

Neonatal bilious vomiting: risk factors for surgical pathology
Bilious vomiting (BV) in newborn infants is an important presenting sign of intestinal obstruction. To determine the incidence and associated risk factors for surgical pathology in this population, we conducted a review of the presentation and management of term neonates with BV admitted to a neonatal intensive care unit. More than 50% of babies with BV presented within the first 24 hours but surgical pathology was more likely in infants who presented after 24 hours. Abdominal distension was a major risk factor for surgical pathology in infants with BV. Abdominal plain radiographs demonstrated a high sensitivity and specificity for predicting surgical pathology.
David A Cummins
Neonatal Consultant, Royal Jubilee Maternity Hospital, Belfast, Northern Ireland
ORCID: 0000-0002-8116-7675
Twitter: @dcumminsno9
david.cummins@belfasttrust.hscni.net
Carl A Kuschel
Neonatal Consultant, Royal Women’s Hospital Melbourne, Australia
carl.kuschel@thewomens.org.au
Cummins D.A., Kuschel C.A. Neonatal bilious vomiting: risk factors for surgical pathology. Infant 2023; 19(3): 100-04.
Bile is a luminous yellow fluid produced by the gall bladder. It drains into the duodenum via the biliary tree and is not normally present in vomitus unless forward intestinal flow is obstructed. Bilious vomiting (BV) presents clinically as green vomitus, secondary to the action of gastric acids. Surgical teaching dictates that BV is secondary to intestinal obstruction, either mechanical or functional, until proven otherwise and that BV associated with abdominal tenderness or distension requires urgent surgical assessment.1 It may be the only symptom of intestinal malrotation and catastrophic gut ischaemia and death can occur if it is not treated promptly1 with mortality as high as 4% for neonates with volvulus.2 The proportion of neonates with BV who subsequently have a surgical pathology identified varies between 20 and 50%.3-6 However, the overall incidence of BV with or without a surgical diagnosis in term infants is unknown.7
Malrotation is a congenital cause of BV with an incidence of 1:6,000 births.1 Abnormal fixation of the small bowel in malrotation can compromise the blood supply to the whole intestine as the root of the mesentery is on a thin stalk prone to twisting (volvulus), vascular obstruction and gut ischaemia.1 30% of neonates with malrotation present within 3-7 days, and 80% by one month, indicating that many cases will present after discharge from hospital.7 One study reported that 15% of term infants of <7 days old transferred by the London Neonatal Transport Service were for BV.8 An upper gastrointestinal (UGI) contrast study remains the best available radiological investigation for diagnosing malrotation with a positive predictive value of 90%,2 although ultrasonography has also been shown to be safe and reliable.9-11
We observed a high admission rate of infants with BV and reviewed their presentation, management and subsequent outcomes to determine the incidence of surgical pathologies in this population and any associated risk factors.
Methods
Design
This investigation looked at a retrospective case series. All inborn term neonates (37 weeks’ gestation or more) admitted to the neonatal intensive care unit (NICU) at the Royal Women’s Hospital Melbourne (RWH) during a five-year period between 1 January 2015 and 31 December 2019 were identified through a prospectively maintained database. Only infants with BV, defined as any green-stained vomit, were included. Clinical data were collected from the clinical records, including demographic details, feeding at presentation, age at passage of meconium, colour and number of vomiting episodes, and whether the infant was considered clinically unwell at presentation. Data were collected on radiological investigations (abdominal plain radiographs [AXR] and UGI studies), laboratory tests and the duration of antibiotic therapy. We recorded if the infant was transferred to a surgical centre for further investigation or management.
Statistical analysis
Statistical analysis was performed using Microsoft Excel version 16.37 and R Version 4.0.0 (R Foundation for Statistical Computing, 2020). Median and range were determined for non-normally distributed data, with mean and standard deviation (SD) calculated for normally distributed data. A Mann Whitney U Test was performed to compare non-normally distributed populations. This audit was approved by the RWH Human Ethics and Research Committee as a quality assurance activity AQA21/02.
Results
Clinical presentation
Over the five-year period, 33,957 term infants were liveborn in our institution. 153 infants with BV were admitted to the NICU, giving an incidence of 4.5 per 1,000 live births. 55.6% of infants were male. 66.0% had an isolated episode of BV. While there was variation in the description of the colour of the vomitus, all were documented as ‘green’. The median age at presentation was 23 hours (range = 4-168 hours). The mean (SD) gestational age was 39+4 (±1+2) weeks and mean birth weight was 3,446g (±439g). Six infants (3.9%) were readmitted after initial discharge, at a median of 59 hours (range = 32-168 hours). Five babies (3.3%) first passed meconium more than 24 hours after birth. 83.7% of babies were exclusively breastfed at presentation. The characteristics of the cohort are summarised in TABLE 1.
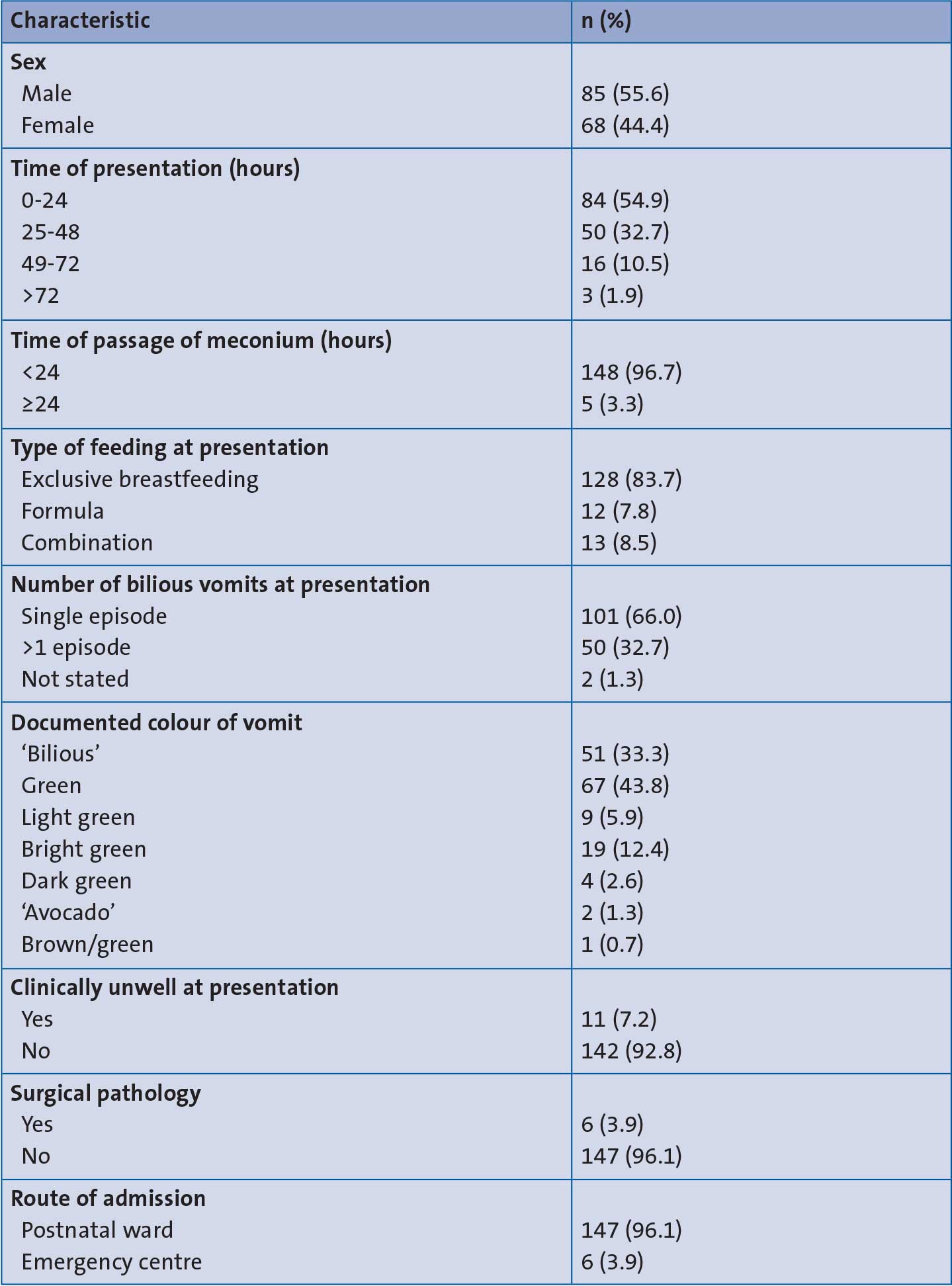
TABLE 1 The characteristics of the cohort (n=153).
Two infants were diagnosed with intestinal malrotation and four with Hirschsprung’s disease, giving a rate of surgical pathology of 3.9% of infants admitted with BV and incidence of 0.2 per 1,000 liveborn infants over this five-year period. The infants with malrotation presented at 40 and 42 hours of age. The median age of presentation in infants with surgical pathology was 40 hours (range 20-168 hours), whereas the median age in normal infants was 23 hours (range 4-96 hours, p=0.04).
Infants who required respiratory or cardiovascular support (such as fluid resuscitation) on presentation or who had an abnormal clinical examination or vital signs, were classified as ‘clinically unwell’. Eleven infants (7.2%) fulfilled these criteria, six of whom had an abnormal clinical examination and were later diag-nosed with a surgical pathology (TABLE 1). All 11 had a blood culture taken and were treated with benzylpenicillin and gentamicin for possible early onset neonatal sepsis. All six infants with surgical pathology presented with a distended abdomen.
Radiological findings
There was variation in the clinical management and investigations carried out and these are shown in TABLE 2. 83.7% underwent an AXR with 5.2% reported as abnormal. UGI contrast studies were performed in 83.7%, with 3.9% reported as abnormal. Radiological investigations and the outcomes are summarised in FIGURE 1.
Of the six infants identified with surgical pathology, all had an AXR reported as abnormal. Four were referred for a UGI with three reported as abnormal. Three babies without subsequent surgical pathology had an abnormal UGI contrast study. One had a normal diagnostic laparoscopy, one had a repeat UGI contrast study, which was normal, and the other had an AXR post UGI, which showed normal transition of contrast to the rectum, so feeds were reintroduced without any problems.
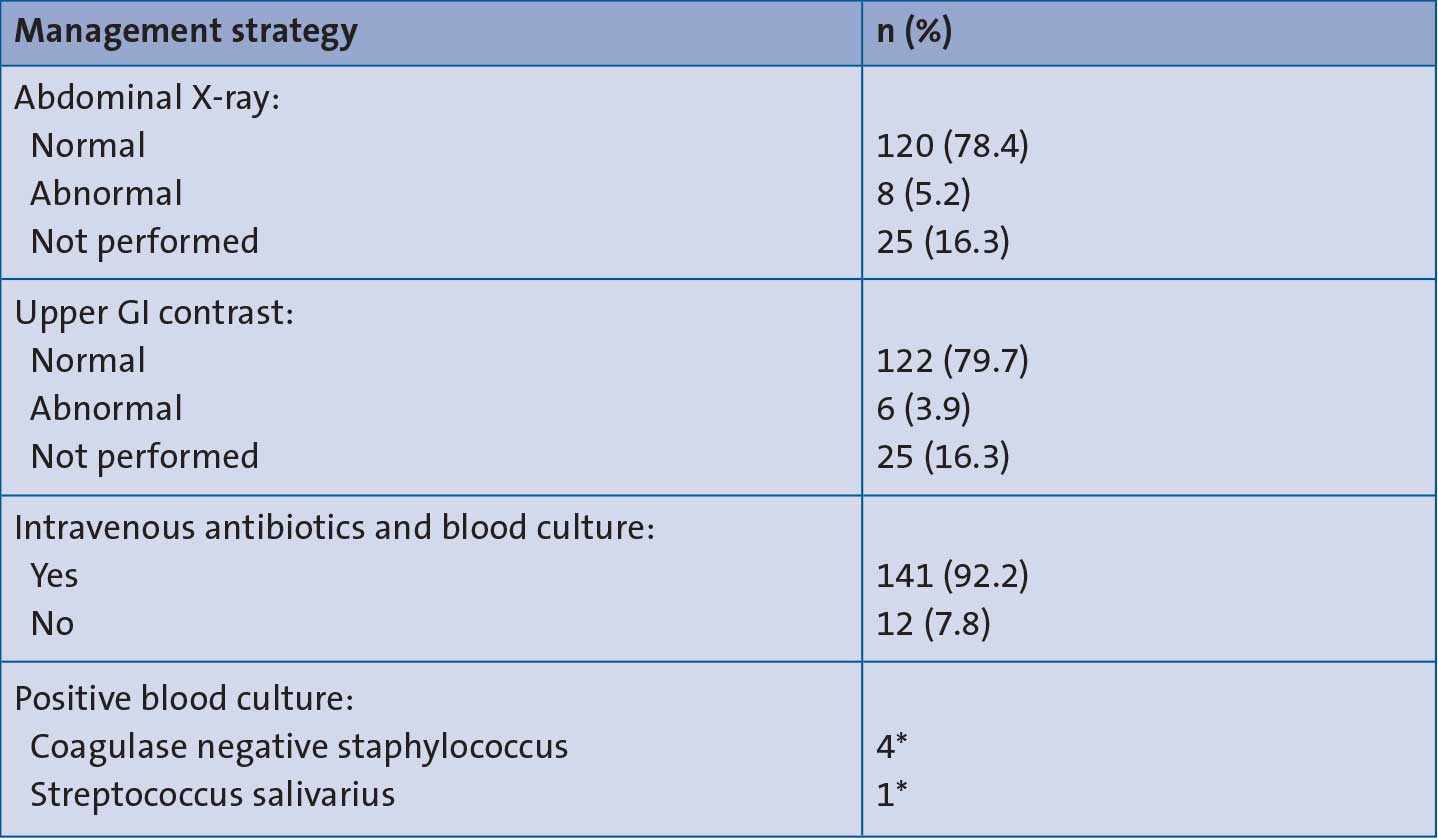
TABLE 2 The management and investigative strategies for the babies with BV (n=153).
*Note, the positive blood culture results were considered likely to be contaminated samples rather than true bacteraemia.
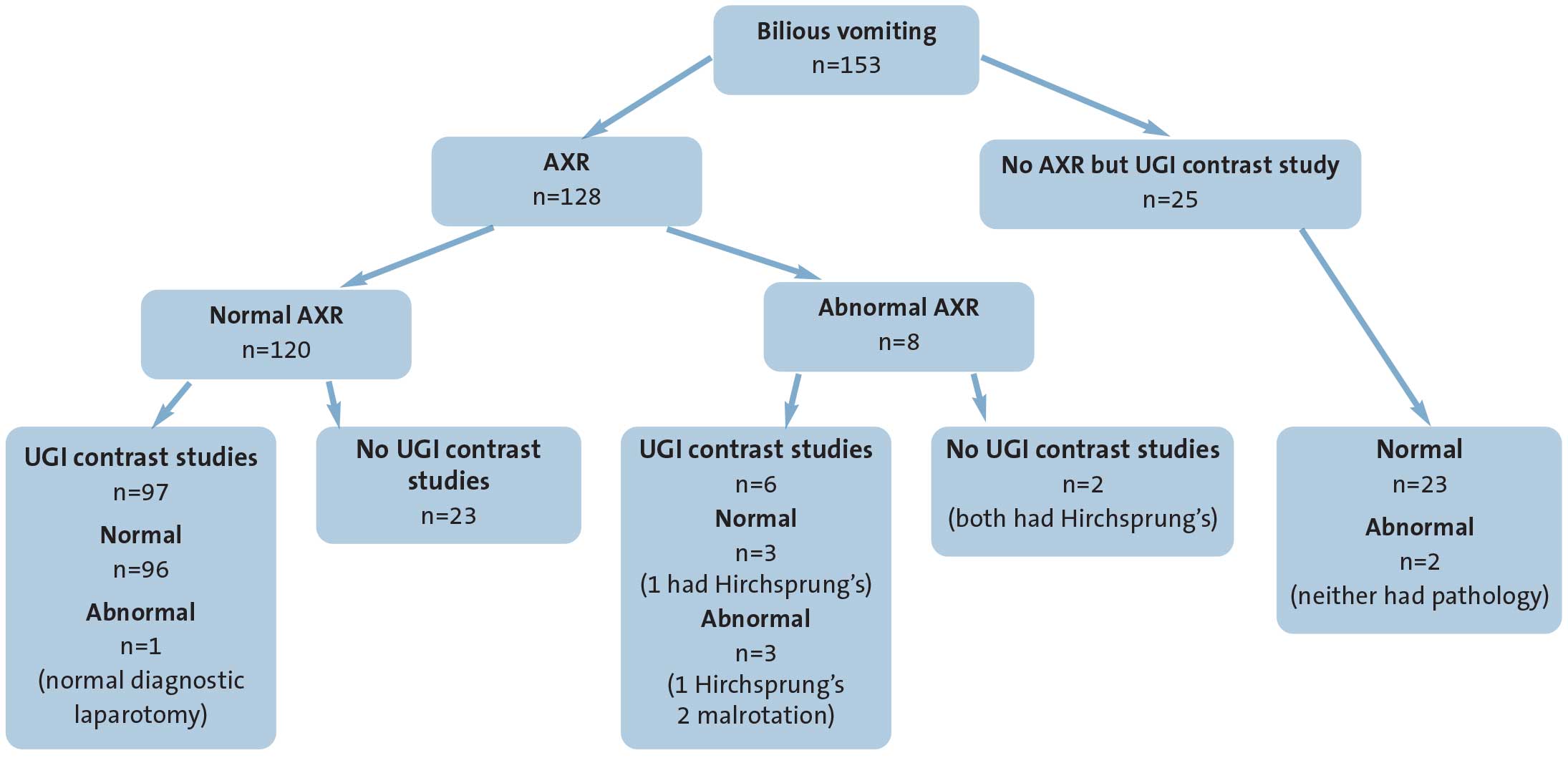
FIGURE 1 The radiological investigations and outcomes (n=153).
The sensitivity and specificity of an AXR for predicting surgical pathology were 100% and 98%, respectively, with a positive predictive value (PPV) of 75%. For UGI contrast studies, sensitivity and specificity were 50% and 97.5% with a PPV of 50%. However, both infants with intestinal malrotation were diagnosed with UGI contrast.
Some babies (n=23, 19.2%) with BV and a normal plain radiograph were not referred for UGI studies, with clinical staff appearing reassured by normal clinical and plain radiography examinations. In 18 of these babies, the BV was an isolated event and feeding was recommenced after a period of observation. None of these babies subsequently presented to the tertiary children’s hospital following discharge with further episodes of BV.
Seventy-three (47.7%) infants were transferred from our institution to a children’s hospital for further investigation or management. While a UGI study can be performed at our site, it is dependent on the availability of a radiologist. Seven of these babies (9.6%) were transferred for a surgical opinion (one abnormal UGI study at RWH; six with concerning clinical signs). The others were transferred for imaging.
Antibiotic therapy
141 (92.2%) babies had a blood culture test and were commenced on antibiotic therapy. Five of these babies (3.5%) had a positive blood culture (four coagulase-negative staphylococcus and one streptococcus species) with four receiving a treatment course of five or more days. All had C-reactive protein (CRP) above 10mg/L but none presented as ‘clinically unwell’ and the positive blood culture results were considered likely to be contaminated samples rather than true bacteraemia.
Discussion
This study describes a cohort of term infants presenting to a non-surgical perinatal centre with BV and demonstrates a low rate of surgical pathology (3.9%) compared to that previously reported in the literature (50%).3 Most paediatric surgical centres receive referrals of infants with BV for further management from a large number of non-specialist hospitals, including infants with clear surgical signs and those who are clinically unwell. This may explain the higher incidence of surgical pathology demonstrated in these studies.3-6,8 Our study was population-based from a single centre and a cohort of ‘well/normal’ term infants, therefore unlikely to have a high incidence of underlying pathology.
Clinical recognition of BV may be difficult.13 While most clinicians appreciate that bile-stained vomitus is abnormal, there can be confusion about what colour indicates bile-staining.13 The introduction of a chart including the colour of vomitus and the appropriate escalation path in our hospital identifies infants who require review (FIGURE 2). Consideration should be given to raising awareness of BV among inexperienced clinicians and midwives. Non-specialist hospitals should develop and follow standardised guidelines, in conjunction with surgical colleagues, on the investigation and management of BV in newborn infants.

FIGURE 2 A colour chart to aid clinical recognition of BV. Any green-stained vomit is considered bilious and the infant should be assessed promptly. Yellow vomit is usually considered normal.
The incidence of malrotation was much lower in our study (0.06 per 1,000 births) compared to that quoted in the literature (0.17 per 1,000 births).1 In epidemiology, such statistics are usually calculated from whole populations from multiple centres, whereas our study was from a single centre, which could account for the lower incidence demonstrated here. While we have calculated the incidence of BV in a population of inborn infants, some infants may have been discharged from our hospital and presented directly to another hospital. A review of infants who did not undergo UGI imaging did not reveal any presenting to the local children’s hospital surgical service with a subsequent surgical diagnosis. However, our estimate of the incidence of BV and surgical diagnosis is approximate as other infants with BV may have presented to the local children’s hospital. The most significant predictor of surgical pathology in this cohort was abdominal distension, with 100% sensitivity. Similar findings have been reported in other studies.3,5 Four infants in this cohort were diagnosed with Hirschsprung’s disease, all presenting with abdominal distension and BV, typically after 48 hours. Although delayed passage of meconium on its own did not predict surgical pathology in our cohort, Hirschsprung’s disease is usually characterised by this in combination with abdominal distension.12 BV can also be a cardinal sign of Hirschsprung’s disease.12 Abdominal distension is a clear risk factor for surgical pathology and any infant presenting as such, with or without BV, should be investigated and referred to a surgical service promptly.
Our results suggest that the timing of presentation may be important. Our findings demonstrated a trend toward later presentation in infants who subsequently were diagnosed with a surgical pathology. A UK prospective audit of neonates with BV reported a median age of presentation of 26 hours.4 As these infants were referred to a surgical service, that study demonstrated a much higher incidence of surgical pathology. Although the audit did not specifically look at the age of presentation in those with surgical pathology versus those without, it suggests that surgical pathology may be more likely if presenting after 24 hours. Only two infants in our cohort were diagnosed with malrotation, both presenting after 24 hours, which is consistent with other reports in the literature.7
It may be that BV in the first 24 hours is more common than has been appreciated and, in the absence of abdominal distension or clinical signs of an unwell infant, is less likely to be due to a surgical cause. 55% of our cohort presented at 24 hours or less and only one infant had a surgical diagnosis. This infant presented with abdominal distension and was diagnosed with Hirschsprung’s disease. Previous studies suggest that the yield of abnormal UGI contrast studies and surgical pathology is greater after day 2 in infants referred with BV,7 consistent with these findings. An Australian study of infants referred to a surgical centre with BV reported a mean age of admission of three and a half days and a 26.6% incidence of surgical pathology.6 This, again, could indicate that babies with surgical pathology are more likely to present later. Regardless, although most infants with BV will not have a pathological cause identified,6 investigation to exclude an underlying surgical condition (particularly malrotation) is recommended. Even though some would not consider referral for a UGI contrast study after a single BV,14 our review identified that all infants underwent either an AXR, a UGI contrast study or both (FIGURE 1).
An AXR successfully identified all infants with a surgical pathology in our cohort, however they also all presented with abdominal distension. The specificity of an AXR was much higher in our study (98%) compared to that reported in a recent UK observational study of neonates <7 days old with BV transferred by a regional service (14%).5 However, this was attributed to variations in interpretation of the X-ray films, mostly by junior inexperienced medical staff rather than a specialist,5 whereas all AXR reports in our study were by radiologists. Specificity and sensitivity scores for identifying a surgical or time-critical diagnosis with UGI contrast studies have been reported at over 90%.3 The lower sensitivity score for a UGI contrast study in our investigation may be attributed to the much lower incidence of surgical pathology; also, four out of the six infants with a surgical diagnosis had Hirschsprung’s disease and a UGI contrast study does not typically diagnose this. The two infants with malrotation in our study were both diagnosed with a UGI contrast study.
Even though a normal AXR is common in infants with malrotation, it may be prudent to consider it in infants with BV as it will diagnose duodenal atresia by demonstrating the typical double-bubble appearance.1,15 These infants can present with BV plus or minus abdominal distension.1 However, unless there is a clear diagnosis on an AXR, all infants with BV should be considered for a UGI contrast study or appropriate discussion with a paediatric surgeon.
Ultrasound may be an alternative investigation for detecting malrotation.9-11 The presence of the ‘whirlpool sign’ along with inversion of the superior mesenteric artery and superior mesenteric vein on ultrasound, has accuracy up to 100% for diagnosis of malrotation.11 However, as with any radiological investigation, the availability of experienced sonographers to scan babies with a potential time-critical diagnosis remains a limitation of ultrasound.
92% of our cohort received antibiotics as part of their management, with 67% discontinuing after 48 hours. In the majority of cases, the only documented indication was BV. There is no clear evidence that BV alone is a feature of early onset neonatal sepsis, particularly in a ‘well’ infant.16 Unless there is a clear suspicion of sepsis, judicious use of intra-venous antibiotics should be employed, as evidence suggests that prolonged or unnecessary antibiotic exposure may increase the risk of obesity, atopy and morbidity associated with necrotising enterocolitis, bronchopulmonary dysplasia and death in preterm infants.17
If the clinician decides that antibiotics are necessary, it is important that blood cultures are drawn correctly as they have excellent sensitivity for detecting bacteraemia.17 However, antibiotics should be discontinued as soon as possible in infants with sterile samples and a low suspicion of sepsis to begin with. Consideration should be given to whether antibiotics are necessary in the first place in well term infants with BV where the only question is whether they have malrotation and where a UGI study is readily available.
Conclusions
What was already known on this topic:
- BV is a common presenting feature of intestinal malrotation.
- UGI contrast studies are the best available investigation for diagnosing malrotation.
- Timing of presentation of BV is not fully understood.
What this study adds:
- This study from a non-surgical NICU showed a low incidence of surgical pathology (3.9%) in term infants admitted with BV.
- The most significant risk factor for surgical pathology was abdominal distension.
- The timing of BV presentation may be important. More than 50% of babies with BV presented within the first 24 hours. There was a trend toward later presentation in those with pathology.
- AXRs demonstrate a high sensitivity and specificity for predicting surgical pathology.
- UGI contrast studies to exclude malrotation should be performed in any infant presenting with BV.
Author contributions, acknowledgement and ethics approval
DC worked as a neonatal fellow at RWH from August 2019 to August 2020. He collected/interpreted the data and wrote the manuscript. CK established the cohort of patients, advised and assisted with data interpretation and made edits to the manuscript.
The authors are grateful for the assistance of Dr Leah Hickey, Royal Children’s Hospital, Melbourne, in collecting data about outcomes of babies transferred for surgical review.
Ethics approval was granted by the ethics department at RWH.
Or read this article in our
Tablet/iPad edition
- Larger multicentre cohort studies may improve our understanding of the timing of BV and its link to surgical pathology.
- Improving access to upper gastrointestinal contrast studies may reduce the need for unnecessary transfers to surgical centres.
- Understanding risk factors may help in parental discussions while awaiting investigations.
Also published in Infant:
