21 countries. Although the methodological quality of the trials was suboptimal, results support the use of skin-to-skin care to promote breastfeeding. Mothers who practised skin-to-skin care were more likely to breastfeed longer compared to mothers who received routine care.24
As well as proven health benefits, skin-to-skin care can help to keep the baby calm and empower the mother as a caregiver.
A mother that may feel marginalised from her child’s care can give her baby her undivided attention to help build her confidence in her ability to care for her baby. In this way, skin-to-skin care contributes to the philosophy of ‘mothers as treatment’, offering the opportunity to bond and practise caring for the baby.
Swaddling
Swaddling is an ancient practice of firm wrapping to calm infants. Traditional swaddling employs a tight restrictive wrap, which tends to completely immobilise the infant. Nowadays, light, breathable blankets are recommended to comfort infants. Swaddling can provide a gentle, soothing environment with minimal stimulation; it can be a good way to calm and soothe an irritable infant suffering from withdrawal.25,26 Swaddling helps to maintain continuous and adequate body positioning to provide a stable sleep environment and encourage muscle tone; it can help to minimise tremors and jerks. Infants typically like to be swaddled for sleep, but infants with NAS may benefit from being swaddled for longer periods.
Skin care
Babies who develop NAS are more prone to skin injury as they display hyperirritability that results in excessive and uncontrolled motor movements; rubbing of the skin leads to excoriation. Areas which are prone to this are the chin, cheeks, elbows, the back of the head and other exposed sites. Non-pharmacological interventions for infants with NAS help prevent skin injuries by reducing neurological irritability.27
To prevent napkin dermatitis, it is vital to maintain suitable skin care of the perianal area through frequent nappy changes and appropriate treatment as per hospital guidelines. Breast milk can lower the pH of both urine and faeces therefore improving the overall pH of the skin, which in turn helps to prevent napkin dermatitis.28
Sound
Although exposure to sound is crucial for fetal sensory stimulation, intense sound can have adverse implications for the developing brain resulting in physiological instability and behavioural problems.29 A 2020 Cochrane review found that noise can cause a significant stress response in neonates including alterations in blood pressure, heart rate and oxygen saturations.30
The Sound Study Group recommends that pregnant women should avoid prolonged exposure to low-frequency sound levels (<250Hz) above 65dB. According to the American Academy of Pediatrics, average hourly noise levels in neonatal units should not exceed 45dBA. Maximum noise levels, regardless of duration, should not exceed 65dBA.31 To put this into context, whispering is around 30dB and normal conversation around 60dB. Reports of sound levels in NICUs range from 50-89dB with peaks of 105dB.
Reducing noise levels in the NICU
Noise reducing measures in the NICU can be very effective, for example:
- quieter conversations
- desk phones on mute with only a flashing light to indicate incoming calls
- quieter equipment – attending to monitor alerts promptly
- walls and ceilings made of sound absorbent materials
- earmuffs/plugs and sound-absorbing fabrics placed over incubators.
In a RCT studying the effects of silicone earplugs in 34 very low birth weight infants, the intervention group showed higher rates of passing the auditory brainstem response test and better Bayley II mental development index scores at 18-22 months.32 Although there is insufficient data on the effect of sound in infants with NAS, it is hypothesised that reducing stimulation and sensory overload by this means would be worthwhile.
Music therapy
The use of music therapy for infants in the NICU is gaining recognition as a non-pharmacological intervention that is beneficial to infants as well as to their families.33-35 Music therapy and lullaby singing has been used to calm infants during painful procedures, reinforce sucking during feeds and mask background noise in the intensive care environment.
Lullabies have been shown to promote relaxation in infants as they are generally slow, repetitive and melodically simple. Chorna et al from Vanderbilt University, Tennessee, conducted a randomised trial to test the hypothesis that the mother's voice played through a pacifier activated lullaby (PAL) device (FIGURE 4) during non-nutritive sucking would promote more effective oral feeding in preterm infants. The PAL is a US Food and Drug Administration-approved device with a pressure-sensitive sensor that activates the playing of a lullaby in direct response to sucking as a positive reinforcement to the infant (the PAL is only authorised for sale in the USA). Ninety-four preterm infants completed the study. They received five 15-minute sessions daily of either PAL with their mother's recorded voice or no PAL, along with routine non-nutritive sucking. The intervention group had significantly increased oral feeding rates and faster time-to-full oral feeds compared with the control group.36 In a further study, Detmer et al included 22 infants with NAS receiving morphine treatment. Infants assigned to the music arm received three, 10-minute PAL therapy sessions within 30 minutes of a feed, starting on the first day of admission until the infant’s first day of morphine weaning. Infants that received music therapy via the PAL required shorter morphine treatment with a lower dose and had an overall shorter length of hospital stay.37 Similarly PAL has been used to reinforce non-nutritive sucking and soothe infants with NAS. Lullabies and white noise (a combination of all of the different frequencies of sound) have been used to help encourage sleep in neonates.38

FIGURE 4 The pacifier activated lullaby device (permission obtained from Powers Medical Devices LLC, Florida, USA).
A randomised trial is underway at Mount Sinai Hospital, New York, where researchers are exploring the effect of live music therapy interventions on the calming, stabilising and development of infants of >28 weeks’ gestation with NAS. Infants will receive six music therapy sessions over a two-week period. The outcome measures will look at activity levels, sleep states, feeding (sucking and absorption), NAS scores and parental postpartum bonding feedback.39
The ‘eat sleep console’ model of care
Grossman et al developed and introduced the ‘eat sleep console’ (ESC) model of care in 2015.40 This family-centred approach emphasises increased parental involvement, feeding on demand, consoling when the baby is irritable and letting it sleep as much as possible between feeds. ESC focuses on three key areas:
- Eat: is the baby feeding normally?
- Sleep: is the baby able to sleep between feeds?
- Console: can the baby be comforted?
If the baby feeds well, sleeps for >1 hour and can be consoled within 10 minutes, it is considered well managed and no further intervention is required. Pharmacologic treatment is only considered when all the other non-pharmacologic interventions are in place. Grossman et al demonstrated that only 12% of infants required pharmacotherapy using the ESC method compared to 62% with the standard Finnegan NAS scoring approach. Similarly, Hein et al (2020)41 and Miller and Willier (2021)42 showed a sizable reduction in the number of infants who required pharmacotherapy using the ESC method. The ESC model has since gained acceptance among neonatal units in the USA. Studies have demonstrated positive impact overall with the ESC method in regards to the length of hospital stay and cost of treatment, however, further insight is needed in terms of long-term outcomes.
Learning points and conclusion
NAS is a growing problem with significant short- and long-term adverse outcomes for neonates. Although most commonly associated with opioid exposure, it can be caused by a wide range of recreational and prescription drugs. Standardised scoring should be carried out for at-risk infants using a model such as the modified Lipsitz, Finnegan score or ESC. Traditional management has relied on lengthy hospital stays and pharmacological treatment using medications, which themselves pose significant risks.
Data suggest that use of non-pharmacological methods improves outcomes for babies with NAS and reduces the length of hospital stay and use of pharmacological treatments. Making the mother-infant dyad a priority is key to this model of care.
FIGURE 5 shows the main take home messages for non-pharmacological management of infants with NAS. The foundations of management are to:
- promote bonding between the mother and baby
- encourage skin-to-skin care and breastfeeding
- practise cluster care
- decrease environmental stimuli.
Much of the current research either examines bundles of non-pharmacological treatments (rather than individual techniques) or does not look specifically at a NAS population. However, the evidence suggests that breastfeeding, skin-to-skin care and rooming-in are beneficial to infants. Further RCTs are required, particularly to clarify the optimum lighting, sound environment and swaddling of infants with NAS.

FIGURE 5 Learning points.
Acknowledgements
The authors would like to thank Ashley Manchester, Staff Nurse, University Hospital Crosshouse, for assistance in developing the pictures. Thanks also to Natalie McLennan-Murray, Regional Medicines Information Pharmacist, Midlands, for providing information about drugs and breastfeeding.
Author contributions
RS conceived the idea for the article. RS and CC performed the literature review, drafted the manuscript and critically revised it.
Or read this article in our
Tablet/iPad edition
- Non-pharmacological interventions should be the cornerstone for management of infants with NAS. Such methods show improved outcomes for babies and reduced length of hospital stay and use of pharmacological treatments.
- Non-pharmacological interventions are easy to implement and cost effective. Staff education is an integral part of management.
- Empowering the mother as principal caregiver is key to the success of managing babies without medications.
- Pharmacotherapy should be reserved for infants with severe NAS.
Also published in Infant:
