

Coffee bean sign in a preterm neonate on an abdominal X-ray
A preterm male infant presented with abdominal distension and palpable bowel loops at 27 days of life. An abdominal X-ray showed a ‘coffee bean’ appearance of the bowel and raised the possibility of a sigmoid volvulus. Subsequent abdominal X-rays showed resolution of the coffee bean but the presence of intramural gas, and thus the infant was managed conservatively for necrotising enterocolitis. In this case a careful clinical evaluation with early imaging and multidisciplinary team discussion played an important role in ruling out sigmoid volvulus.
Vikranth Bapu Anna Venugopalan
Consultant Neonatologist
Ahmed Abdulaziz Omar Ahmed
Consultant Neonatologist
Francine Wootton
Advanced Neonatal Nurse Practitioner
Birmingham City Hospital, Sandwell and West Birmingham Hospitals NHS Trust
The Case
A 27-day-old male preterm neonate born at 32 weeks’ gestation presented with a markedly distended abdomen with dilated loops of bowel (while in the neonatal unit). He was on a mixture of the mother’s expressed breast milk with human milk fortifier and breast feeds.
He was born in good condition and had needed continuous positive airway pressure (CPAP) for four days. He was breathing well on his own and his feeds had been slowly increased to 180mL/kg/day.
At the time of the deterioration, when he presented with abdominal distension and palpable bowel loops, there was no respiratory distress. His haemodynamic status was stable with normal perfusion and capillary refill time of <2 seconds. There was no history of vomiting and the infant had opened his bowels with normal stools (ie not blood stained). He had normal blood gas parameters with normal lactate levels. He was screened for sepsis and started on antibiotics.
An abdominal X-ray (FIGURE 1) showed dilated loops of bowel in the left iliac fossa; notably a ‘coffee bean’ appearance of the bowel, and thus a possibility of a sigmoid volvulus could not be excluded.
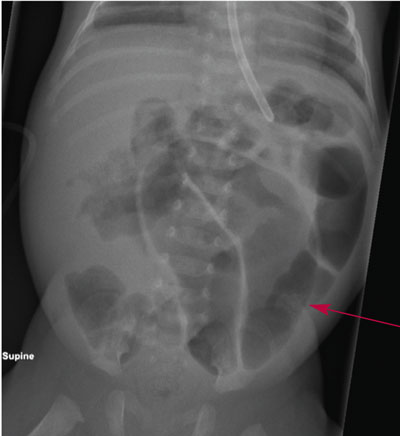
FIGURE 1 The coffee bean sign on an abdominal X-ray in a preterm neonate.
The child was stable from a respiratory and haemodynamic point of view and did not have a tense or tender abdomen. It was felt that this was unlikely to be a sigmoid volvulus and the paediatric surgeons at a tertiary hospital concurred with this. A subsequent abdominal X-ray (FIGURE 2), performed five hours after the initial X-ray showed resolution of the coffee bean appearance but there was evidence of intramural gas on the X-ray; therefore the infant was managed conservatively for necrotising enterocolitis (NEC) with seven days of nil-by-mouth and triple antibiotics (flucloxacillin, gentamicin and metronidazole).
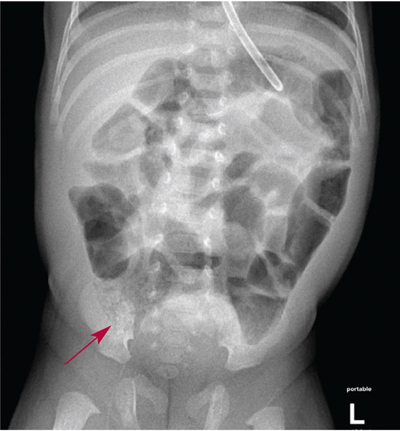
FIGURE 2 The abdominal X-ray repeated five hours later showing resolution of the coffee bean sign and presence of intramural gas
Following this, the infant was recommenced on enteral feeds, which were slowly increased to full feeds. He was discharged home nine days later and remained well.
Discussion
Sigmoid volvulus is the most common cause of volvulus in adults and the coffee bean sign is the classical radiological finding of a sigmoid volvulus, first desc-ribed in 1946.1-5 Sigmoid volvulus is an extremely rare cause of bowel obstruction in the newborn period.3,6-8 The first report of sigmoid volvulus in a 14-day-old boy was published in 1961,6 whereas the youngest patient reported is a one-day-old boy with anal stenosis.8 It can also be associated with Hirschsprung’s disease.9
In this neonate, although there was abdominal distension with the classical coffee bean sign on an abdominal X-ray, the baby was haemodynamically and clinically stable and this did not fit with a diagnosis of sigmoid volvulus. Subsequent sequential abdominal X-rays showed resolution of the coffee bean appearance but the presence of intramural gas. NEC is a gastrointestinal emergency with potentially devastating consequences and early diagnosis and treatment is extremely important. NEC is usually associated with tenderness and the presence of a tense abdomen, which was absent in our neonate, however, intramural gas in a neonate is considered indicative of NEC and therefore, the infant was managed conservatively for NEC.
The differential diagnoses for this case were:
- dysmotility of the gut due to prematurity, which was felt unlikely as the baby was fully fed and tolerating feeds prior to the deterioration
- meconium plug obstruction, which usually occurs in the first few days of life and was considered too late for this neonate.
Clinical examination findings and repeat X-rays guided further management and ruled out the possibility of a potentially serious surgical problem of sigmoid volvulous. Following discharge, he remained well.
This case highlights the importance of correlating clinical and radiological findings, and careful evaulation of a baby via clinical examination and repeat X-rays.
Or read this article in our
Tablet/iPad edition
- The ‘coffee bean sign’ is a classical radiological presentation of a sigmoid volvulus, however this did not fit with the clinical presentation and stability of the baby in this case.
- While the coffee bean sign might be a sign of sigmoid volvulus in older children and adults, X-ray appearances in preterm infants are often not ‘classic’ and may present unusual findings.
- This case highlights the importance of clinical and radiological correlation.
Also published in Infant:
