

Necrotising enterocolitis in a preterm infant with late-onset group B streptococcus sepsis and meningitis
Here we report the case of a preterm infant born at 29+5 weeks’ gestation who presented at two weeks of age with symptoms of necrotising enterocolitis (NEC) and features of late-onset sepsis. NEC was diagnosed radiologically and group B streptococcus (GBS) was isolated in blood and cerebrospinal fluid cultures. The baby was treated medically for NEC, sepsis and meningitis and later suffered significant complications of meningitis with hydrocephalus. This case report describes the link between late-onset GBS sepsis and NEC.
Dyanne Imo-Ivoke
ST2 Paediatrics
Hull University Teaching Hospitals NHS Trust
Joanna M Preece
Consultant Neonatologist, Department of Neonatology, University Hospitals of Leicester
joannapreece@nhs.net
Background
Reports suggest a link between GBS sepsis and NEC in newborn infants.1,2 The gut microbiome changes with age; in the early neonatal period the gut is colonised by maternal flora and then common environmental commensal organisms. By two years of age, it is relatively the same as an adult’s gut. Abnormal or deficient gut colonisation has been implicated in NEC.3 Infective causes of NEC include bacteria such as E. coli, viruses and fungi but GBS is not a commonly recognised infective cause of NEC.4 Atypical presentations leave the question as to whether other microbes, particularly GBS, could trigger the cascade resulting in NEC. However, GBS as a bowel commensal in association with NEC may secondarily lead to blood sepsis, meningitis and the more typical picture of late-onset GBS sepsis.
The case report
Presentation
A preterm infant of 29+5 weeks’ gestation was born at home following spontaneous rupture of the membranes. The pregnancy was normal and there were no other risk factors for sepsis apart from prematurity.
Early problems included hypoxia, hypothermia and hypoglycaemia; respiratory, glycaemic, and thermoregulatory support commenced with good effect. Nutrition was maintained on day 0 with intravenous fluids. Enteral feeds commenced on day 1 of life and were established over the next few days. The baby passed meconium by day 3.
Routine screening for sepsis was undertaken upon admission to the neonatal unit and the baby was commenced on benzylpenicillin and gentamicin. C-reactive protein (CRP) levels were low and considered negative (two tests, at least 18 hours apart) as was a blood culture. Antibiotics were stopped once the blood culture result was available. Probiotic drops (Labinic) were started early and caffeine citrate was given to a gestational age of 34 weeks.
By day 5, 14.7% weight loss was noted despite regular nasogastric tube feeds of expressed breast milk (EBM). These were fortified with human breast milk fortifier and the volumes delivered were increased to encourage growth. There were a few episodes of vomiting with feeds, which resolved with medical management for reflux. All aspects of care were stable after the first week and the baby was well enough to be transferred to the special care baby unit to establish oral feeds. With declining maternal breast milk supply, donor EBM was initially used and then the feeds were transitioned to preterm formula over a two-week period.
On day 19 of life, the baby developed recurrent desaturation and pyrexia. Activity and alertness were much reduced. The baby developed a full, tense and tender abdomen with recurrent apnoeas needing mechanical ventilation. Mild septic shock developed with metabolic acidosis, managed with saline fluid bolus and bicarbonate. The baby had a fixed tender loop on clinical examination and a series of X-rays were performed over four days. A diagnosis of NEC was made based on the clinical signs in conjunction with radiological findings. In mild NEC, the X-ray may be normal or may show some intestinal dilatation and ileus. Findings on X-ray therefore contributed to the diagnostic picture when interpreted with the clinical signs.5 A conservative and supportive management strategy was followed.
Investigations
The infant had thrombocytopenia with a platelet count of 43x109/L. The initial CRP level taken at the time of deterioration was 28mg/L, peaking at 122mg/L 24 hours later. A blood culture taken during the acute deterioration was positive for Streptococcus agalactiae (group B streptococci).
A chest X-ray showed a right upper lobe collapse and there was a paucity of gas with spreading right pneumatosis on the abdominal X-ray (FIGURE 1). No bowel perforation occurred. The baby was stable enough for a lumbar puncture four days later, with an initial tap having a cloudy appearance. A PCR test (polymerase chain reaction) was positive for GBS. The cerebrospinal fluid (CSF) was blood-stained and, therefore, a cell count could not be performed.

FIGURE 1 Chest and abdominal X-rays taken on day 20 of life show possible intramural gas and dilated bowel loops. The right upper lobe consolidation was attributed to a mechanical issue with ventilation and resolved quickly.
Early management
The NEC was managed medically and did not require surgery. Following the acute deterioration, the baby was ventilated for respiratory support. A platelet transfusion was given, and milk feeds were withheld for 10 days with nasogastric tube drainage to decompress the bowel. The baby initially received triple antibiotics (teicoplanin, gentamicin and metronidazole) as per the local NEC management policy. After the isolation of the GBS on blood culture and following advice from the microbiologist, this was changed to meropenem and teicoplanin and continued for 10 days. A further four days of benzylpenicillin was given as part of the recommended 14 days of treatment for GBS meningitis.
Parenteral nutrition was maintained until feeds were re-established. There was adequate pain control with morphine. Antifungal prophylaxis was given in line with the guideline for late-onset sepsis in newborns.6
Late complications
A routine cranial ultrasound scan (CrUSS) was performed at 34+1 weeks corrected gestational age (CGA) and showed enlarged cerebral ventricles with ventricular indices on the 97th centile (FIGURE 2). Repeat CrUSS at 36+3 weeks CGA showed a significant increase of the ventricular index to 97th centile + 4mm. Occipitofrontal circumference (OFC) remained stable on the 9th to 25th centile. Neurological examination and behaviour remained normal for CGA. Referral to the neurosurgeon and magnetic resonance imaging (MRI) was arranged.
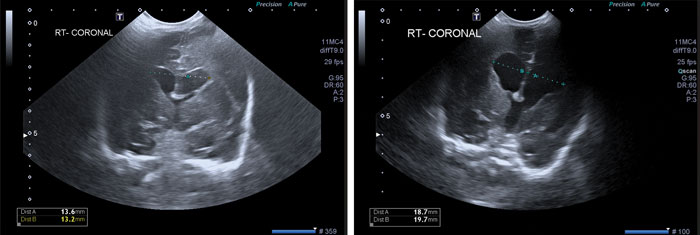
FIGURE 2 CrUSS at 34+1 weeks CGA (left) vs CrUSS at 36+3 weeks CGA (right) showing an increase in ventricular index (VI) from 13mm to 21mm over a two-week period. At 36+3 weeks the VI is already over the 97th centile for gestational age.7
At 36+4 weeks CGA, there was an acute deterioration with generalised seizure. The septic screen was repeated and benzylpenicillin and gentamicin were commenced. The seizure was brief and a single episode. Monitoring of cerebral function was normal. A brain MRI showed marked dilatation of the third and lateral ventricles and narrowing of the mid aspect of the cerebral aqueduct. There was no evidence of intraventricular haemorrhage or abnormality in the brainstem structures. There were no clinical features of active hydrocephalus.
A second lumbar puncture was performed before the antibiotics were commenced and the CSF analysis showed increased leukocytes (mainly polymorphs) with a ratio of 1:50 red blood cells to white blood cells. No organism was seen, and CSF, PCR, CRP and a blood culture were negative. IV benzylpenicillin and gentamicin were given for three weeks.
A further lumbar puncture was performed at 38+4 weeks CGA and showed persistent leukocytosis with a ratio of 1:295 red blood cells to white blood cells. CSF culture and gram stain were negative. During this treatment phase, the OFC progressively increased to the 75th to 91st centile, requiring a therapeutic lumbar puncture to drain the CSF. The CSF cell count ratio was 1:2 red blood cells to white blood cells with CSF culture and PCR remaining negative.
The baby was transferred to the nearby centre and a ventriculoperitoneal shunt was inserted at 39+6 weeks CGA by the tertiary neurosurgical team. Progress following this was smooth and the baby was successfully discharged home to receive neurodevelopmental and neurosurgical follow-up as an outpatient.
Discussion
This case describes NEC in a preterm infant with confirmed evidence of late-onset GBS sepsis complicated by meningitis and hydrocephalus.
GBS and sepsis in the newborn
GBS is a common commensal in the gut and vagina; about one in five pregnant women in the UK are colonised with GBS.8 It is implicated in early and late-onset neonatal sepsis. GBS sepsis is rare after three months of age.
GBS sepsis caused by S. agalactiae is an important cause of sepsis in newborns, with 1 in 1,750 babies born in the UK and Ireland each year developing GBS sepsis. While most babies will make a good recovery with prompt management, about one in 19 babies with GBS sepsis die, and one in 14 survivors will have lifelong physical or neurological sequelae.9
In early-onset GBS sepsis (occurring within 72 hours of birth), the presentation is usually respiratory distress; in late-onset GBS sepsis, meningitis is a common presentation. GBS is the most frequent pathogen in early-onset sepsis, accounting for up to 31% of cases. In late-onset sepsis, it accounts for about 9% of cases. While GBS commonly manifests as septicaemia, in <1% of cases it can manifest as focal infections.10
Meningitis is a known presentation of late-onset GBS sepsis. GBS and E. coli account for more than two-thirds of cases of meningitis in late-onset sepsis. In the UK, the case fatality associated with neonatal meningitis has declined from 25% to 10%, but the long-term sequelae remain unchanged.11,12 Preterm babies have a four-fold higher risk of GBS meningitis and a significantly higher case fatality ratio than term infants.
GBS sepsis and meningitis are a known association, and this can cause hydro-cephalus due to impedance of CSF flow and reduced reabsorption of CSF. Seizures, lethargy and low serum white cell count are common presentations of hydrocephalus after GBS meningitis, with up to 10% of these infants showing a non-communicating picture requiring a ventriculoperitoneal shunt.13-15 In one series, meningitis presented at the median age of 12 days of life, and hydrocephalus developed at the median age of five weeks after the diagnosis of meningitis.13 In our case, the age at presentation is within the median age. However, the complication of hydrocephalus developed earlier.
In children with GBS meningitis, it would be beneficial to anticipate this complication and have regular follow-ups commencing as soon as possible. Repeat lumbar puncture towards the end of and after treatment is essential to rule out partially treated meningitis.
Prematurity is a significant risk factor for late-onset sepsis, and the risk is inversely proportional to the gestational age.16 Babies born to mothers of black origin and babies of mothers with a positive GBS culture have a higher risk for early and late-onset sepsis.17 Late-onset GBS sepsis can occur following transmission of GBS through breast milk and nosocomial acquisition.18
NEC
NEC is a common cause of gastrointestinal emergencies in newborns, especially preterm infants. In the early phases, the signs are non-specific and can mimic many other conditions such as sepsis, feeding intolerance, gastro-oesophageal reflux and urinary tract infection. Blood investigations are non-specific. Persistent thrombocytopenia or neutropenia and metabolic acidosis can indicate very severe disease. Elevated levels of CRP may be a pointer to an underlying complication such as abscess or stricture. Diagnosis of NEC is confirmed radiologically on serial abdominal X-rays.
The exact pathophysiology of NEC remains poorly understood because it is multifactorial. Gut maturity and abnormal colonisation of the gut by microbes are some of the implicated factors. In our case, the initial presentation was not specific and, in the absence of any obvious foci, it was suggestive of late-onset neonatal sepsis. However, features in keeping with NEC developed rapidly. This is suggestive of a primary focus of NEC leading to a bloodstream infection. Metabolic acidosis and thrombocytopenia, though suggestive of severe NEC, are also seen in primary bloodstream infection, making the initial diagnosis of NEC difficult. A high level of CRP is not specific to NEC and can be caused by a host of other conditions. Conservative management for NEC is the recommendation for Bell stage II of NEC, and the baby was managed based on this.
GBS as a cause of NEC
GBS is not commonly implicated in NEC and is not universally accepted as a cause of NEC. There have been some instances of NEC with GBS positive culture. Gram-negative bacilli are the typically isolated organisms in culture-positive NEC.1,2
The concept of translocation of bacteria through the lumen wall is not new.19 Cases of early-onset GBS bloodstream infection in newborns with NEC have been reported and led to the suggestion that GBS be added as a potentially infectious agent associated with NEC.2 A mechanism of translocation through the injured intestinal mucosa was supported rather than bacteraemia being the initiating event for NEC. The link between NEC and late-onset GBS sepsis has also been described.20
Further small studies point to GBS presence in the neonatal gut causing bloodstream infection following trans-location and can be implicated in late-onset infection.21 Preterm infants do not have a normal gut microbiota. Multiple GBS strains may colonise for a prolonged period and are not easily cleared by parenteral antibiotics.
GBS sepsis with a proven focus of infection such as NEC or catheter-associated bloodstream infection is not rare. It is associated with significantly higher rates of infectious complications and severity of illness.22 In neonates presenting with features of sepsis, an effort should be made to identify the focus of infection. Complications such as septic shock, disseminated intravascular coagulopathy, thrombocytopenia, anaemia and metabolic acidosis are more likely to occur in these infants.
It has been suggested that there could be three different entities in the spectrum of GBS disease with NEC:23
- NEC-associated bloodstream infection
- primary bloodstream infection occurring under 72 hours
- post-NEC bloodstream infection more than 72 hours after the onset of NEC.
Other studies have proposed that the exact initiating step in the association between sepsis and NEC may, at best, be complementary rather than bloodstream infection arising directly from the loss of gut wall integrity or that the bloodstream infection predisposes to NEC by activating a proinflammatory response.24 This supports the theory that the presence of a bloodstream infection does not necessarily precede NEC, as widely thought.
There is a difficulty in monitoring for late-onset sepsis as symptoms are often non-specific, differences exist in agreed definitions in some countries, and pathogens are more varied than in early onset sepsis.25 In addition, blood cultures have low sensitivities partly due to the low volume of blood taken in neonates, which reduces the associated diagnostic accuracy of late-onset sepsis. The diagnostic dilemma with late-onset sepsis also applies to NEC as the initial symptoms are often non-specific and can be mild, leading to an underdiagnosis of the condition in preterm infants with late-onset sepsis.
In all cases, bacterial colonisation appears necessary for NEC-associated GBS sepsis, which may be in the form of colonisation from the mother, siblings, hospital staff or breast milk.
Conclusion
This case discussion seeks to emphasise that there is a need for further review of microbial causes of NEC as there is evidence of an association between GBS and NEC. There was an onset of features suggestive of NEC and X-ray findings within 24 hours of deterioration, indicating that translocation of GBS through the injured mucosa may have led to the sepsis and the complication of meningitis. Regular and prompt follow-up with CrUSS and serial OFC measurements allowed early assessment of the need for neurosurgical intervention and enhanced monitoring.
Bloodstream infection associated with NEC is likely to be underdiagnosed due to the small samples often achieved when taking neonatal blood cultures. There may be clinical signs of a focus in many cases of bloodstream infection in the newborn. In newborns presenting with clinical features of NEC, concurrent foci of infection should be actively ruled out.
Complications from GBS meningitis may manifest up to seven weeks post treatment. In a patient with GBS-associated meningitis, it is relevant to institute monitoring such as CrUSS and serial OFC measurements.
This case report describes the link between late-onset GBS sepsis and NEC. In preterm infants colonised with GBS and at risk of NEC, NEC may be the primary trigger of blood sepsis and associated severe complications such as meningitis. Conditions such as late-onset GBS sepsis and NEC have significant long-term consequences for preterm infants. The presence of additional complications, such as meningitis, should be actively sought and later complications, such as hydrocephalus, anticipated and monitored.
Parental consent
The authors obtained written consent from the child’s parents for publication of the case history and images.
Author contributions
D I-I: writing, literature review.
JP: conception, supervision and text editing.
Acknowledgements
The authors would like to extend special thanks to: Dr Hiba Ahmed and Dr Alyssa Loo for the images; Hull University Teaching Hospital NICU and Leeds General Infirmary Neurosurgical team for care of the baby; and Embrace, the transport service for critically ill infants and children in Yorkshire and the Humber.
Or read this article in our
Tablet/iPad edition
- NEC may be caused by GBS but NEC remains a poorly understood condition and no assumptions should be made regarding its causative factors.
- In preterm infants colonised with GBS and at risk of NEC, NEC may be the primary trigger of blood sepsis and associated severe complications such as meningitis.
- In a patient with GBS-associated meningitis, it is relevant to institute cranial monitoring.
Also published in Infant:
