

Simulation-based curriculum development and team training for neonatal transport: a Canadian experience
The transport of critically ill newborns requires a highly competent team with proven skills for caring for sick neonates. Simulation provides an opportunity to allow transport team members to both acquire and maintain skills specific to their role. This article will shed light on the importance of simulation training for neonatal and paediatric transport teams as well as provide a practical approach to building a transport simulation programme.
Wail Seleem1
MD
wseleem@manitoba-physicians.ca
Debbie Fraser2,3
MN, CNEON(C), Associate Professor, Neonatal Nurse Practitioner
Ganesh Srinivasan1
MBBS, MD, DM
Michael Narvey1
MD, Associate Professor, Medical Director of the Child Health Transport Team
1Department of Neonatology, Health Sciences Center, University of Manitoba, Canada
2Faculty of Health Disciplines, Athabasca University, Canada
3NICU, St Boniface Hospital, Winnipeg, Canada
Neonatal transport medicine is a unique, challenging specialty that evolved during the 1960s and 70s as a consequence of the regionalisation of neonatal and paediatric specialties.1 In Canada, neonatal transport teams developed as a result of regionalised secondary and tertiary care for severely ill newborns, which required neonates to be transported between neonatal services. The Canadian Neonatal Transport Network is made up of Canada’s 16 neonatal transport teams, who perform approximately 5,000 neonatal interfacility transports each year.2 However, the demographics of the teams – the number of transports, mode of transfer, and team composition – differ significantly.
In Manitoba, which is the fifth most populous province or territory in Canada, the Neonatal Transport Service was founded in 1983. The team currently consists of 12 nurse clinicians and 13 advanced respiratory therapists. The team covers Manitoba (648,000km2), Northwestern Ontario (470,000km2) and Nunavut (2 million km2). On an annual basis, there is an average of 700 neonatal and paediatric transports.
For the past eight years, a simulation transport programme has been in place in Manitoba. In addition to procedural skills, transport team members must also understand flight physiology, mitigate the adverse effects of the transport environ-ment (ie temperature fluctuation, vibration and noise), work in the confined environments of a small plane or helicopter, and comfortably assess a patient with or without the use of accurate monitoring equipment.3 In addition to these challenging air medical settings there are a variety of risks associated with neonatal transport, such as equipment failure (ventilators, warmers, and infusion pumps) or ambulance collisions and, in rare cases, accidents involving helicopters or airplanes that have ended in tragedy. When infants and children are transported by non-specialised transport teams, adverse events such as airway compromise, loss of vascular access or need for cardio-pulmonary resuscitation have been reported. Studies have demonstrated that having a specialised neonatal transport team is associated with improved outcomes related to morbidity and mortality.4
Acquisition and maintenance of transport competencies is challenging but achievable through ‘deliberate practice’. Ericson and colleagues highlight the importance of deliberate practice of a skill through multiple repetitions and provision of constructive feedback as key to developing expertise and ensuring the skill is being learned correctly.5
Simulation-based transport education
Using simulation to replicate clinical scenarios has been the subject of extensive research and it is now generally accepted that simulation-based learning assists in developing health professionals’ knowledge, skills and attitudes while protecting patients from unnecessary risks.6,7 As a result, offering simulation-based training is a strategy that adheres to the highest educational standards and ethical principles and should be tailored to the unique characteristics of each organisation.8
High fidelity simulation for transport team training improves team members’ confidence in their clinical and communications skills, improves their knowledge base, equipment utilisation, and communication strategies and behavioural performance.9 Therefore, this training method has the potential to have a profound impact on the ability of teams to provide optimal care for critically ill children.10-15
With the transition to competency-based medical education, the interplay between simulation-based procedural training and supervised clinical experience is essential for achievement of competence leading to mastery. The skills requirements for transport teams that can be enhanced with the use of simulation include: technical and functional expertise training, problem-solving and decision-making skills, teamwork skills and interpersonal communication techniques.
Technical and functional expertise training
Simulation enables repeated procedural exposure in a safe environment without compromising patient safety; ‘see a lot, simulate and train a lot, teach and assist a lot, and harm none’.16 Integrating skill objectives into event-based simulation scenarios can provide repeated practice opportunities to perform skills within the context of the team training in a controlled safe environment.4
Communication and teamwork
Crisis resource management (CRM) refers to a set of principles (TABLE 1) dealing with cognitive and interpersonal behaviours that contribute to optimal team performance.17 Professor of Anaesthesiology David Gaba and his colleagues, transferred and adapted CRM to medicine, calling it ‘anaesthesia crisis resource management’.18 Simulation-based CRM training programmes were soon developed in other high-risk, high-acuity medical specialties, including neonatology.19
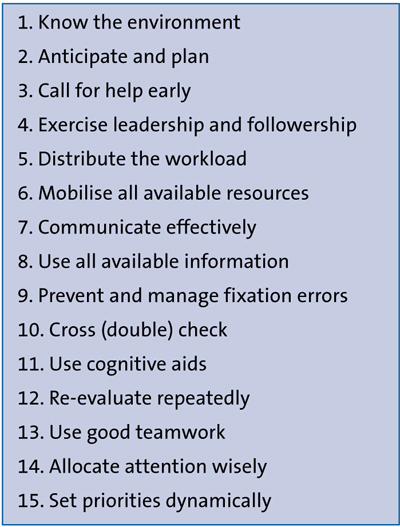
TABLE 1 The key features of CRM.20
Curriculum development for the transport team using simulation
Transport medicine is a unique, challenging and rapidly expanding discipline with its practitioners drawn from a mix of backgrounds. Using a structured curriculum development framework to design a simulation-based neonatal transport team training programme would ensure that training meets the needs of both the transport programme and the learners.
The process of creating a medical education curriculum can seem overwhelming at first, but when broken down into smaller pieces, it can be straightforward.21 Kern described a novel approach to curriculum development22 involving the following steps:
- general needs assessment
- targeted needs assessment
- goals and objectives
- educational strategies
- implementation
- evaluation and feedback.
A case study
Jonathan is a junior faculty member in the neonatal intensive care unit experienced in team training and simulation. He has been tasked by the neonatal and paediatric transport medical directors to develop a simulation-based neonatal transport curriculum. Jonathan uses Kern’s six steps as a guide to developing the curriculum.
1. General needs assessment
The first step in creating a great curriculum is to clearly identify the problem and then look for an appropriate solution. Jonathan and the director of the transport team meet and agree that the general needs are to develop a simulation-based neonatal transport curriculum that targets teamwork, skills, and competencies of the neonatal transport team. Identification of the general needs will aid in the development of the overall topic and objectives.
Targeted needs assessment
Jonathan intends to conduct targeted need assessments at two levels.
- Managerial level – by convening a meeting, designing and distributing a survey to the transport team leader, educator and medical director, enquiring about expectations, what the team needs to know, specific gaps, and how he can achieve that goal.
- Learner level – holding group orientation sessions followed by a survey asking transport team members what they want to learn and how they could progress as a learner.
After analysing the results of targeted needs assessments, Jonathan developed a list of topics and procedure skills that should be included in the curriculum.
The following is the suggested list of topics:
- hypoxic-ischaemic encephalopathy (HIE)
- congenital diaphragmatic hernia
- neonatal resuscitation
- pneumothorax
- meconium aspiration syndrome
- septic shock
- procedures: intubation, chest tube inser-tion and umbilical catheter insertion.
We will use HIE as the example for this article, with the remainder of the subject and procedure being applicable.
3. Goals and objectives
Use the SMART acronym to set the goals: (S) specific, (M) measurable, (A) attainable, (R) relevant, and (T) time-based.23 For example, the goal will be ‘competent transport team members provide safe and effective neonatal transport services’. Be specific: why exactly should you achieve this goal, is it achievable – can the learners meet the goals through simulation and can the learning objectives be met in the time allotted for the scenario? When writing a scenario, try to define three to five objectives, which could be cognitive (knowledge), affective (attitude), and psychomotor (behaviour).
While the goal can be more generalised, the transport team member (learner) objectives must be specific and measurable according to the selected topic. For example, the general objectives could be:
- Apply neonatal transport effectively
- Follow neonatal transport protocols
- Understand transport physiology
- Effective team work and communication.
The specific objectives for an HIE scenario are:
- Identify HIE (cooling protocol)
- Demonstrate an appreciation of HIE and transfusion protocols
- Good triage communication and pre-arrival advice
- Integration of referring staff in stabilisation of a complex case.
Creating a successful simulation scenario necessitates careful preparation and can be broken down into several stages (TABLE 2). Simulation scenarios are intended to evaluate, inform, and assist learners in identifying gaps in their knowledge or application of that knowledge. Writing cases is a different skill set to programming or operating a high-fidelity simulator, regardless of previous simulation experience.24 A well-designed scenario involves a script, an instructor document, a simulation technician document, and equipment requirements. The instructor document contains primary goals and objectives, a case description and instructor notes, which include ideal flow, anticipated learner errors, branch points, tips for keeping the scenario going and hard stops. The simulation technician document contains information on the required tools, props, and fidelity, as well as standardised patients, moulage, and manikins. The required degree of fidelity is determined by the priorities and objectives.
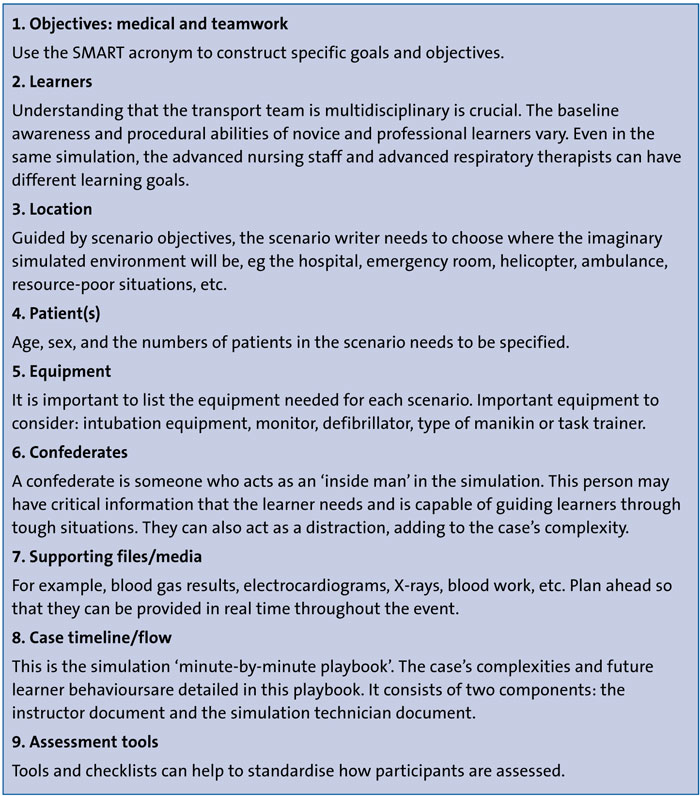
TABLE 2 Important components of a simulation case.24
When you write a simulation scenario, start by defining the learners, then move on to the desired results, which must involve the skills and behaviours that the learner may develop after participating in the simulation. A scenario design template is a written description and flow of the case. There are a variety of scenario models online. The following elements must be included in the scenario objectives:
- The intended result
- Critical actions checklist
- Setup for the simulation
- Scenario flow diagram with branch points
- Case narrative
- Notes from the instructor
- Debriefing strategy.
Jonathan and the transport team educator completed the final manuscript of the HIE case, which was reviewed by the transport medical director. A practice run in the simulation centre was scheduled to ensure that the scenario was ready for inclusion in the teaching curriculum.
4. Educational strategies
Using the simulation scenario’s objective as a guide, the method for achieving this objective can be a task trainer, a standardised patient, or computer-based simulation.
The curriculum developer must decide on the best method for achieving the training objective, which may include a didactic lecture, a flip class, or a simulation session. Jonathan intends to deliver a video didactic lecture to the transport team before they participate in a simulation session. Guided by HIE scenario objectives, Jonathan chose to run a computer-based simulation in a simulation centre. If there is difficulty having protected time for staff to attend the session, another alternative is to run it in situ; simulation that is physically integrated into the clinical environment provides a method to improve reliability and safety in high-risk areas.25
5. Implementation
Jonathan and the transport team educator take the following logistical measures in preparation for the HIE simulation session to ensure its success:
- make a reservation at the simulation centre
- send the finalised HIE scenario to the simulation technician
- assign a transport team member to the session and ensure that their time is protected
- send a calendar reminder to session participants
- arrange food and drinks.
On the day, Jonathan and the transport team educator arrive one hour before the session to make sure the equipment is available and to discuss the scenario flow with the simulation technologists. They allow 10 minutes for a pre-brief, information gathering and advice. A brief introduction to the simulation is necessary to ensure positive learning experiences. The pre-brief also sets up learners to the concept of simulation and familiarises them with the simulation environment. It allows for the establishment of perfor-mance and confidentiality expectations, and it is a crucial factor of a practical simulation experience. The instructor should also state the purpose of the simulation scenario up front: education versus assessment.
Simulation scenarios for education should be at a level of difficulty higher than the learner should be expected to handle well, in order to foster growth in the individual’s performance. Simulation scenarios designed for assessment should be at the expected level of performance for the person evaluated.
During the simulation pre-brief, participants will be given a case history. The scenario’s flow is based on the case vignette, and it starts with initial parameters (eg predetermined patient vital signs) that will change over time. The pace at which these parameters adjust should be as reasonable as possible, but there is flexibility in changing the rate of patient decline and titrating the degree of difficulty based on learner experience.
In these dimensions, scenario design usually includes expected activities and changes, as well as concrete responses to anticipated interventions. In scenario models, this can be interpreted as tables or flow diagrams. In this way, an unfolding plot can be plotted out. Many types of simulators may be used to pre-programme transitions and reactions to particular actions (eg apnoea following administration of surfactant). Staff must, however, remain vigilant during simulation delivery to ensure that simulator responses match participant behaviours, even when the unexpected occurs.26
At the end of the scenario, it is important to allow 20-30 minutes for debriefing during which the learners/teams reflect, revisit, and analyse the activity in order to improve individual and team clinical skills and judgement.6,27
6. Evaluation and feedback
Getting input from learners through a structured post-simulation session survey or focus group discussion will help you tailor the simulation programme to the learners’ future needs. Examples of debriefing and post-session evaluation tools include the DASH tool.28
Conclusion
Neonatal transport medicine is a unique and challenging specialty. Simulation provides an opportunity for transport team members to acquire and maintain skills specific to their role. Developing a simulation programme curriculum is complex and time and resource-intensive. There is no single way to develop a simulation programme curriculum, but having a structured approach will ensure the simulation programme's success.
Or read this article in our
Tablet/iPad edition
- Deliberate practice of a skill with constructive feedback is critical to building expertise and mastery.
- High-fidelity simulation for transport team training improves team members' confidence in clinical and communication abilities.
- Creating a simulation programme curriculum takes time and resources. An organised approach will ensure success.
Also published in Infant:
