

Neonatal intubation skills: results of a national trainee survey
Neonatal intubation is a vital procedure, however, there are fewer opportunities for paediatric trainees to become proficient in this skill. This survey provides information about trainees’ current experiences of educational training, exposure and skills with regards to achieving neonatal airway competence as well as providing suggestions to inform future training and workforce planning.
Katie EvansNeonatal GRID trainee
Ashford and St Peter's Hospital NHS Foundation Trust
katie.evans7@nhs.net
Kathryn Macallister
Neonatal GRID trainee
St Michael’s Hospital Bristol
Jennifer Waspe
Anaesthetic Trainee
Sheffield Teaching Hospitals NHS
Eleri Adams
BAPM President and Consultant Neonatologist,
Oxford University Hospitals NHS Foundation Trust
Cheryl Battersby
BAPM Data and Informatics Lead and Academic Neonatologist
Imperial College London
Background
Over the last few years, the number of neonatal intubations has fallen across the UK, predominantly due to a wide range of improvements in perinatal care,1 including the increased use of non-invasive ventilatory techniques. For current paediatric trainees this has significantly reduced opportunities to gain skill and confidence in neonatal intubation skills. In 2022 the Royal College of Paediatrics and Child Health (RCPCH) recognised the lack of opportunity to achieve competence in this skill and removed neonatal intubation from the level 1 curriculum. Additionally, the new Progress Plus Curriculum has reduced the total duration of training from eight years to seven years and removed the requirement for a neonatal placement at senior registrar level, which is likely to decrease trainee exposure to neonatal intubation further.
Within adult anaesthetics, where airway competencies are key skills, it is suggested that over 40 intubations are required to be deemed competent (a success rate of > 80% at the first attempt).2 There is no current evidence available suggesting the number of neonatal intubations required to reach such proficiency levels. One UK-based study across four tertiary neonatal units found that only 53% of all neonatal intubations were successful on the first attempt, across all levels of operator from junior to consultant.3 When looking specifically at paediatric trainees, first time intubation success rates ranged from 38% (specialty trainees year 1 to 3) to 54% (specialty trainees year 4 to 8) with significantly lower success rates in the delivery room setting when compared to the neonatal unit. In practice, however, when drawing parallels between anaesthetic training and paediatric training it is important to recognise that the number of times a skill is performed is not used as a marker of competence. Anaesthetic trainees complete a three-month period of daily supervised work with supported teaching and simulation to achieve basic airway competence, which is assessed regularly. Only on completion of this supervised training period are they deemed suitable to be placed on an on-call rota with responsibility for airway management out of hours.
There is understandably a lot of concern among paediatric trainees regarding the over-reliance on trainees for successful airway management, including intubation. Currently within the UK, many hospitals rely on trainees to provide on-site senior cover overnight, and outside of tertiary neonatal units it is common for consultants to cross-cover paediatrics and neonates, thus performing intubation very infrequently. Within the UK, it is common practice for the paediatric registrar to hold sole responsibility for neonatal airway emergencies out of hours, and even if their lack of skills and confidence were to be communicated with anaesthetic colleagues, it is unlikely that they themselves would feel confident enough with neonatal airway skills to support. A previous UK-based trainee survey from 2019 demonstrated that only 18% of trainees feel completely confident at neonatal intubation4 and anecdotally trainee forum communications suggest many felt quite distressed by the curriculum changes with their associated uncertainty of who is expected to perform this potentially life-saving procedure in the future.
Aims
This national survey aimed to update our knowledge regarding neonatal intubation exposure of paediatric trainees in 2022 in England in view of its removal from the level 1 RCPCH curriculum. It considered three main aspects:
- training in neonatal intubation
intubation experience
barriers to developing intubation skills.
The ultimate objective is that these results could be used to help inform education and training guidelines, alongside workforce planning for the future.
Methodology
A 20-question survey was conducted via an online platform with key stakeholders, including neonatal, paediatric and anaesthetic trainees contributing to question design to ensure representation. National dissemination took place in February 2022 via the British Association of Perinatal Medicine (BAPM), RCPCH trainee representatives and social media. Structured answers were invited in preselected domains for quantitative analysis and also in free text to allow analysis of important themes.
Results
Trainee demographics
There were 210 participants across the UK, with only 8.6% comprising those working within neonatal subspecialty training (GRID). From a seniority perspective, 28% were working at ST1-3 level, 31% ST4-5 level and 41% ST6-8 and their answers and confidence were considered separately throughout the analysis. However, we considered it important to recognise that seniority within the training programme would not necessarily correlate with neonatal experience so this was captured separately. Geographically there was good representation across the UK with trainees responding from within all regions.
Formal intubation training exposure
Of the trainees that responded to the survey, 1.4% reported never having received any neonatal intubation training to date. The most commonly reported training modality was the supervised intubation of a term infant, with 87% of trainees having received this. It was clearly demonstrated that the commonest training modalities were ‘shop-floor’ exposure with observation and supervised intubations on term and preterm babies. Notably, theoretical training was significantly less frequent, with only 31% of trainees reporting being trained on the medications used and only 50% having attended a lecture on neonatal intubations (FIGURE 1).
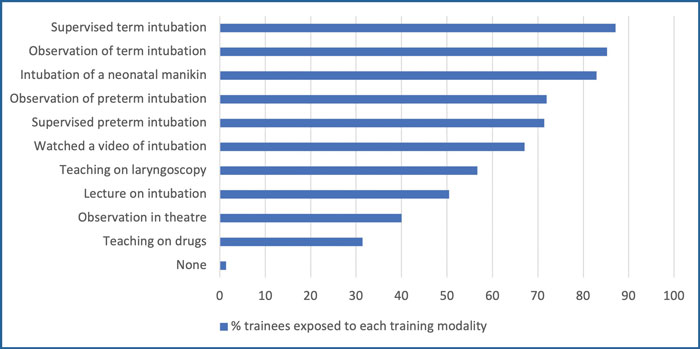
FIGURE 1 Exposure to formal training modalities in neonatal intubation.
Intubation experience
There is a wide range in number of supervised and unsupervised intubations (TABLE 1) and it is notable that only two-thirds of senior ST6-8 trainees have independently intubated more than 10 times. During ST1-3 training, the majority of trainees achieved between one and 10 supervised intubations, however even prior to the curriculum change, 14% of trainees progressed to registrar roles having never successfully intubated.
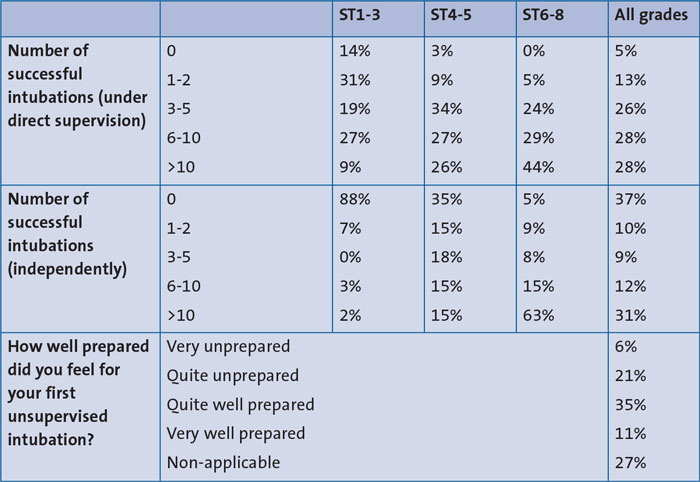
TABLE 1 Number of successful supervised and unsupervised neonatal intubations.
Trainee confidence in neonatal intubation
Confidence rates vary significantly among trainees, correlating most closely with the duration of time working within a neonatal setting, rather than the level of training.
27% of trainees surveyed did not feel adequately prepared prior to undertaking their first independent intubation with only 11% feeling very well prepared (TABLE 1). Of these trainees, most felt unprepared due to a lack of previous experience (32%), followed by patient instability (20%), an extremely premature infant (12%) or a previous negative experience (11%).
Trainees were asked to rate their confidence levels in the three key domains of equipment preparation, drug use and understanding of the procedure on a 10-point Likert scale from ‘not-confident’ to ‘extremely confident’. Trainees demonstrated the highest levels of confidence (10 on the Likert scale) regarding equipment preparation (46.2%) followed by the view on laryngoscopy (32.4%), the procedure (30.5%) and the lowest levels of confidence with the use of drugs (8.6%) (FIGURE 2).
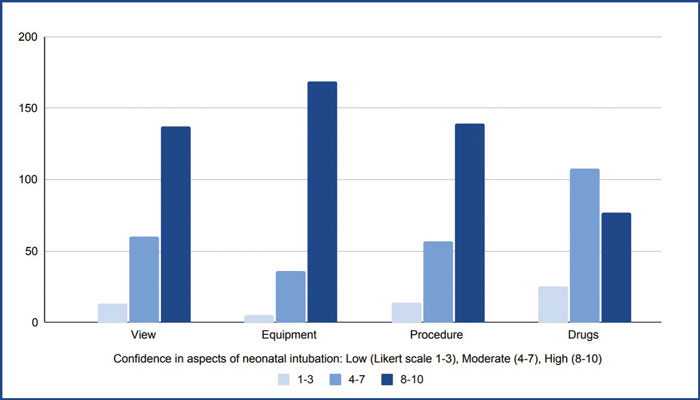
FIGURE 2Confidence in preparing equipment, use of drugs, view on laryngoscopy and the procedure of neonatal intubation.
Trainee opinions
When questioned on why neonatal intubations are difficult, trainees felt it was a combination of patient factors (prematurity, birth weight, anatomy), psychological factors (stress, pressure) and experiential factors (limited experience). Most respondents (74.8%) did not feel that environmental factors such as access to the correct equipment contributed to difficulties in neonatal intubation (FIGURE 3).
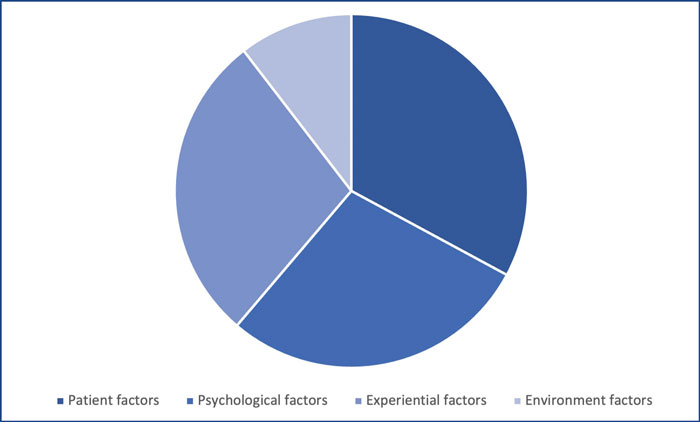
FIGURE 3Trainee opinions on why neonatal intubations are difficult.
Discussion
This survey has updated our existing knowledge regarding the difficulties faced by current trainees in achieving neonatal airway competencies. It is clear that trainees are exposed to very few intubation attempts at junior levels of training and therefore are extremely unlikely to achieve a ‘competent’ standard of practice as defined in adult anaesthetic literature. With laryngeal mask insertion now a key component of Newborn Life Support,5 this may further mitigate the need for intubation skills, however in smaller babies and those requiring a secure airway there is a concern that the next generation of doctors will not be proficient at intubation.
Trainees were asked to describe what factors contributed to feeling unprepared for performing neonatal intubation and there were a number of common themes. Multiple trainees mentioned a lack of support, particularly when working outside of a tertiary neonatal setting with comments such as:
- “Consultant refused to attend”
“Sent to a district general to be by myself on nights with 24 and 25 weekers delivering”
“No backup on site”
“Consultant more than one hour away.”
The reduced exposure to intubation has resulted in many registrars not feeling confident and wanting practice, hence even less opportunities for junior trainees. This competition for the few procedures exten-ded to other members of the multidisciplinary team with many trainees feeling that permanent staff were prioritised:
- “Most of the time the ANNPs get to do it as they’re quicker and can do it unsupervised”
“Procedures were given preferentially to the ANNP.”
The general structure of training was also regularly mentioned as an issue, with neonatal rotations often spaced years apart, further compounded for those trainees who take time out of training or work less than full time.
There were lots of constructive suggestions from trainees who participated in the survey for ways to improve neonatal intubations. The commonest theme was simply increasing exposure and practice; however, it was acknowledged that as intubation becomes less frequent this is a real challenge. Some potential solutions posed included exposure to paediatric intubation on routine anaesthetic lists. Several participants mentioned a desire for better theoretical training – specifically didactic teaching on drugs, views and equipment. Simulation was also mentioned frequently as a potential solution – especially using term and preterm or high-fidelity manikins, however the effect of simulation training on neonatal intubation success is still unclear.6 Training on various equipment was also suggested, such as direct laryngoscopy, video-laryngoscopy and the use of airway adjuncts such as iGels. It was mentioned that although many units may feel that they offer this teaching as part of their regular teaching programmes or simulation sessions, the shift-based rota systems mean that unless it is scheduled for multiple times over the same rotation, many trainees will not be given the opportunity to attend. One trainee suggested that perhaps there should be a standardised course that all trainees are given study leave to attend at some point during their training to achieve consistency.
The service provision role of junior trainees, who often spend a large proportion of their neonatal training on the postnatal wards undertaking care such as newborn baby checks, despite these not being advocated as routine training,7 was also cited as a barrier to achieving intubation competencies. Practically within a standard six-month tertiary neonatal rota, many trainees may only have around 14 shifts timetabled in neonatal intensive care where the best training opportunities are. There was also some discussion of future workforce planning with trainees suggesting that in the future it may be necessary to share responsibility with anaesthetists in district general hospitals.
Most paediatric trainees do not feel confident in neonatal intubation and would welcome more structured training on airway management. Our findings from this group of key stakeholders should be useful to inform future work to improve training and workforce planning surrounding the provision of neonatal intubation. Currently, BAPM is developing a new framework for practice on airway standards for UK neonatal services, which will aim to address the standards expected for managing the neonatal airway in neonatal units. The framework will be accompanied by development of resources to improve training and education for all staff types, including an e-learning package for drugs used for intubation.
Or read this article in our
Tablet/iPad edition
- Opportunities to develop neonatal intubation skills are falling for UK-based trainees.
- Training and experience with neonatal intubation is variable and it is important to quantify this to identify areas for improvement.
- The recent removal of neonatal intubation as a core competency for level 1 trainees should act as a prompt for the neonatal community to consider how to train and workforce plan to safeguard future infants.
Also published in Infant:
