

The implications and considerations of redirecting care in a local neonatal unit
This paper explores the case of a very sick infant in a local neonatal unit (LNU) for whom we unfortunately had to redirect care from intensive to palliative. It was decided that it was in the best interests of the baby and the parents to do so in the LNU, rather than transfer him to the tertiary neonatal unit. This article describes the benefits and challenges of redirecting care in the LNU, and how other LNUs can develop tools to empower themselves to confidently provide redirection of care in these unusual cases.
Arameh Aghababaie1
Paediatric ST3 Doctor
a.aghababaie@nhs.net
Catherine Douch2
Paediatric ST5 Doctor
Yana Belosludtseva3
Neonatal Consultant
1Homerton Health NHS Foundation Trust, London
2Royal Free London NHS Foundation Trust
3Barts Health NHS Foundation Trust, London
Advancements in neonatal medicine have enabled us to maintain life in babies who might previously have been considered unviable. Where possible, these babies are transferred to a tertiary unit in utero to avoid enduring the risks of transfer. If delivered in LNUs, they are transferred to the tertiary centre once stabilised. In some cases, where the predicted outcome is poor, redirection of care may be considered, which raises the question: where is the most appropriate location for redirection of care?
As neonatologists, our role involves both resuscitation and active intensive care, as well as considering redirection of care in cases where ongoing treatment is not in the best interests of the baby. Situations such as these can cause distress to staff and present with particular challenges in a LNU setting where treatment escalation is limited and staff have less experience to care for such babies.1
Staff may be reluctant to redirect care within the LNU setting as they wonder whether the baby should be transferred to a tertiary centre for a second opinion, or because a tertiary centre may be a more appropriate setting for redirection of care.
To illustrate the nuances of this decision-making process, we will discuss the case of an extremely premature baby born in very poor condition, with a poor predicted outcome, who had care redirected in the LNU where he was delivered. This example demonstrates valuable learning points relating to the implications of redirecting care in a LNU setting, what this means for the family and staff, and how teams in district general hospitals can be supported in such circumstances.
The case: part one
A gravida 4 para 3 female was brought to hospital via ambulance due to abdominal pain and vaginal bleeding at 28+2 weeks of her pregnancy. She had a background of gestational diabetes controlled by metformin. All ultrasound scans had been normal prior to admission. The maternal blood group was B positive with no atypical antibodies and the maternal serology was protective.
Upon arrival at the hospital her membranes were ruptured (the timing of which was unknown), her cervix was 6cm dilated, she was having four contractions in 10 minutes and she was heavily bleeding per vagina. Cardiotocography (CTG) was performed, which was severely pathological with a fetal heart rate of 30-40bpm (beats per minute), and the mother went into pulseless electrical activity (PEA) arrest requiring adrenaline and fluid resusci-tation. She was immediately transferred to theatre for a category 1 emergency caesarean section under general anaesthetic. No antenatal steroids or magnesium sulphate were administered. During the caesarean, she was found to have a complete placental abruption.
A male infant was delivered at 28+2 weeks’ gestation weighing 1,010g (20th centile). The baby was born in extremely poor condition with Apgar scores of 0, 0, 0. He was intubated at two minutes of age on the first attempt with a size 2.5 endotracheal tube (ETT) at 6.5cm to the lips. He received chest compressions until 20 minutes of life, with his first audible heart rate at 20 minutes. During resuscitation he received the following via an umbilical venous catheter and peripheral venous cannula inserted in theatre:
- three 10μg/kg doses of 1:10,000 adrenaline
- 2mL/kg of 4.2% sodium bicarbonate
- 2.5mL/kg of 10% dextrose bolus
- 20mL/kg of 0.9% sodium chloride bolus
- 30mL/kg of packed red blood cells.
The cord gases are presented in TABLE 1.
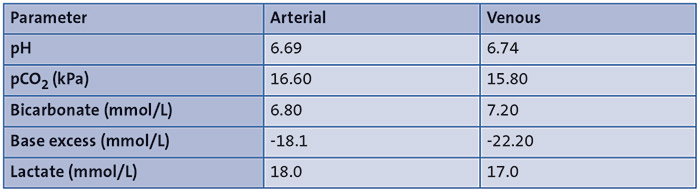
TABLE 1 The arterial and venous cord gases, which show a severe mixed respiratory and metabolic acidosis.
The baby was transferred to the neonatal unit at 30 minutes of life. He was ventilated on synchronised intermittent mandatory ventilation (SIMV) mode at pressures of 25/5 cmH2O, with a rate of 60 breaths per minute and an FiO2 of 100%, maintaining saturations between 30-50%. His heart rate was 80-100bpm and mean arterial pressure was 19mmHg. At 45 minutes of life, while he was being transferred from the transport incubator to the unit incubator, the ETT dislodged causing desaturation to 10-20% and a bradycardia of 40-60bpm. He was reintubated successfully on the first attempt with a size 2.5 ETT fixed at 6.5cm to the lips. This prompted another 10 minutes of chest compressions and a further 10μg/kg dose of 1:10,000 adrenaline. After which his bradycardia resolved and saturations rose to their previous baseline.
Question 1. What would be your next step?
- Give surfactant
- Insert central lines
- Start inotropes
- Contact the neonatal transport team and tertiary unit.
Question 2. What do you predict the outcome will be for the baby?
- The baby may survive but with long-term disabilities
- The baby will likely pass away within the next 24 hours
- The baby may survive and live a normal, healthy life.
A chest X-ray was performed, which showed the ETT was correctly placed between T1 and T2, with a complete white-out of both lung fields. Umbilical venous and arterial lines were sited and infusions of 10% dextrose and morphine were commenced. Our neonatal transport team and local tertiary unit were contacted and they simultaneously advised not to proceed with active treatment (ie surfactant administration and inotropes).
An arterial gas taken at one hour of life showed an unrecordable pH and pCO2, and a lactate of 19mmol/L.
An arterial blood gas taken four hours after admission showed a pH of 6.82, pCO2=7.59kPa, base excess= -22.1mmol/L, bicarbonate 8.7mmol/L and lactate 18mmol/L.
Question 3. What is the most likely differential diagnosis?
- Sepsis
- Severe perinatal hypoxia
- Respiratory distress syndrome
- Hypovolaemic shock
- All of the above.
At four hours of age, the baby developed clinical seizures with a corresponding cerebral function monitoring trace and was started on a midazolam infusion. He continued to have abnormal jerky movements although this improved with the infusion. A cranial ultrasound showed brightness throughout but no intraventricular haemorrhages.
Question 4. Do you think transferring this baby out to a tertiary unit is in the baby’s best interests?
- Yes - this is a complex baby who is in labile condition and requires intensive input and monitoring and this is best done in a tertiary unit
- Yes - this baby will likely require redirection of care and this is best done in a tertiary unit
- No - the baby is too unstable for transfer at this point and requires further stabilisation before he can be transferred to a tertiary unit
- d. No - the baby has a poor prognosis and it would be best to redirect care at his LNU.
Question 5. What is the best way to come to a decision about redirecting care in a LNU?
- Discussing with the parents
- Discussing with the neonatal transport team
- Discussing with tertiary neonatal intensive care unit (NICU) consultant colleagues
- All of the above.
Discussion
Decision-making regarding redirection of care in neonatal practice
Advances in perinatal medicine and neonatal care have resulted in markedly improved survival rates, thus redirection of care decisions often concern the quality of life in those who survive. It is now estimated that more than 80% of deaths in neonatal units result from redirecting care.2 Deciding whether to redirect care is especially complicated in babies who survive a prolonged resuscitation, as in this case, and it can be difficult to ascertain for how long the baby will survive.3 The baby lies at the core of these decisions and we have to consider whether prolonging treatment in these cases is in their best interests or not.3
Recognising that intensive care may not be in the baby’s best interests is a difficult conclusion for clinicians to reach and there are many barriers to delivering optimal redirection of care that need to be overcome:
1. Decision-making: there is a paucity of formal training relating to redirecting care in neonatal medicine in undergraduate or postgraduate medical education, resulting in a limited capacity to make decisions related to redirecting care.4 This was reflected in a 2013 study in which only a third of neonatal doctors reported feeling competent in redirecting care and only one third of neonatal nurses felt they had received any training in supporting families of babies whose care was being redirected.5,6 It is therefore imperative that educational programmes address this gap in knowledge as a starting point to optimise local practices.7 In a local neonatal setting, it is also beneficial to manage cases of redirection of care in collaboration with a tertiary centre for a second opinion.
2. Out of the comfort-zone: not only are we faced with decisions about how long to continue intensive treatment for, but sometimes the decision to be made is: ‘Do we initiate intensive treatment at all?’ Providing comfort and alleviating suffering lie at the heart of redirecting care. But these principles are often conflicting with the culture of intensive care medicine. Intensive treatments often start on autopilot from the moment a baby is admitted. For example, this baby had central lines inserted and antibiotics were initiated as soon as the baby was brought to the neonatal unit. This can form a barrier to effectively redirecting care in neonatal medicine.8 Therefore, active and targeted training to improve confidence and competence in redirecting care will help to bridge this gap.
3. Communication: parents should be recognised as a member of the team caring for their own baby; thus, it is important for us to encourage open discussion with the parents throughout. Neonatal practitioners can feel apprehensive when communicating with parents of babies who are dying, for fear of causing them further distress. 6 Early and in-depth discussions and decision-making has been shown to improve the quality of care in babies whose care was being redirected. Simultaneously, a lack of communication increases parental distress, therefore it is integral that these conversations are raised and integrated into conversations as soon as a neonate is recognised as nearing the end of life – this may even begin antenatally in some cases.9
Communication should balance sympathy and empathy with honesty and clarity, acknowledging the emotional challenges to the family, giving them time to process.10 Decisions should be made in clinical partnership with families, to the point which they desire and are capable of. Individual family preferences, beliefs and expectations should also be taken into consideration. A study of different communication frameworks when involving parents in critical care decision-making showed that when clinicians communicated ‘options’ to parents, rather than ‘recommendations’, it allowed for more opportunity for questions and collaboration and involvement, should the parents wish, and in turn created more of a sense of ease and control for parents during a difficult process.11 This is good practice and fosters a relationship based on trust between both parties and is less likely to result in conflict.10 Parents should be reassured their baby will continue to receive care and ongoing assessment to avoid feeling abandoned when care is redirected.12
4. Support: there must be a focus on psychological safety for both parents and staff. Parents of babies whose care is being redirected are at significant risk of emotional trauma and it is suggested that neonatal units should have access to a clinical psychologist and spiritual support, as well as support from religious leaders.7,13,14 Parents should also be encouraged to make memories with their baby, for example, taking photographs, dressing the baby, taking handprints, and keeping other mementos such as locks of hair, which can be extremely important to families. As for neonatal staff, they should always debrief after a baby has passed following a period of redirection, to promote open discussion and have an opportunity to reflect.7 This should be well publicised and potentially be repeated to allow all staff involved to attend.
In instances of clinical uncertainty or disagreement between the neonatal team and family, it can be useful to invite a second opinion. If the conflicting opinions continue and fail to resolve with mediation, these disputes can be settled with an independent arbitration or in court.15 Legal action is best avoided if possible; however, if all options have been exhausted, then it may be in the best interests of the baby.16 Although the court’s attitude is strongly in favour of preserving life, their role in redirection of care decision-making is to provide objective judgement of the situation, taking the relevant clinical considerations, intolerability of treatment and impact on quality of life into account.16 Collective decision making between teams and parents reduces the incidence of legal action.3 This collective decision-making, ultimately drives an ethos of delivering care in the best interests of the baby, while showing consideration for all parties involved.
The case: part two
A three-way conference call was arranged with the local neonatal consultant, the neonatal transport consultant and the tertiary neonatal consultant. Discussions took place regarding the prognosis of the baby and whether it would be in his best interests to be transferred to a tertiary neonatal unit. It was a well-coordinated discussion between the teams, providing clinical and emotional support to the team in the LNU. The general consensus was that the long-term outcomes would be extremely poor and the baby was unlikely to survive. Thus, the decision was made between all the consultants that transferring the baby was not in his best interests.
The local neonatal team again expressed concerns about whether a transfer may be appropriate. The tertiary consultant visited the baby to give an in-person second opinion and, after their assessment, agreed that redirection of care was still in the best interests of the baby.
This led to a further meeting with the parents, involving the local and tertiary NICU consultants, and the obstetric and midwifery teams. Following this meeting, it was mutually agreed that the baby’s care would be redirected to focus on comfort. The parents wished for him to remain intubated, which was respected. However, it was agreed that chest compressions, blood tests and inotropes would be inappropriate.
The baby sadly passed away at 31 hours of age. The parents were given time to hold their baby and were seen by the chaplain. He was christened as per the parents’ wishes. A month later, the parents were invited for a follow-up appointment with the local neonatal consultant involved, to answer any questions they had about the baby’s care and his unfortunate passing and to receive ongoing support.
Discussion
Redirection of care in a LNU
Although LNUs have less exposure to redirecting care, it is important that they are capable of redirecting care in such cases. There are several benefits of doing so in the baby’s LNU:
- it keeps families together, allowing parents more time with their baby to make memories
- unnecessary patient transfers are avoided and tertiary neonatal beds are available for other admissions
- it demonstrates unified clinical decision-making and manages parental expectations. It is a complex message for parents to understand that their baby is being transferred to a unit capable of more intensive treatment, only for care to be redirected. These mixed messages can cause additional emotional trauma to families.
In our case, as the mother was very unwell post-partum, had the baby been transferred to a tertiary neonatal unit she would not have had any time with her son before he passed away.
Second opinions are also very valuable, especially in a district general hospital setting. Babies who are very unwell or extremely premature or born with severe congenital abnormalities are usually delivered at, or transferred to, tertiary neonatal units once delivered. These are the babies who have the highest incidence of mortality, thus tertiary neonatal units have more robust experience of redirection of care. LNUs that are infrequently faced with these cases have a more limited experience in neonatal redirection of care.4 Therefore, obtaining a second opinion from a tertiary unit, and having them involved in the care of the baby, can be invaluable in helping make an informed decision and communicating this to the parents. A second opinion is also useful for legal purposes, particularly when the parents do not agree with the decision to redirect care.16 In our case, we sought a second opinion and held a multidisciplinary team (MDT) meeting involving the parents regarding the baby’s prognosis and care. The input from two neonatal consultants was reported to be of great value to the parents, who felt reassured that the tertiary NICU consultant agreed with our plan to redirect care. Hosting an MDT meeting with the parents ensured continuity of care and collaboration and made the parents feel involved in the decision-making process. Additionally, our local neonatal team felt supported with the clinical advice and also emotionally supported by working in collaboration with a larger centre.
Providing support for the local neonatal team and parents is also very important as this situation will be distressing for all involved, as mentioned previously.7,13,14 In our case, the local neonatal team were given multiple opportunities to debrief and a follow-up appointment was made for the parents to meet with the local neonatal consultant, as an opportunity for them to reflect, debrief, ask questions and receive ongoing support during this difficult time.
Overall, this case is an excellent example of how a LNU made the decision to redirect care for an extremely unwell premature baby, with the support of the tertiary neonatal unit and the MDT. This was achieved with consistent parental input from early on, ensuring all their wishes were respected and that their limited time with their baby was not compromised by transferring to the tertiary neonatal unit. They were also provided with ongoing support during the baby’s short life and after the baby’s passing. However, this case also highlights our shortfalls – although there were opportunities for the local neonatal team to debrief, these sessions were sporadic and consultant-dependent. Since this case, our unit has formed a group to regularly debrief about neonatal resuscitations, cases where care is redirected, and to offer peer support. We also noted that we have no dedicated psychological support for families or staff, which is an area flagged for improvement.
Conclusion
In this particular case, the process of decision-making was facilitated by the support received from the tertiary neonatal unit via teleconferencing and eventually a face-to-face review of the baby and joint discussion with the family. Having their involvement helped to aid this emotionally and mentally challenging process for our team and the family. We would like to encourage other tertiary care units and district general hospitals to consider collaborating in this way when faced with difficult situations.
Footnote
This article is loosely based on a real case but all data have been changed and anonymised to protect the identity of the child.
Or read this article in our
Tablet/iPad edition
- Babies that are born sick or extremely preterm or with severe congenital abnormalities in a LNU are often transferred to a tertiary neonatal unit once stabilised.
- These babies have the highest incidence of mortality and, therefore, tertiary neonatal units have more robust experience of redirection of care in neonates.
- On occasion, it may not be possible or in the baby’s best interests to transfer to the tertiary unit and it may be appropriate to redirect care from intensive to palliative in the LNU.
Also published in Infant:
