

A multidisciplinary approach to the implementation of non-pharmacological strategies to manage infant pain
Newborn infants, both term and preterm, endure many painful procedures when receiving treatment on a neonatal intensive care unit. Unmanaged neonatal pain can have a negative influence on short- and long-term neurodevelopmental outcomes and can also impact on parental wellbeing. While clinicians are aware of the efficacy of non-pharmacological strategies to reduce pain, these are not always implemented into neonatal care. This article summarises efforts made by a multidisciplinary team to improve the use of non-pharmacological approaches in the management of infant pain during procedures on a level 2 neonatal unit
Emily Hills
Clinical Specialist Neonatal Occupational Therapist, Imperial College Healthcare NHS Trust
James Rosenberg
Neonatal Consultant, Starlight Neonatal Unit, Royal Free Hospitals NHS Foundation Trust
Natalie Banfield
Neonatal Staff Nurse, Starlight Neonatal Unit, Royal Free Hospitals NHS Foundation Trust
Celia Harding
Honorary Professor, City University of London and Neonatal SLT, Royal Free Hospitals NHS Foundation Trust
It is estimated that around 90,000 infants born each year in the UK require specialist hospital care.1 While receiving hospital care, term and preterm infants may experience medical procedures, many of which are painful. Coughlin2 suggests that all healthcare practitioners who work with neonates have an ethical obligation to prevent pain. There are some neonatal pain management guidelines identifying the use of non-pharmacological strategies to reduce pain (eg American Academy of Pediatrics3). Recent evidence in the literature promotes the use of breast-feeding, skin-to-skin contact and sucrose to minimise pain, however while clinicians are aware of the efficacy of non-pharmacological strategies to reduce pain, it has been shown that these strategies are not always implemented into neonatal care.
Pain in neonatal care
Historically it was thought that newborn infants were incapable of experiencing pain, although it is now known that this is not the case.4 Unmanaged pain has an immediate impact on a neonate’s behav-ioural and physiological development.5 In hospital, preterm infants can experience up to 12 painful procedures each day and less than half of these interventions use pain management.6 Often pain is untreated in neonatal units7 despite electrophysiological evidence suggesting that acute pain results in diffuse brain activation for preterm infants, with region specific alterations in the lateral thalamus and thalamocortical pathways in extremely preterm infants.8,9 Managing neonatal pain is important as repeated pain and stress can have a lifelong impact on the infants themselves and on parental wellbeing.4,10 The best pain management strategy is to try and prevent pain if possible, or minimise the intensity of the pain when carrying out a procedure.
There are pharmacological and non-pharmacological interventions available to enable practitioners to manage infant pain. Non-pharmacological interventions are cost effective and can be easily integrated into neonatal care by a range of neonatal practitioners.11
Thematic analysis of the literature
Reviews of the literature have identified the following non-pharmacological strategies as being effective in pain management:
- skin-to-skin opportunities12
- use of sucrose13
- experiencing breastfeeding or having breast milk14
- use of non-nutritive sucking, swaddling, tucking, rocking and holding.15
Further investigations of the literature highlight five key themes that are important in relation to infant pain management:
- Involving parents. Parents need to be directly involved as they are aware of their infant’s pain16 and they also have a desire to alleviate pain.17 Parent participation and involvement in developing pain management strategies is best achieved through a collaborative approach.18 Parents need to be valued as advocates for their infants, rather than a disruptive influence.19
- Improving awareness of pain management by discussing it. For clinical practice to change in the management of infant pain, communication within the team is essential.18,20 Projects that involve healthcare practitioners and parents working together have the most effective outcomes.18 Limitations in the communication used between healthcare practitoners and parents can produce a sense of unease, leading to limited implementation of important pain management approaches.19
- Educating staff and parents. To implement non-pharmacological strategies into neonatal care there need to be key dedicated individuals on the unit who can promote these and encourage others to use them.21 To ensure all practitioners are aware of the rationales underpinning the approaches, an appreciation of the diversity of staff and parent learning styles is essential.22 Practical education sessions can support linking theory to practice.23
- Providing resources to enable practice of pain management strategies. Visual resources such as posters and brochures that are readily available can help enhance education.16 Pain champions can ensure strategies are taking place in practice.24 Despite these positive elements in promoting pain management there are barriers to overcome, such as reduced nurse-to-infant ratios21
- Involving and informing the whole organisation. A whole unit approach with active collaboration from all levels of practice, including management, is necessary to implement non-pharmacological strategies to minimise infant pain.16,23 It is stated that implementation of changes in practice can take between three and five years to allow for neonatal culture and practice alterations.25
Exploration of practice on a level 2 neonatal unit: methods
This project took place in a level 2 neonatal unit in north London – Starlight neonatal unit, Barnet Hospital. This unit has 30 cots, of which six are intensive care, 10 are high dependency, four are special care cots, and 10 are individual care rooms. The hospital the unit is in has approximately 5,800 deliveries per year. It is the third busiest neonatal unit in NHS England. Staff from the unit met in December 2017 and agreed to review pain management on the unit.
The literature was discussed as a team, with general agreement that good pain management was necessary to ensure the best possible long- and short-term outcomes for infants. A four-phase quality improvement project was implemeted that:
- supported staff and parents to understand neurobehavioural infant cues and non-pharmacological strategies
- used a pain assessment tool
- provided pain management gudelines regarding non-pharmacological methods when working with infants.
The pain project was scheduled to take place from January 2018 to January 2019. Two observation audits were undertaken at the beginning of the project to observe what staff did to minimise infant pain during immunisations, lumbar punctures, blood tests, nasal prong adjustments, nasogastric tube re-insertion, cannulation and eye testing. Observation findings were discussed during training sessions.
Staff received education about pain management throughout the 12-month period and filled in the same questionnaire twice to test their knowledge and to identify changes in views about using non-pharmacological approaches at two time points during 2018 (February and December). Specifically, staff answered questions about neurobehavioural cues and support for parents; practice knowledge and beliefs, and confidence with non-pharmacological pain management strategies (ie skin-to-skin, non-nutritive sucking, breastfeeding/ breast milk, use of sucrose, etc).
Parents were informed that a pain audit and training were taking place on the neonatal unit. They were invited to participate in education sessions during ‘supper club’ including a video about minimising infant pain while their infants were on the unit. Parents also had cotside information sharing and training. They were asked for feedback about how their infant’s pain was managed after discharge from the unit.
Outcomes
The two early observation audits high-lighted that seven non-pharmacological strategies were used by staff; these are outlined in TABLE 1. It is interesting to note that during the second observation, no skin-to-skin, breastfeeding or use of expressed breast milk strategies were used. In addition, parents were not always present when painful procedures were undertaken.
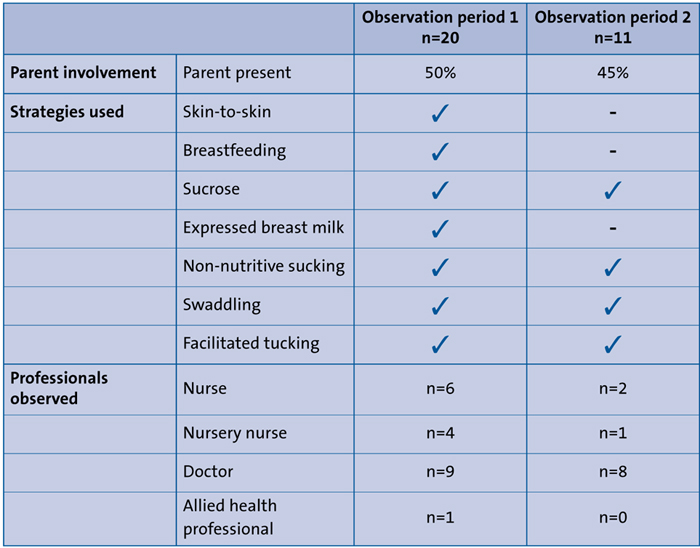
TABLE 1 Procedures used during initial observation periods.
At time point 1 (TP1, February 2018), 33 staff completed the questionnaire, and at time point 2 (TP2, December 2018), 21 staff completed it. Age of participants at both time points ranged from 25-64 years of age. A wide range of neonatal practitioners completed the questionnaires at both time points. At TP1, 47% were nurses, 41% were doctors, 9% were allied health professionals, and 3% were classified as ‘other’. A similar profile of staff was noted at TP2, with 47.5% nurses, 42.5% doctors and 10% allied health prof-essionals. The experience of participants was recorded, so at TP1, 48% had five years or less experience with neonates, with 32% having over 15 years neonatal experience. At TP2 30% had five years or less neonatal experience, and 33% with over 10 years’ experience.
Participants were asked about neuro-behavioural cues and working with parents and the relevance of this to working to minimise pain within infant care. A five-point rating scale was used, from ‘strongly agree’ to ‘strongly disagree’. At TP1 64% strongly agreed that infants were able to communicate non-verbally in contrast with TP2 where 75% strongly agreed that infants were able to communicate non-verbally. In relation to involving parents in infant pain management, at TP1 42% strongly agreed that parents should be involved in pain management procedures, in contrast with TP2 where 50% strongly agreed that parents should be involved in pain management procedures.
Participants were asked to rate statements related to their knowledge and beliefs about infant pain management. At TP1 88% strongly agreed that neonates could experience pain compared with TP2 where 79% strongly agreed. Regarding minor procedures 82% strongly agreed that even minor procedures could cause pain at TP1, and this view was similar at TP2 with 83% stating that they strongly agreed. There was an increase in the strongly agreed category between the two time points that poor pain management could increase the risk of neuro-developmental problems (a change from 70% to 80%).
Participant knowledge about pharmacological and non-pharmacological interventions to manage infant pain was considered with 30% strongly agreeing that non-pharmacological interventions were effective at TP1, increasing to 54% at TP2. Overall, participants identified a range of non-pharmacological approaches for infant pain management as listed in TABLE 1. At TP1, 9% strongly agreed that skin-to-skin was an effective non-pharmacological strategy in contrast with 36% who strongly agreed that sucrose was effective. At TP2, 4% strongly agreed that skin-to-skin was an effective strategy in contrast with 63% who strongly agreed that sucrose was effective.
Before training, most staff reported on the questionnaire that they used breast comfort to manage pain before training, but interestingly, after training, at TP2, most reported that they used sucrose. This was not reflected in the unit observations of pain management practice where skin-to-skin, breastfeeding and use of expressed breast milk were not used on both occasions in contrast with non-nutritive sucking, sucrose, swaddling and facilitated sucking.
Parents were invited to give feedback about infant pain management once they had been discharged from the unit. Comments made by parents were favourable, as outlined in TABLE 2.
TABLE 2 Parent feedback.
Conclusions
This neonatal pain management project implemented in a level 2 neonatal unit to improve practice highlighted that although non-pharmacological interventions are often recommended, and even though staff are aware of them, they are used variably as reported by staff.26 In addition, parents were not always present for painful procedures at the beginning of the project. Further consideration needs to be given to the use of sucrose. Interestingly, the observation audits revealed sucrose use both times, with a high reporting of use of sucrose in the questionnaires, especially at TP2. Research suggests that sucrose use in infancy, when a significant amount of neuroplastic change is occuring, can be detrimental to both white and grey matter development in the brain.27 The unit has a commitment to exploring non-pharmacological approaches to minimise infant pain, and use of sucrose will be a major discussion point within the team. As the pain management project demonstrated, there remains diversity in clinical practice in methods used.28
Acknowledgements
Dr C. Cane, Dr S. Shanmugalingham, Dr T. Wickham, Dr K. Job, L. Collier, P. Chong, K. Eglinton, A. Hollings.
Or read this article in our
Tablet/iPad edition
- Newborn infants are capable of experiencing pain.
- Infants requiring specialist hospital care are likely to experience painful medical procedures.
- Unmanaged pain has a long-lasting impact on an infant’s behaviour and physiological status.
Also published in Infant:
