

Using social media to improve the communication bottleneck in learning from risk incidents
The intensive care environment is prone to risk incidents. Bradford Neonatology introduced a multi-platform approach including social media to provide improved awareness and timely dissemination of learning from risk incidents. A qualitative survey a year after introduction showed that staff felt this to be a useful learning tool that had led to a perceived change in their practice
Caroline Fraser
MBChB, BSc, MRCPCH, DTM&H
Paediatric ST5 Registrar
carolineafraser@gmail.com
Charlotte Ashton
MBBS, BSc Hons, MRCPCH
ST6 Neonatal Grid Trainee
Carol Hudson
RGN
Advanced Neonatal Nurse Practitioner
Sunita Seal
MBBS, DCH, MRCPCH
Consultant Neonatologist
Neonatal Unit, Bradford Royal Infirmary
A risk incident is defined as any unintended or unexpected incident that could have or did lead to harm.1 Intensive care environments are well known for being prone to both risk incidents and ones with significant consequences. Reporting these incidents has become an integral part of improving patient safety within the UK. Part of this process involves effective communication with the team about learning outcomes (FIGURE 1).

FIGURE 1 The four main stages involved in learning from risk incidents (adapted from Drupsteen et al 20132).
Providing feedback to the team from incidents is important to demonstrate that incidents have been acknowledged, acted upon, and that lessons have been learnt.3 Lack of feedback from incident reporting has been shown to contribute to a lack of incident reporting from staff, whereas at least monthly feedback has shown an increase in the number of incidents filed.4
Common methods for delivering the feedback of learning outcomes to frontline staff include monthly e-newsletters and placing posters around departments.4 It is important that the information being delivered is done in such a way that it reaches each team member. This needs to take into account that the majority of clinical staff are busy shift workers.
One way to increase the coverage and penetration of these messages is through using effective channels, sending brief, clear and comprehensive messages in a way that is accessible to all staff.
Aims
The aims of the study were to:
- increase the frequency of feedback to the neonatal team from reported risk
incidents
- develop the use of multiple channels (especially social media) for rapid and timely dissemination of learning
- directly involve the multidisciplinary team (MDT) in the management of risk incidents
- encourage learning from risk incidents and identification of areas for improvement.
Methods
Bradford Neonatology is a neonatal intensive care unit (NICU) with 31 cots. There is a pro-active attitude to filing incident reports among the MDT, with the aim of learning and implementing changes to prevent future incidents. The reporting system has been highlighted as a particular strength in the General Medical Council trainee feedback (top quartile in the country).
The previous practice for communicating risk incident learning to the team was via monthly newsletters by the neonatal consultant and advanced neonatal nurse practitioner (ANNP) in charge of risk management. These involved ‘risk themes’ and were usually two or three A4 pages in length. The themes often incorporated multiple similar risk incidents into one theme, eg a reminder about breast milk practice based on multiple incidents with breast milk errors. Therefore, more than one incident was often reflected in a theme. The reports were emailed to staff members and a few copies put up in the department. These were time consuming to create and as a result were not always monthly. They were also time consuming for staff members to read and it was recognised that many staff did not even open the emails with the attached newsletters.
The risk team decided to introduce an innovative approach to ensure rapid and timely dissemination of learning from risk incidents. The initial project team included the neonatal consultant and ANNP in charge of risk management, and one junior doctor. Incidents reported via the online Datix system were reviewed on a weekly basis and action/learning points agreed.
An aesthetic A4 sized poster was created with no more than six learning points (FIGURE 2).
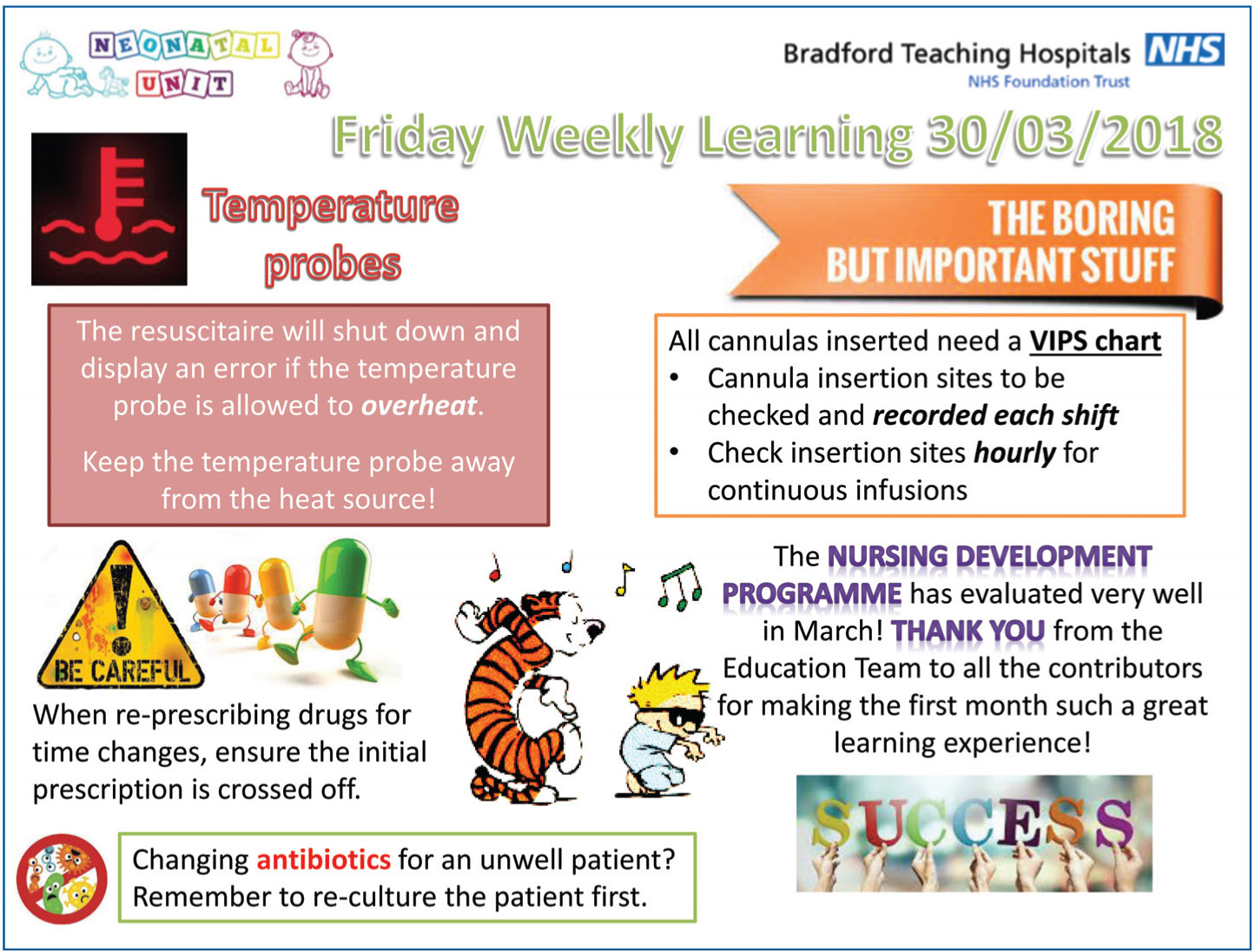
FIGURE 2 Example of a poster with learning points.
The poster was presented at the weekly multidisciplinary grand round. The grand round on the Bradford neonatal unit occurs in the main intensive care room with a large staff presence including all available medical staff, senior and junior nursing staff, pharmacists, outreach team and administrative team. Team members were invited to suggest changes and improvements to the action points.
The updated poster was then dissem-inated in three main ways:
- Displayed around the department including on the backs of toilet doors (where most reading occurs) and on the doctors’ jobs book.
- Posted on staff private social media groups (senior and junior doctors’ WhatsApp groups and nurses’ Facebook page).
- Presented at nursing handovers.
The Trust’s information governance department was consulted prior to the start of this project regarding the use of social media. Senior staff were keen to implement this idea as they were aware that this method of communication was particularly appealing to younger doctors and nurses. Some more senior consultants were even persuaded to download WhatsApp. The information governance department’s guidelines were adhered to about how to circulate information safely. The majority of staff check the staff social media groups on a very frequent basis. They are used for work purposes and felt to be the most reliable way (compared to email) to contact the majority of staff. Distributing the posters on these private groups enabled those who were not at the grand round to access the learning.
Feedback from the team early on was that the messages on the poster felt quite negative. The decision was made to start including at least one positive point or good news story each week. Lessons from morbidity and mortality reviews, serious incidents, issues raised by the pharmacy team and patient safety alerts were also included in the weekly learning posters.
This project started in March 2017 with the initial team of a consultant, ANNP and junior doctor. The team expanded to include nurses of multiple grades and a few junior doctors who were recruited on to the team at the start of each medical rotation. The team worked together and shared roles such as designing the poster.
One year after starting this project, in March 2018, a review of the risk incidents was undertaken and a qualitative questionnaire using Likert scales was distributed to all neonatal staff using SurveyMonkey to gather feedback about the weekly learning project.
Results
In the 12 months prior to the start of this project there were a total of 15 incident themes communicated to the team via the monthly newsletter. As previously mentioned, these themes could have incorporated multiple incident reports, or were standalone incidents.
The new system was established in April 2017. Over the next 12 months, learning points from 233 risk incidents were actively communicated to the team using this platform. Although this is comparing individual risk incidents to risk themes, this is a 15-fold increase from the previous year. Between August 2017 and March 2018, 202 incidents were reported and reviewed of which 159 (78.7%) were selected for discussion using this platform.
The team was able to note recurring incidents due to the frequency of the presentations and changes to practice were made.
Between July and December 2017 there were eight incidents related to breast milk. These included equipment failure, breast milk being administered to the wrong baby and expired milk in the fridge. At this time there was a small kitchen with one large fridge and one large freezer. Both were often overstocked, there were frequent failures of the freezer and it was difficult to distinguish between the milks due to cramped space. In December 2017 fridges were introduced into the clinical areas for parents to access and two freezers were placed in the milk kitchen. Between July and December 2018 there was one breast milk-associated error and this was some expired breast milk found in the fridge. There is now an allocated breastfeeding support worker on duty each shift whose roles include cleaning fridges and checking stock. This will hopefully further reduce such incidents.
In the six months after the introduction of the weekly learning there were four incidents related to antibiotic prescribing and administration on the postnatal ward. These incidents included gentamicin being given at 12 hours after the previous dose, gentamicin given without a gentamicin level, and missed doses. As a result guidelines were changed, so that Cefotaxime was used as a single agent in all babies requiring antibiotics after 36 hours. In the six months since these errors were spotted and the guidelines were changed to Cefotaxime, there were no postnatal antibiotic incidents.
There were 56 responses to the staff qualitative survey completed by various members of the MDT; 96% of respondents ‘strongly agreed’ or ‘agreed’ that the weekly risk learning was a useful learning tool while 79% of staff either ‘strongly agreed’ or ‘agreed’ that this new project had changed aspects of their clinical practice (FIGURE 3). Some of the comments from the survey can be seen in FIGURE 4.
Areas identified for improvement from the survey included learning points being mainly applicable to medical staff. At the time of the staff feedback the risk team did not include any junior nurses. Their inclusion in the current team helps to keep the posters more balanced.
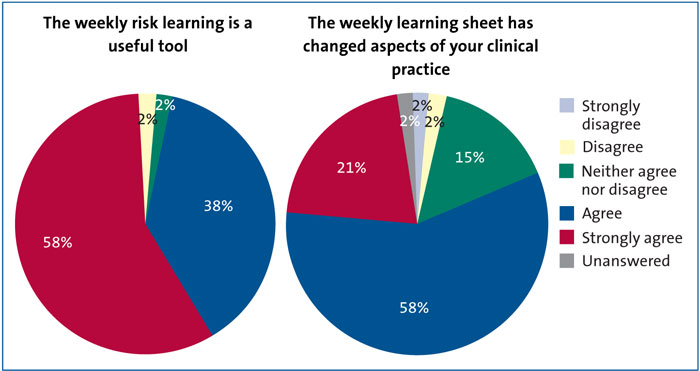
FIGURE 3 Responses to the staff feedback questionnaire (n=56).
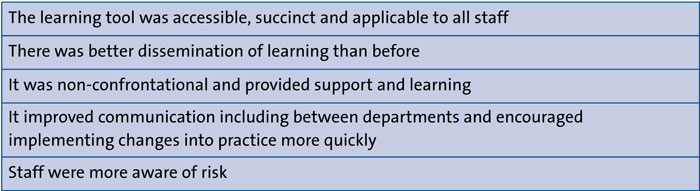
FIGURE 4 Responses to the staff feedback questionnaire (n=56).
Discussion
The aim of this project was to overcome the ‘communication bottleneck’ of risk incident learning. We replaced the lengthy monthly e-newsletters with a weekly aesthetic poster with succinct and clear learning points and used a multi-pronged approach to disseminate this information among the team. We increased the number of incidents being actively communicated to the team 15-fold and communicated >75% of all incidents reported using this method. The frequent and active addressing of risk incidents has encouraged staff to feel that reporting incidents is more meaningful and worthwhile.
The presentation of the poster at the weekly grand round at a time when there is large multidisciplinary staff presence has helped with staff engagement in this project. The open discussion of the poster, inviting comments from the team, createsa non-dictatorial and non-punitive atmosphere for discussing risk incidents and actually encourages positive team involvement. The frequent team discussions of incidents on the neonatal unit has enabled earlier detection of recurring themes so that changes to procedures and practice are made earlier (eg changing postnatal antibiotic guidance) resulting in a demonstrable reduction in associated incidents.
Publicising the concise, and often fun, weekly poster on the private staff social media groups results in quick and effective dissemination of the learning from risk incidents. It has been well received throughout the department and allows for a multidisciplinary approach to continuous learning from risk incidents. As this project has evolved it has become the principal method for communication of changes in practice and updates within the team.
The involvement of junior staff members in the risk team offers them a greater understanding and experience of risk management, helping to develop future interests. ‘Highlights’ of learning from the preceding six months are also presented to the new junior doctors at each induction.
The overall process is hugely time saving for the risk team. Reviewing incidents on a weekly basis and with a larger team has meant that it is quicker to review and suggest appropriate action points.
This project has improved awareness and has resulted in rapid and timely dissemin-ation of learning from risk incidents. This has now been adopted in several other departments in the hospital and, following presentation at a regional meeting, in other neonatal units within the Yorkshire and Humber Operational Delivery Network.
Or read this article in our
Tablet/iPad edition
- A multi-pronged approach including social media has resulted in improved awareness and rapid dissemination of learning from risk incidents.
- Risk incidents fed back to the team have increased 15-fold since introducing this new method, suggesting greater staff involvement.
- Weekly discussions at grand round have led to recurrent errors being identified earlier and effective changes made.
Also published in Infant:
