

Exploring the landscape of the ANNP workforce: results of a UK-wide survey
This article discusses a UK-wide survey to gather information related to the advanced neonatal nurse practitioner (ANNP) workforce. The cohort of ANNPs that responded to the questionnaire provided detailed information on various aspects of their role and a positive response to the proposal for a career framework. The data gathered will be used to influence the design and production of a career development framework for ANNPs.
Kirstin WebsterANNP
Jane Couper
ANNP
Joanne Hodson
Nurse Consultant
Melanie Carpenter
ANNP
Tracey Jones
Senior Lecturer in Neonatal Nursing
tracey.m.jones@manchester.ac.uk
In collaboration with the BAPM Working Group to develop an ANNP career framework (TABLE 1)
Background
The impact of workforce shortages upon service delivery of neonatal care across the UK has been thrown into sharp focus,1,2 with considerations of workforce and service delivery models under increasing scrutiny. Strategic recommendations, aimed at supporting service delivery and the ANNP workforce, have included reviewing the role of ANNPs to ensure maximisation of skill-sets and clear training and development to support mechanisms to help retain and develop staff, producing a more stable mixed workforce.3,4
In early 2019 a survey that was endorsed by the British Association of Perinatal Medicine (BAPM) was designed and distributed as an information gathering exercise to provide data on the current ANNP workforce. ANNPs were invited to take part via the BAPM website, Twitter and Facebook groups and via the professional social media sites of both the Neonatal Nurses Association and the Scottish Neonatal Nurses Group. UK-wide neonatal units were also contacted via operational delivery neonatal networks in England, Wales and Northern Ireland and neonatal managed clinical networks in Scotland.
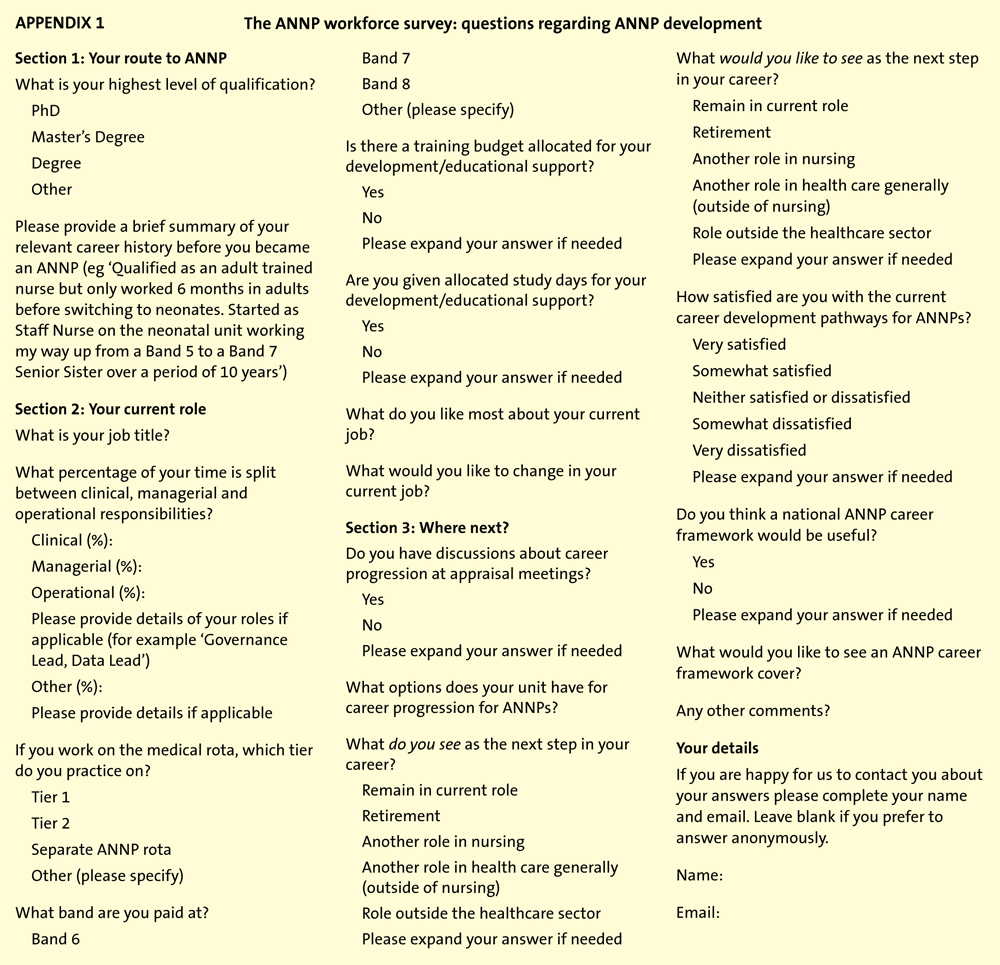
The survey was designed by BAPM Nurse Representative Joanne Hodson and BAPM Chief Executive Kate Dinwiddy who hypothesised disparity between NHS trusts and health boards regarding ANNP activities, pay band, rota and level of education. It comprised a self-completion questionnaire with facility for additional narrative and optional anonymity (APPENDIX 1).
Further information was sought alongside the questionnaire regarding the number of ANNPs working in individual NHS trusts and health boards by directly contacting neonatal units to request information on the number of ANNPs in their team. This number is yet to be finalised as not all units have responded to the inquiry. However, it is known that there are 78 whole time equivalent ANNPs working in Scotland with a further 10 in training. There are 22 in Wales with six trainees. In England the estimate is 347 including those in training. The numbers in Northern Ireland remain unknown. Although these figures were correct at the time of collection they may now differ due to the ever-changing ANNP workforce profile.
Since the survey was distributed BAPM has endorsed the establishment of a working group to assist development of an ANNP career development framework (TABLE 1).5 Data analysis from this survey will add contextual evidence to support the production of the BAPM ANNP career framework and will add to the body of evidence regarding the working landscape of ANNPs in the UK.
TABLE 1 Members of the BAPM Working Group to develop an ANNP career framework.
Responses to the questionnaire
There were a total of 126 responses to the questionnaire; there was one dataset missing and one duplicate entry, leaving 124 remaining for inclusion. Respondents were allowed to continue through the questionnaire without answering all of the questions.
Level of education
Of those who answered:
- 19.4% (24/124) have studied to degree level
- 5.6% (7/124) have completed post-graduate education (PG Certificate or PG Diploma)
- 70.2% (87/124) are educated to Master’s level
- 1.6% (2/124) have completed PhD studies (FIGURE 1)
- four gave incomplete or unclear answers.
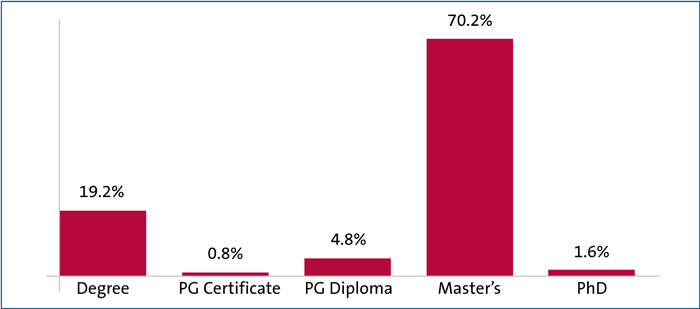
FIGURE 1 Highest level of qualification.
Background
ANNPs have entered the field of neonates from a variety of backgrounds:
- 31.1% (38/124) from a paediatric nursing background
- 16.4% (20/124) qualified as adult nurses
- 2.5% (3/124) are direct entry midwives
- 40.3% (50/124) have completed dual or triple training in combinations including adult nursing, paediatrics, midwifery and health visitor training
- 13 gave no information in response to this question.
A further breakdown of background by specialty can be found in FIGURE 2.
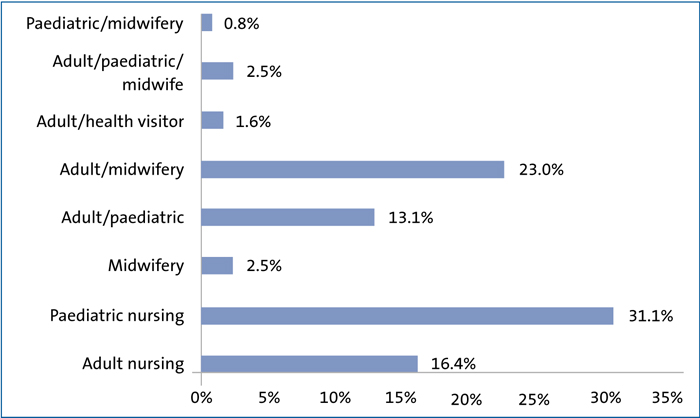
FIGURE 2 Background by specialty.
Job title, banding and rota
122 responded with their job titles:
- 88.5% (108/122) of these are a variation on ANNP (ie ANNP, Senior ANNP, Lead ANNP, Transport ANNP, Senior Nurse/ANNP, Senior ANNP and Joint Clinical Lead, ANP, Advanced Clinical Practitioner - Neonates)
- 7.4% (9/122) described their job title as Trainee ANNP.
The remaining job titles for respondents who have trained and are currently working as or have worked at some time as an ANNP are:
- Clinical Lead Nurse for Neonatal Surgery
- Lead Nurse for Neonatal Transport Service
- Lecturer/Researcher in Women and Child Health
- Clinical Director Neonatal Services and Neonatal Nurse Consultant
- Lead Midwife Practice Development and Education.
This displays some of the potential clinical roles beyond ANNP.
Of the 108 respondents with the job title ANNP (or variation thereof):
- 85.2% are band 8 (inclusive of those who answered band 8, band 8A or band 8B)
- 9.3% are paid at band 7
- 3.7% of trained ANNPs are paid at band 6
- 1.9% answered ‘other’.
Of the nine Trainee ANNPs:
- 55.6% are paid at band 7
- 44.4% are paid at band 6
- 44.4% are on a supernumerary rota
- 33.3% are on a separate ANNP rota
- 22.2% are working on the tier 1 rota.
Of the 113 qualified ANNPs that responded:
- 42.5% are working on the tier 1 rota
- 23.9% are working at tier 2
- 23% have a separate ANNP rota
- one respondent is working on a consultant level rota and one on a nursing rota
- 3.5% are incorporated on a transport rota
- of the 4/113 who responded ‘other’, two work on both the tier 1 and tier 2 rota.
FIGURE 3 illustrates the rota distribution.
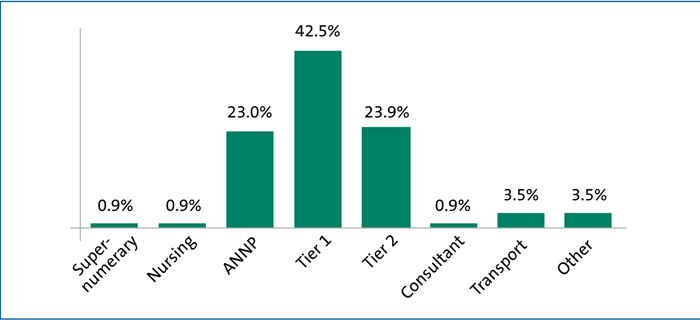
FIGURE 3 Rota distribution.
Study leave
Half of the respondents that replied to this question said a study leave budget is available (61/122); 44.3% (54/122) answered that no budget is available. The remainder gave unclear answers or didn’t know. Time allocated for study leave is available for 73.0% (89/122); 23.8% (29/122) have no allocated study leave.
Time split
Respondents were questioned on how they split their time between clinical, mana-gerial, operational or other activities. They were not asked if they had a formal job plan in place and no one responded with this information voluntarily.
Of 124 respondents, 21.8% (27/124) of the total times did not add up to 100%; time allocations given ranged from 66% to 150%. Analysis of the remaining 97 respondents revealed 24.7% (24/97) listed 100% clinical time. The range of clinical time was between 20% and 100% (median 85%). Managerial time ranged from 0-60% (median 5%) time and ‘other’ ranged from 0-70% (median 10%).
Additional activities on top of clinical work include audit, governance, teaching, quality improvement, guidelines, mentorship, simulation, Newborn Life Support faculty, perinatal mortality review tool and research.
Likes/dislikes of the role
The main enjoyable aspects of the role include:
- autonomy
- working with families and babies
- clinical skills, clinical decision-making, multidisciplinary team (MDT) working
- the challenge and variety of the role
- the ability to remain in a patient focused clinical role while advancing their practice (FIGURE 4).
FIGURE 4 Reports from individuals about aspects of their role that they like.
Elements of the role that respondents would like to change:
- more time to incorporate education and formal training
- expansion of the role into clinics and extending clinical skills/procedures
- more allocated time for non-clinical work
- improved recognition of the role (some think of this role as ‘playing at being a doctor’).
Many felt undervalued in comparison to the medical trainees, citing that they feel used ‘to plug medical rota gaps’. Disparity between pay bands across the UK was mentioned, ranging from band 6 to 8b for the same role. Some respondents alluded to their advancing age and the impact of working night shifts. There were comments that suggested that younger medical trainees would be better placed to cover night shifts.
Career progression
77.0% (94/122) discussed career progression at their appraisal and when asked what career progression is available to them, 50.8% responded to say ‘none’, ‘not sure’ or ‘don’t know’.
Framework
When asked if a career framework would be useful, 91.1% (113/124) replied yes. Of these, 70.8% (80/113) gave a narrative response outlining what they would like to see included in a framework. There was overwhelming reference to a standardisation of the ANNP role with clear progression throughout the UK. Education aligned with the medical trainees and recognition of advanced practice on the Nursing and Midwifery Council (NMC) register was also stated, in addition to competencies and access to an e-portfolio based on the four pillars of advanced practice (FIGURE 5).
FIGURE 5 Suggestions for the ANNP career framework.
Discussion
The results of the survey display a hetero-genous group with a disparity between pay bands, job title and background. The survey demonstrates that more than half of those who responded do not foresee any career progression available to them.
The participants who responded are highly qualified and vary greatly in the activities they perform over and above the clinical aspect of the role. More than 90% stated that a career framework would be useful, with many giving suggestions of elements for inclusion.
It was recognised during the first meeting of the BAPM Working Group to develop an ANNP career framework that crucial information was missing from the data received via the questionnaire. A lack of demographic information including respondent age, years to retirement and amount of their personal time spent on work-related activities was not included in the questionnaire. Additional information that would have been useful to obtain would have related to personal funds used for training and conference attendance. Contracted hours and shift pattern, for example 12.5-hour shifts or 7.5-hour shifts and time spent on extra activities in hours as percentages have proven to be inaccurate.
Limitations of this questionnaire lie in the wording and design of the questions. Too many open questions allowing for free text alongside closed questions can lead to difficulty in quantifying data. Assigning identifiers to respondents (eg NMC PIN number) may discourage some people from responding for fear of identification but otherwise leaves open the potential for duplication of respondents.
There may be disparity between NHS trusts and health boards as to who is incorporated in the tier 1 rota, for some this may include foundation doctors (FY2), GP specialty trainees and paediatric specialty trainees of levels 1-3. Some units that are able to support neonatal grid trainees may differ in the grade of medical staff incorporated on their tier 2 rota.
Conclusion
A positive response to the creation and implementation of an ANNP career framework has been received. The cohort of ANNPs who responded to the questionnaire provided detailed information on various aspects of their role and this will inform the writing of the framework.
Or read this article in our
Tablet/iPad edition
- A questionnaire was designed and distributed to gather data on the current ANNP workforce.
- There were 126 responses to the questionnaire.
- The survey offers a snapshot of quantitative and qualitative responses and demonstrates that an ANNP career development framework would be well received.
Also published in Infant:
