

Bovine-based breast milk fortifier and neonatal outcomes in premature infants of <32 weeks gestational age
Breast milk (maternal or donor) is the gold standard nutrition for preterm infants. Breast milk fortifier (BMF) provides supplementary nutrition to avoid the high growth failure rates in preterm infants. Conflicting reports have implicated BMF, especially bovine-based products, in the development of necrotising enterocolitis (NEC) and persistent safety concerns regarding BMF have led to variability in use across the UK and internationally. This study examines whether the use of bovine-based BMF in preterm infants plays a role in the development of NEC, or an increase in all-cause mortality.
Kate W. Jordan
Clinical Fellow
Laura De Rooy
Consultant Neonatologist
Justin Richards
Consultant Neonatologist
Anay Kulkarni
Consultant Neonatologist
anay.kulkarni@stgeorges.nhs.uk
Neonatal Intensive Care Unit, St George’s University Hospital, London
Adequate nutrition and growth in hospitalised preterm infants are fundamental to their long-term physical and neurodevelopmental outcomes.1 Breast milk is the gold standard nutrition for preterm infants due to its multiplicative protective features, including a reduced risk of developing NEC.2,3 However, preterm infants receiving breast milk have high postnatal growth failure rates4 and supplementation with BMF has been shown to support growth and development in preterm and very low birthweight infants.5
In practice, BMF use is variable due to persistent safety concerns and conflicting reports implicating bovine-based BMF with the development of NEC.6-8
Within our tertiary surgical neonatal intensive care unit (NICU), bovine BMF (Cow & Gate Nutriprem Human Milk Fortifier) is routinely used as a supplement to human breast milk (maternal or donor). We undertook a 10-year retrospective audit of premature infants of <32 weeks gestational age (GA) to explore the possible relationship between BMF use and neonatal outcomes.
Materials and methods
This study was a retrospective single-centre audit of 952 preterm infants, born at <32 weeks GA at the tertiary surgical level 3 NICU of St George’s Hospital (SGH), London.
Subjects: Preterm infants, <32 weeks GA, born at SGH between January 2010 and September 2020, whose treatment was complete when data collection and analysis were performed. The total cohort comprised 952 infants. Analyses included the total cohort and subgroups by GA:
- GA 23+0 to 25+6 (n=221)
- GA 26+0 to 28+6 (n=325)
- GA 29+0 to 31+6 (n=406).
Data collection: Demographic and clinical variables were obtained from the patients’ notes on BadgerNet, UK, the national electronic neonatal database containing all clinical notes.
NEC: Bell stage II NEC diagnosis was confirmed from the clinical notes and defined as any infant who had clinical features consistent with NEC (abdominal distension, abdominal pain, bloody stools, radiographic evidence consistent with NEC) and received either medical treatment for ≥5 days or had surgical treatment or surgical review confirming NEC. Infants who received medical treatment for <5 days or had surgery for spontaneous intestinal rupture not associated with NEC, were excluded.
NEC cases were further sub-grouped as having surgical/severe NEC if they met the criteria for Bell stage IIIB NEC (requiring surgery) or died with a cause of death directly due to/contributed to by NEC.
Mortality data: All-cause mortality was defined as neonatal death during any episode onsite at the NICU. NEC causing or contributing to death was defined as infants who had NEC listed on their death certificate and/or those who died during treatment for NEC.
Analysis: Association between BMF use and the outcomes of interest was examined by calculating odds ratios (OR), risk ratios (RR), and number needed to treat (NNT). Significance was defined by p values and corresponding confidence intervals. Only NEC cases that developed after the introduction of BMF were included in relationship analyses.
Results
- Use of BMF increased significantly across the 10-year study timeframe. Conversely, NEC rates were stable across this timeframe
- BMF was not associated with an increased risk of developing NEC in preterm infants, including within subgroup analyses
- BMF was not associated with an increased risk of all-cause mortality
- In the most clinically vulnerable subgroup (<26 weeks GA), BMF use was associated with a decreased risk of developing NEC and decreased all-cause mortality.
BMF use over time
Use of BMF increased in our NICU from 2010 to 2020 in all subgroups analysed (FIGURE 1A, 1B). In 2010, 10.5% of the cohort received BMF, compared to 45.8% of the 2020 cohort.
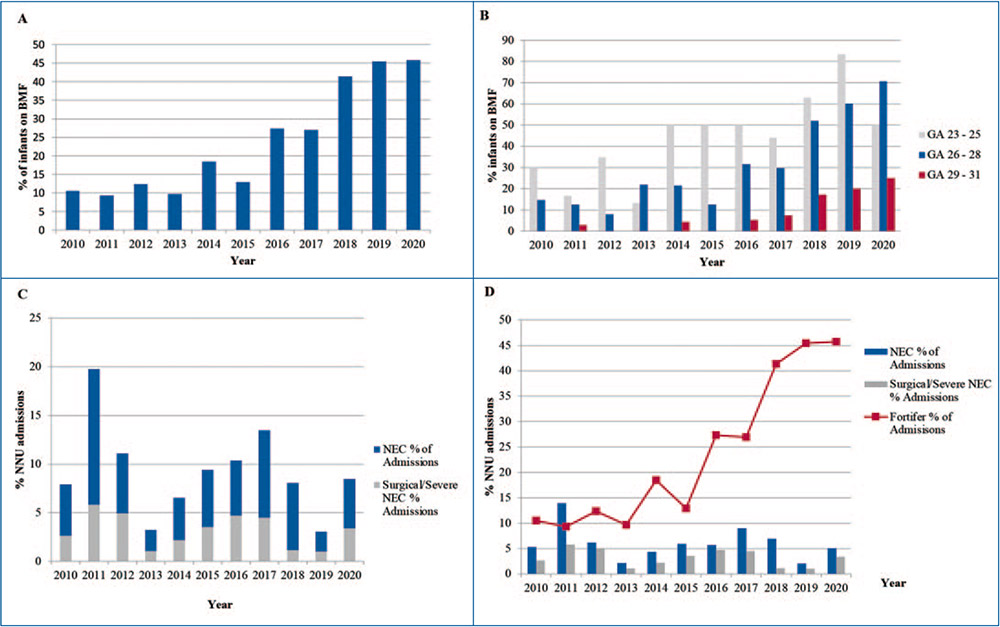
FIGURE 1 Bovine-based BMF use and the development of NEC in infants <32 weeks GA on the NICU of SGH from 2010-2020. (A) BMF use in full cohort. (B) Subgroup analysis of BMF use by GA. (C) NEC rates, Bell stage II and surgical/severe NEC. (D) BMF use overlayed with rates of Bell stage II NEC and surgical/severe NEC.
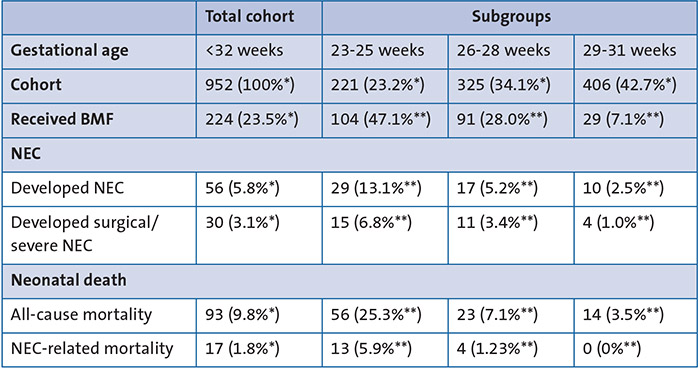
TABLE 1 Characteristics of the study cohort. The total cohort comprised preterm infants born at SGH at <32 weeks GA from Jan 2010 to September 2020, whose treatment was complete at the time of analysis (n=952). All statistical analyses were run for the total cohort and subgroups by GA. * % of total cohort of 952 infants across entire audit time frame. ** % of gestational age subgroup across entire audit time frame.
NEC rates over time
During the audit timeframe, 5.9% of the total cohort developed NEC (n=56 infants, TABLE 1). Among NEC cases, 53.6% (n=30) developed surgical/severe NEC (3.2% of the total cohort).
The majority of the infants that developed NEC (51.8%) were <26 weeks GA (n=29, 13.1% of admissions in that subgroup); 30.4% were 26-28 weeks GA (5.2% of admissions within that subgroup); and 17.9% were 29-31 weeks GA (2.5% of admissions within that subgroup) (FIGURE 1C and TABLE 1).
Rates of developing NEC did not change significantly over time:
- from 2010 to 2014, 6.3% of the cohort developed NEC
- from 2015 onwards, 5.8% of the cohort developed NEC (FIGURE 1C).
BMF use and the development of NEC
BMF use did not increase the odds or risk of developing NEC within the total cohort (OR=0.62, CI=0.30-1.29, p=0.20; RR=0.64, CI=0.32-1.28, p=0.21), nor within any subgroups analysed by GA (TABLE 2). Extremely premature infants of <26 weeks GA, were at less risk of developing NEC if they received BMF (OR=0.31, CI=0.12-0.76, p=0.01; RR=0.36, CI=0.16-0.90, p=0.01; NNT for benefit=4.80-30.32).
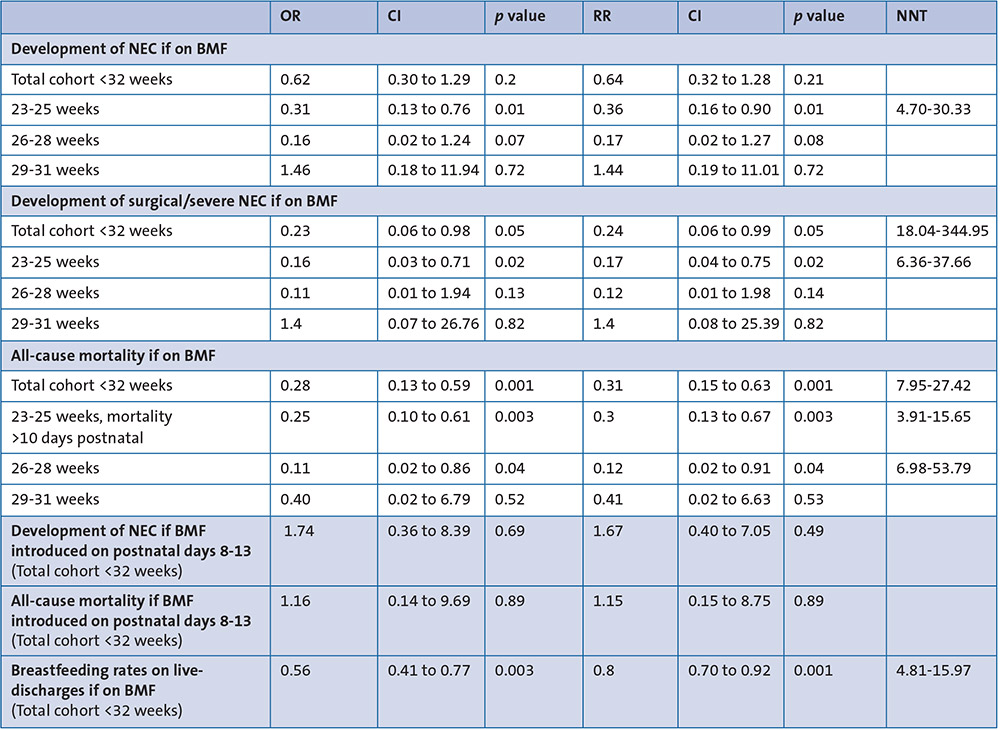
TABLE 2 Association of BMF with the development of negative outcomes, including subgroup analyses. BMF use did not increase the odds or risk of developing the negative outcomes (NEC, surgical/severe NEC, or all-cause mortality). Neither the risk of developing NEC nor all-cause mortality were increased if bovine-based BMF was introduced on postnatal days 8-13. Breastfeeding rates on live discharges were not statistically reduced if on BMF. Key: OR=odds ratio; CI=confidence interval; RR=risk ratio; NNT=number needed to treat.
BMF use was associated with a decreased risk of developing surgical/severe NEC in our total cohort (OR=0.23, CI=0.06-0.98, p=0.05; RR=0.24, CI=0.06-0.99, p=0.05; NNT=18.04-344.95), and for infants in the <26 weeks GA subgroup (OR=0.16, CI=0.03-0.71, p=0.02; RR=0.17, CI=0.04-0.75, p=0.02; NNT=6.36-37.66) (TABLE 2).
BMF can be introduced at any postnatal age and introducing BMF early in postnatal development (between days 8 and 13) was not associated with an increase in developing NEC (OR=1.74, CI=0.36-8.39, p=0.69; RR=1.67, CI=0.40-7.05, p=0.49) (TABLE 2).
Of the 56 babies who developed NEC during the study period, nine were exposed to BMF prior to developing NEC (16.1%). Across the audit, 215 babies were exposed to BMF for at least one day and did not subsequently develop NEC (95.9% of babies initiated on BMF did not develop NEC). Four babies developed NEC prior to BMF being initiated and, following recovery from NEC, were subsequently intro-duced to BMF without recurrence of NEC.
Among the infants who developed NEC following exposure to BMF (n=9), the time from BMF exposure to the onset of NEC ranged from 1 day to >2 months. Three babies developed NEC within three days of exposure to BMF (33.3%); three babies developed NEC after 4-7 days of BMF (33.3%); two babies developed NEC after 8-14 days of BMF (22.2%). One baby developed NEC after >14 days of BMF supplementation (11.1%).
Probiotics were not routinely used on the neonatal unit during the study period.
Mortality
NEC was a cause of death for 17 infants across the study timeframe, representing 56.7% of the infants who developed surgical/severe NEC (FIGURE 2).
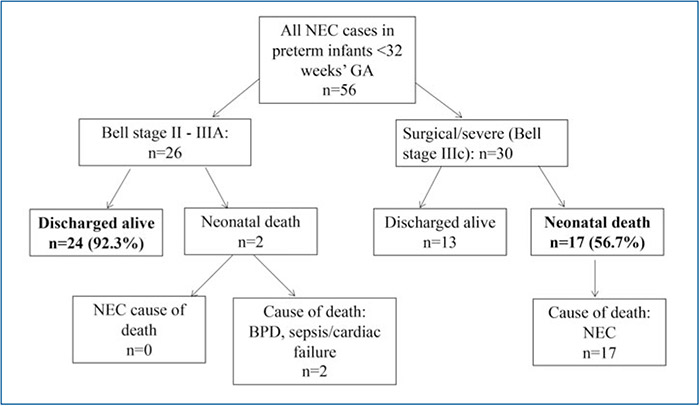
FIGURE 2 NEC rates and mortality rates of infants who developed NEC. Developing surgical/severe NEC had a mortality rate of 56.7%.
BMF use was associated with a decreased risk of all-cause mortality in preterm infants of <32 weeks GA (OR=0.28, CI=0.13-0.59, p=0.001; RR=0.31, CI=0.15-0.63, p=0.001; NNT for benefit=7.95-27.42) (TABLE 2). Within the subgroup analysis, there was no increased risk of all-cause mortality associated with BMF use. Extremely premature infants of <26 weeks GA were at less risk of all-cause mortality if on BMF; this was true for all infants in this subgroup, and those who survived >10 days postnatally (OR=0.25, CI=0.10-0.61, p=0.003; RR=0.30, CI=0.13-0.67, p=0.003; NNT=3.91-15.65).
Discussion
Rates of BMF use increased over time, while NEC rates remained stable
BMF use increased significantly over time on our NICU (FIGURE 1A, 1D), consistent with results of a recent UK-wide survey of neonatal dietitians reporting BMF use in all responding units.9
Notably, increase in BMF use on our unit corresponds to the implementation of a standardised local protocol for introducing BMF in 2016, rather than an increase in overall use of breast milk in the NICU (as demonstrated by a stable rate of breastfeeding on discharge across the audit timeframe (FIGURE 3). Nationally, 77% of UK neonatal units employ standardised BMF guidelines, with variation between them in criteria for starting BMF.9
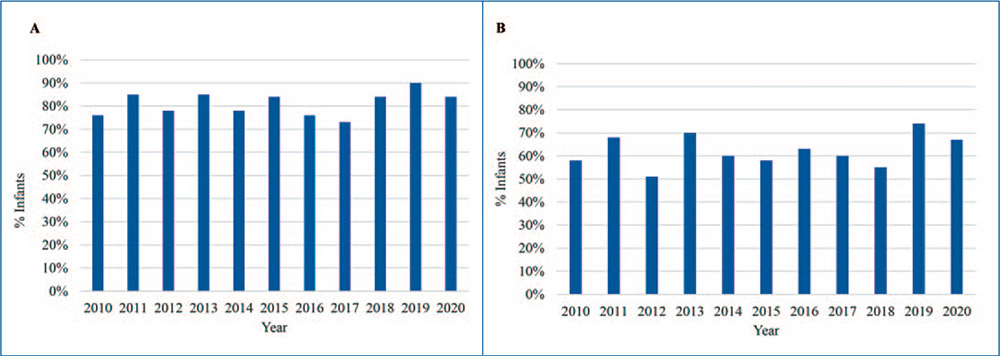
FIGURE 3 Breastfeeding rates of infants <32 weeks GA at birth on discharge across the audit timeframe. (A) Infants (% admissions) who received any breast milk on discharge across the 10-year audit timeframe. (B) Infants (% admissions) who were exclusively breastfed on discharge. Contrasting with the significant use of BMF over the audit timeframe, the rates of breastfeeding on discharge remained stable.
Contrasting with increasing BMF use, incidence of NEC on our NICU did not increase over time (FIGURE 1D). In our cohort there was a 3.2% rate for severe NEC, which corresponds with a whole population surveillance study carried out in England between 2012 and 201310 showing a national rate of severe NEC of 3.15%. For the current study, the criteria for defining NEC were intentionally broad, so as not to underestimate NEC incidence.
Use of BMF did not increase risk of negative outcomes
Reassuringly, the use of BMF was not associated with either an increased risk of NEC or all-cause mortality.
Internationally, variability in BMF use is unsurprising given the persistent belief that an exclusively human milk derived diet is best for NEC prevention. However, a Cochrane review found insufficient evidence to support this conclusion: there was low certainty evidence from one study, which showed no change in risk of NEC between infants given human milk-derived versus bovine-derived fortifier.11 A recent meta-analysis suggesting NEC rates were increased with bovine vs human BMF had only weak quality evidence and included significantly fewer infants than our study.8 Our work, which is a large single study analysis over a long time period, provides reassurance as to the safety of bovine-derived fortifier for preterm infants. This is especially important considering the great cost burden of providing human milk fortifier, and the remaining ethical contro-versies in the processes required to produce human milk fortifier.
As our unit’s BMF protocol has no minimum postnatal age, we were reassured by results that early BMF introduction (postnatal days 8-13) was not associated with an increased risk of NEC or all-cause mortality.
Protective role of BMF
BMF use was associated with a decreased risk of developing NEC, surgical/severe NEC, and all-cause mortality in extremely clinically vulnerable infants of <26 weeks GA. A Cochrane review of trials of multi-nutrient fortification found a slightly improved in-hospital rate of growth associated with BMF use.7 Our work may suggest that extremely clinically vulnerable infants are those in whom adequate nutrition, as provided by BMF, has the strongest protective benefit. Further investigation is needed to corroborate this finding.
Use of BMF and its effect on breast milk feeding/breastfeeding
In a study by Ericson et al,12 BMF use in premature babies was felt to be potentially associated with lower rates of breast-feeding. Breastfeeding rates of preterm infants of <32 weeks GA on discharge across the audit timeframe are shown in FIGURE 3. The use of BMF in our audit from 2010-2020, showed that rates of breastfeeding on discharge remained stable. This observation was in line with findings of a UK-wide audit published in 2017.13
Limitations
One of the limitations of the study is its retrospective design. The data are over a 10-year period and multiple factors including improved perinatal care and change in feeding protocols during that period can affect the outcomes. However, we demonstrate that NEC rates, including rates of severe/surgical NEC for inborn babies in our unit, remained grossly unchanged while our fortifier use increased almost four-fold.
Conclusion
The use of bovine BMF was not associated with adverse outcomes in this study. BMF use was associated with a decreased rate of adverse outcomes in the most clinically vulnerable infants. This study demon-strates that breast milk fortification with bovine-based products was not linked to an increase risk of developing NEC in preterm neonates of <32 weeks GA across our 10-year study. Preterm infants on bovine-based breast milk fortification did not have an increased risk of all-cause mortality.
Statements and declarations
Competing interests: The authors have no competing interests to disclose.
Contributions:AK and LDR conceived the study and developed the methodology. KJ performed data collection, analysis and prepared the first draft of the study manuscript. All authors developed the final manuscript.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Ethics: This study was conducted as a registered audit. Data collection was authorised as part of a registered audit.
Or read this article in our
Tablet/iPad edition
- The use of bovine BMF was not associated with adverse outcomes in this study.
- BMF use was associated with a decreased rate of adverse outcomes in the most clinically vulnerable infants.
- The results from this study encourage the use of BMF in preterm infants in neonatal intensive care settings.
Also published in Infant:
