

pCO2 variation in elective transfers of infants on non-invasive respiratory support
Repatriations to local care are an integral part of the remit of neonatal transport teams, with a significant proportion of these infants being transferred on non-invasive respiratory support. A routine blood gas on arrival at the receiving unit is part of our team’s current practice for elective repatriations of infants on non-invasive respiratory support. Through retrospective review of data from a large number of patients transferred, we aimed to determine if there was a significant change in the partial pressure of carbon dioxide (pCO2) on arrival at the receiving unit, and to identify a subgroup of infants most at risk of an increase in pCO2.
Catarina Couto
Clinical Fellow
catarina.couto@uhs.nhs.uk
Mira Parmar
Neonatal Grid Trainee
Julia Arthur
Consultant Neonatologist, PaNDR
Consultant Neonatologist, Neonatal Lead for PaNDR
Sue Broster
Consultant Neonatologist, Clinical Director for PaNDR
Paediatric and Neonatal Decision Support and Retrieval (PaNDR) service, Cambridge University Hospitals
Elective repatriations of infants represent a significant proportion of transfers undertaken by neonatal transport services. While these are non-emergency transfers, they still frequently involve infants on some form of respiratory support.
The Paediatric and Neonatal Decision Support and Retrieval (PaNDR) service provides advice, critical care retrievals, transfers for specialist care and repatriation for neonatal patients across the East of England.1 Our team undertakes around 600 elective repatriations per year, of which a third are on non-invasive ventilation. In our service, infants receiving invasive ventilation are classified as ‘planned emergencies’ rather than repatriations as they require more complex planning and care.
A routine capillary blood gas on arrival at the receiving unit is part of our practice for repatriations of stable infants on non-invasive respiratory support – continuous positive airway pressure (CPAP), high flow nasal cannula (HFNC) or low flow nasal cannula (LFNC). The rationale being that we would document a respiratory deterioration en route. A heel prick is a painful procedure, however, and the blood gas on arrival is not necessarily actionable. It is likely the receiving team would let the infant settle and repeat a second blood gas before making changes to their ventilatory support based on that initial pCO2. Hence, we decided to study the variation of pCO2 in these infants.
Our primary objective was to determine if there is a significant change in the pCO2 on arrival compared to the pCO2 prior to transfer, justifying our current practice. As a secondary objective, we aimed to identify subgroups most at risk of increase in pCO2 as a marker of respiratory deterioration.
Methods
We performed a retrospective cohort study of infants referred to the PaNDR neonatal team for elective repatriation from January to December 2021. Data from all infants receiving non-invasive respiratory support prior to elective repatriation were reviewed. Exclusion criteria were:
- blood gas on arrival not performed or not documented
- documented blood gas on the referring unit performed more than two days prior to the transfer or date not documented
- blood gas on the referring and receiving units from different sampling sites (if the site was not documented, we assumed it was a capillary sample).
Subgroups analysed included:
- corrected gestational age (CGA) (<28 weeks, 28-31+6 weeks, 32-36+6 weeks and ≥37 weeks)
- current weight (<1,000g, 1,000-1,499g, 1,500-1,999g and ≥2,000g)
- mode of respiratory support (CPAP, HFNC and LFNC)
- parameters of HFNC (≤4L/min and >4L/min) and CPAP (≤5cmH2O and >5cmH2O)
- FiO2 requirement prior to transfer (<0.3 and ≥0.3)
- infants who required an increase in settings during transfer (any increase ≥1L/min/1cmH2O and/or increase in FiO2 ≥0.1 at arrival)
- journey duration (≤60min, 61-119 min and ≥120 min).
A paired sample t-test was used to compare pCO2 prior to transfer and pCO2 on arrival. A p-value <0.05 was considered statistically significant. The absolute difference between pCO2 on arrival and pCO2 prior to transfer was also analysed.
Results
We identified 229 encounters that fulfilled inclusion criteria, of which 56 were excluded, leaving a total of 173 encounters for analysis (FIGURE 1), corresponding to 166 infants. Around half the infants included were under 31+6 weeks CGA and under 1,500g. About three quarters were on HFNC with only nine infants on LFNC. The journey lasted between one and two hours for the majority of infants.
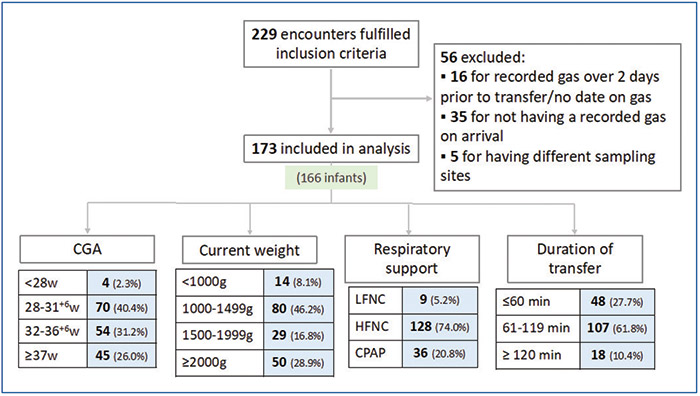
FIGURE 1 Encounters included in the analysis.
The mean pCO2 prior to transfer was 6.65 ± 1.17kPa and on arrival at the receiving unit was 6.59 ± 1.20kPa (p=0.35; FIGURE 2).
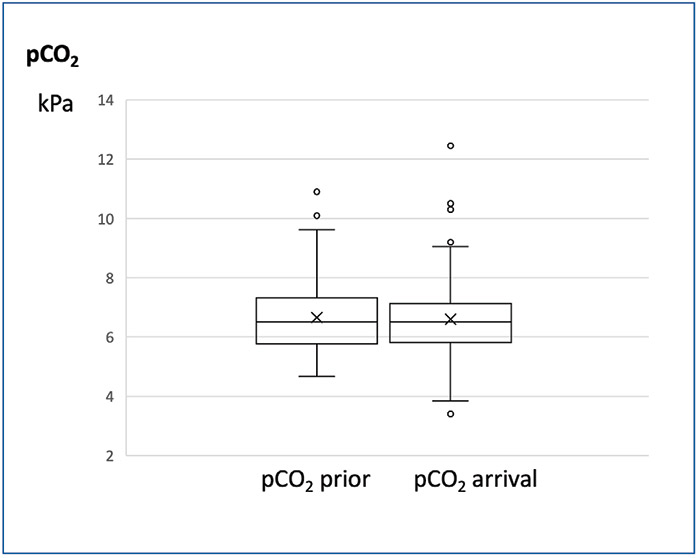
FIGURE 2 pCO2 prior to transfer and on arrival at the receiving unit.
Of the subgroup analysis (TABLE 1), only infants between 28 weeks and 31+6 weeks CGA showed a trend towards a statistically, but not clinically, significant increase in pCO2 on arrival (M ± SD 6.44 ± 0.98 and 6.59 ± 0.93; p=0.06). Infants on different types of non-invasive respiratory support (CPAP, HFNC, LFNC) and with different oxygen requirements (FiO2 <0.3 and ≥0.3) did not have an increase in pCO2 on arrival at the receiving unit.
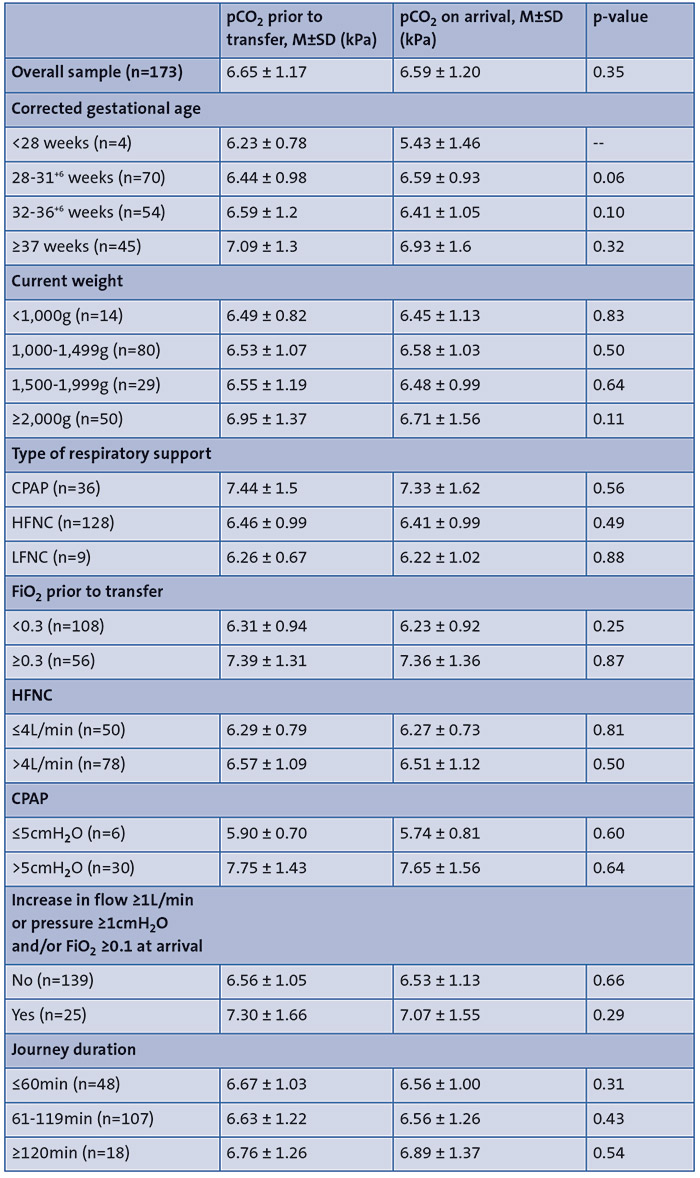
TABLE 1 pCO2 prior to transfer and on arrival: subgroup analysis.
The absolute difference between pCO2 on arrival and pCO2 prior to transfer followed a normal distribution around a mean of -0.04kPa ± 0.84 (FIGURE 3). The maximum increase in pCO2 was 1.84kPa, with one outlier showing an increase of 2.83kPa and three outliers displaying a decrease in pCO2 between 2.21 and 3.87kPa. All the outliers corresponded to infants on FiO2 ≥0.3 prior to transfer.
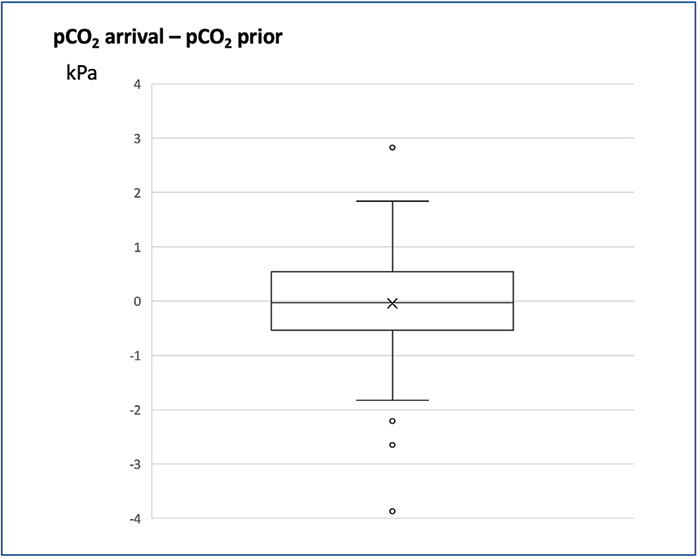
FIGURE 3 Absolute difference between pCO2 on arrival at the receiving unit and pCO2 prior to transfer.
Discussion
Out of the 229 encounters that fulfilled the inclusion criteria, 56 (24.4%) had to be excluded, mainly for not having a blood gas on arrival. The clinical team’s decision not to perform a blood gas on some infants could potentially reflect the clinical stability of the patient and better patient demographics and baseline ventilation status (such as higher CGA and weight, lower respiratory support settings), skewing the final sample towards babies that were thought to be more at risk of increase in pCO2. When compared with the total cohort, the excluded encounters were demographically similar in terms of CGA and weight, but were more likely to be from babies on LFNC who were perhaps considered more clinically robust than those on CPAP or HFNC.
In the overall sample there was no change in mean pCO2 on arrival compared to mean pCO2 prior to the transfer and the absolute difference followed a normal distribution around a mean of zero with a maximum and minimum of around 1.8kPa. All the outliers were infants on FiO2 ≥0.3 suggesting that these infants may have a wider variation in pCO2. A change of pCO2 of up to 1.8kPa in an infant that has just been transferred does not necessarily warrant action, particularly if the infant is otherwise well. It is important to note that our sample included some patients who had a clinical deterioration en route, such as apnoeas requiring stimulation or frequent desaturations and bradycardia. It was reassuring that even when including these infants, the maximum increase in pCO2 was not at a level where the receiving team would have needed to act on it.
In the subgroup analysis, we used CGA and current weight rather than gestational age and weight at birth because we transfer preterm infants across a range of corrected gestations and weight. An extremely preterm infant term-corrected has a different maturity level than a younger infant. This means that in our sample term-corrected infants who were born extremely preterm, were classified in the same gestational age group as their term counterparts, even though the pathology behind the need for non-invasive respiratory support is likely different.
Infants between 28 weeks and 31+6 weeks CGA showed a non-statistically or clinically significant trend towards a higher pCO2 on arrival. We only completed four repatriations of infants under 28 weeks CGA. In this group, the mean pCO2 on arrival decreased, suggesting that there was no deterioration en route, but considering the vulnerability of these infants, we would need a larger sample size to be able to safely suggest the discontinuation of a routine blood gas on arrival. The current weight and journey duration were also not determinant of a significant change in pCO2 on arrival.
As expected, infants on CPAP and/or FiO2 ≥0.3 had a higher pCO2 compared to infants on HFNC and/or FiO2 <0.3. Babies on CPAP and with higher oxygen requirements likely represent preterm infants with evolving bronchopulmonary dysplasia, thus explaining the higher baseline pCO2. They did not, however, have a significant change in pCO2 on arrival to the referring unit. Similarly, infants on higher settings of HFNC or CPAP did not display a significant change in their pCO2 compared to infants on lower settings. Infants with a deterioration en route where the team deemed it necessary to increase the settings on the HFNC/CPAP (flow ≥1L/min or pressure ≥1cmH2O) and/or FiO2 ≥0.1 at the time of arrival had a non-statistically or clinically significant decrease in pCO2.
Limitations of this work include its retrospective design relying on accurate documentation and data collection, the heterogeneity of our sample and the significant proportion of encounters excluded from the analysis.
Conclusions
There was no significant change in pCO2 for infants on non-invasive respiratory support undergoing elective repatriation, hence we can safely consider discontinuing our current practice of a routine blood gas on arrival for these infants. It is reasonable to maintain this practice in infants with a CGA below 28 weeks, particularly considering the very small number of infants studied in this age group and their potential for greater fragility. Despite not displaying a change in pCO2 in our study, we recommend as good practice performing a blood gas on arrival for infants with a clinical deterioration en route.
Or read this article in our
Tablet/iPad edition
- We found no significant change in pCO2 on arrival at the receiving unit in infants undergoing elective repatriations on non-invasive respiratory support.
- A routine blood gas on arrival at the receiving unit following elective repatriations is unnecessary.
Also published in Infant:
