

Human milk oligosaccharides and necrotising enterocolitis
Human milk is known to reduce the risk of necrotising enterocolitis (NEC) in preterm infants, but mechanisms are poorly understood. Human milk oligosaccharides (HMOs) are complex sugars produced by the mammary gland and present in variable amounts in different breast milks. Animal models show HMOs impact on development of NEC and human
preterm infant studies show a specific HMO, called
disialyllacto-N-tetraose (DSLNT), is present in maternal milk in lower amounts in infants who go on to develop NEC. This article reviews the role of HMOs in NEC development and the clinical data in preterm infants, and considers the possible next steps for supplementation in preterm infants.
Kristina Chmelova1
Neonatal Research and Transport Fellow
k.chmelova@nhs.net
Andrea C Masi2
Clinical Researcher
Janet E Berrington1,2
Consultant Neonatologist
1Department of Neonatology, Newcastle upon Tyne Hospitals NHS Foundation Trust
2Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne
Importance of NEC
NEC remains a devastating condition in significantly preterm infants and a major cause of both mortality and morbidity.1 Data from the UK National Neonatal Audit Programme (NNAP) identified that in 2020, 6.5% of infants born at less than 32 weeks’ gestation experienced at least one episode of NEC, equating to 417 infants annually.2 The large UK trials SIFT (Speed of Increasing milk Feeds Trial)3 and ELFIN (Enteral Lactoferrin supplementation in Newborn very preterm infants)4 identified rates of NEC of 5.3% and 5.6%, respectively. Surgery is needed in between 10% and 50% of cases depending on the cohort, and up to 50% of cases will die.5
Neurodevelopmental outcome is worse after NEC than after meningitis or sepsis.6 Caring for an infant with NEC is costly in financial terms to the NHS and in financial, practical and emotional terms to families.7 Despite significant investment in NEC research, rates have not fallen and in some countries are rising as survival in the most extreme preterm infants improves. NEC pathogenesis is complex and incompletely understood, but is believed to occur when the complicated interactions between the immune system, gut microbiome and diet result in an inflammatory process within the bowel.
Modifiers of NEC incidence
NEC is reduced in preterm infants with optimal antenatal steroid use (relative risk, RR=0.5),8 optimal cord management (RR=0.91),9 and in those not receiving prolonged (odds ratio, OR=1.21)10 or no early antibiotics (OR=0.25).11 Meta-analysis of probiotic trials shows an almost halving of NEC incidence (RR=0.54)12 and BOOST (Benefits of Oxygen Saturation Targeting Trial) identified that higher saturation targeting reduced NEC (RR=1.22 for lower saturations).13,14 Milk feed type is also key to NEC prevention; infants receiving maternal milk have a significant risk reduction (RR=0.69)15 and donor milk appears preferable to formula (RR=1.87)16 (TABLE 1). The mechanisms through which human milk, and especially mother’s own milk (MOM), are protective are not well understood but there appears to be a dose dependent response.17,18 Individual breast milk components have been studied and supplemented in clinical trials in preterm infants, notably lactoferrin which was supplemented (in bovine form) in the recent large UK trial ELFIN4 but which did not change NEC rates. Similarly increasing feeds at 18 or 30mL/kg/day did not impact NEC rates, as shown by the SIFT study.3 Some treatments have been shown to be associated with increased NEC notably anti-reflux treatments,19 which are not now recommended in preterm infants.
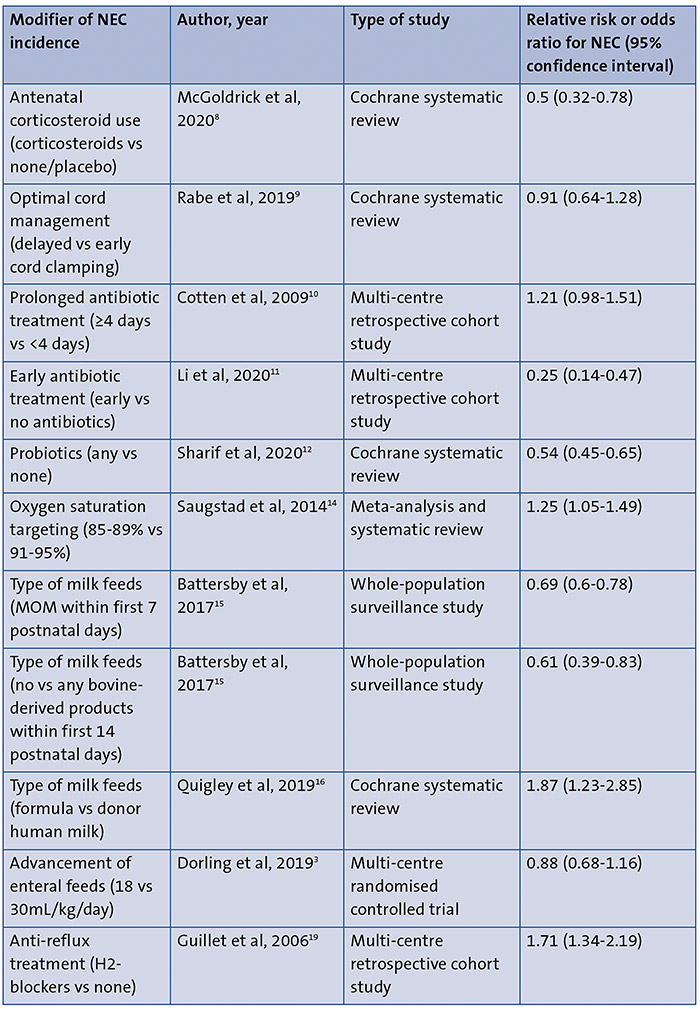
TABLE 1 Modifiers of NEC incidence. Key: NEC=necrotising enterocolitis; MOM=mother’s own milk.
Human milk oligosaccharides
HMOs are complex sugars found in breast milk and are the third most abundant solid constituent, at between 5 and 15g/L depending on lactation stage.20 They have multiple roles that may contribute to help prevent NEC. HMOs cannot be digested by humans as we lack the enzymes to do so, rather they are digested by the bacteria within the gut. They therefore act as a food substrate for bacteria that do have the enzymes to digest them, which in turn produce small molecules (metabolites) that impact on the host metabolism, or feed other bacteria. Certain bacteria are better able to use HMOs as food, including those traditionally considered ‘healthy’ gut bacteria, for example, bifidobacteria. Thus, HMOs act as ‘prebiotic’ promoting a healthy bifidobacterial rich gut microbiome. They can also act directly on the gut epithelial cells to promote development and maintain tight junctions between cells, modifying the ability of bacteria to translocate across the gut endothelium and promote an inflammatory response (FIGURE 1).
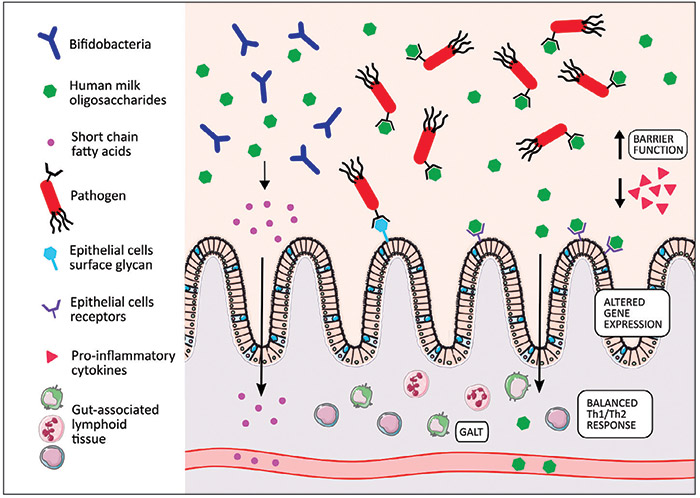
FIGURE 1 Mechanisms mediated by HMOs and influencing infant health (adapted from Masi et al31). HMOs serve as ‘food’ for potentially beneficial bacteria (eg bifidobacteria) and therefore promote their growth, which in turn protects an infant’s gut from pathogen colonisation. Metabolites produced from HMO digestion (eg short chain fatty acids) provide an energy source for colonocytes, increase mucin production and lower intestinal pH. HMOs act as anti-adhesive antimicrobials by coating pathogens and preventing their adhesion to epithelial surfaces. They can act directly on the gut epithelial cells to promote their maturation and maintain tight junctions between cells. This decreases the ability of bacteria to translocate across the gut endothelium. Interaction between epithelial cells and HMOs influences gene expression, which results in regulation of the inflammatory response (via cytokines, cell surface receptors, etc). HMOs can interact with the immune system by influencing lymphocyte maturation (Th1/Th2 response) and modulating leukocyte adhesion to endothelial cells.
HMO structure
HMOs are built from the monosaccharides:
- glucose
- galactose
- N-acetylglucosamine
- fucose
- sialic acid (N-acetylneuraminic acid).
These combine to provide a backbone of disaccharides:
- lactose, which forms the reducing end of the structure
- lacto-N-biose
- N-acetyllactosamine, which can elongate the backbone structure.
Additional modifications to the structure include: branching, with addition of the disaccharide through β1-6 linkage; addition of fucose (fucosilation) or addition of sialic acid (sialylation). These processes are determined by the genetic ability of the woman to produce two fucosyltransferases, which is in turn determined by her secretor status and Lewis positive status. Women with the secretor gene produce more 2-fucosylated HMOs and those with the Lewis gene, more 3-fucosylated HMOs. Some women carry neither gene and will produce very low, but detectable, levels of both. The combinations of sugars allow more than 150 different HMOs to be made, and profiles vary woman to woman (FIGURE 2).
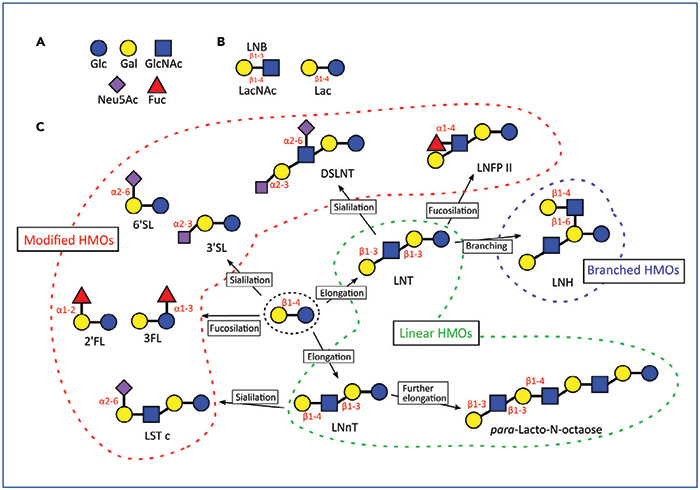
FIGURE 2 HMO structures. (A) Monosaccharides, (B) Disaccharides, (C) Examples of type of linkages and modification characterising HMOs. Key: Glc=glucose; Gal=galactose; GlcNAc=N-acetylglucosamine; Neu5Ac=N-acetylneuraminic acid; Fuc=fucose; LNB=lacto-N-biose; LacNAc=N-acetyllactosamine; Lac=lactose; HMOs=human milk oligosaccharides; 2′FL=2′-fucosyllactose; 3FL=3-fucosyllactose; LNnT=lacto-N-neotetraose; 3′SL=3′-sialyllactose; 6′SL=6′-sialyllactose; LNT=lacto-N-tetraose; LNFP II=lacto-N-fucopentaose II; LST c=sialyl-LNT c; LNH=lacto-N-hexaose; DSLNT=disialyllacto-N-tetraose. Adapted from Masi et al.31
Animal data
In rat pups gavaged with formula, with and without supplemental HMO, and then exposed to NEC-inducing hypoxia, one specific HMO called disialyllacto-N-tetraose (DSLNT) resulted in improved pathology scores in the intestine of the rats.21
Human observational data
In human preterm infants, observational data suggest that the same HMO, DSLNT, may play a role in NEC prevention. Breast milk received by 200 infants who remained healthy and eight who developed NEC had total HMO profiling and measurement of DSLNT levels. Although total HMO quantities did not differ, levels of DSLNT were significantly lower in the infants with Bell’s stage II or III NEC compared to healthy infants or those with stage I NEC.22 This was replicated in a larger cohort of 33 preterm infants with NEC and 37 gestational and age matched controls, with breast milk samples taken from feeds just before development of NEC. Again, no difference in total HMOs was seen, but DSLNT was significantly lower in infants with both medical and surgical NEC.23 A threshold level of 241nmol/mL was suggested as protective against NEC. This study was also able to explore the microbiome in association with DSLNT levels, and demonstrated an association between the pattern of gut bacteria, described as the preterm gut community type (PGCT) and the levels of DSLNT above or below the threshold proposed. Infants with DSLNT levels above the threshold were more likely to progress to a mature PGCT over time than those with DSLNT levels below the threshold. More mature PGCTs were associated with more beneficial bacteria, such as bifidobacteria.23
Human clinical trial data
To date, all clinical human trial data are from term infants where HMOs are added to formula. In 2015, a formula supplemented with 2′-fucosyllactose (2′FL) was given to healthy term infants and their growth compared to infants receiving formula without the HMO supplementation; no differences were observed. As the first human trial, there were no adverse effects noted.24 The infants also had their serum levels of inflammatory cytokines measured and had levels more comparable to breastfed infants than standard formula fed infants.25 Supplementation of term infants with two HMOs (2′FL and lacto-N-neotetraose, LNnT) was also well tolerated and did not affect growth.26 There was also some analysis of the stool microbiome in this study and the authors saw a shift in the bacterial patterns that more closely resembled breastfed infants than unsupplemented formula fed infants.27 Five different HMOs have also been studied in a formula, this time including 3-fucosylated HMOs as well as 2′FL and LNnT. Growth patterns and tolerability were similar compared to standard formula in term infants.28
Potential preterm clinical trials
There are currently no data relating to the deliberate supplementation of preterm infants’ diet with HMOs, but synthesis of specific HMOs is possible, opening up the possibility that clinical trials could commence. Given the complexities of the pathogenesis of NEC, the lack of availability of large quantities of HMOs and the associated costs, it is not currently likely that a large-scale supplementation of HMOs, akin to the ELFIN study, is feasible.
Given the demonstration of impact on gut microbiome, through which benefit may be being modulated, smaller scale feasibility studies are possible, which could also include measures of the gut microbiome/metabolome and infant inflammatory status. Such studies would need to begin by establishing safety and tolerability and dosing aspects, with the final aim being to supplement at levels above the threshold value identified by Masi et al23 for clinical benefit (TABLE 2). Such studies have been undertaken successfully, even on large scales, such as in the mechanistic study MAGPIE (Mechanisms Affecting the Gut of Preterm Infants in Enteral feeding studies), which sampled stool and urine in infants recruited to the ELFIN study across 13 units, and performed microbiomic and metabolomic assessments.29
Supplementation possibilities
Preterm infants could potentially be supplemented with HMOs by several routes. It is theoretically possible, but costly, to quantify the HMO profile and DSLNT levels in individual milk samples, as was carried out by Autran22 and Masi.23 This would theoretically allow milk banks to select milk with the highest levels of DSLNT to give preferentially to the infants most at risk of NEC. However, given the importance of the relationship between the HMOs and the gut microbiome, it is unknown whether supplementation via another woman’s milk, in the absence of a maternally transferred microbiome, would result in the same beneficial effects.
An alternative approach would be to synthesise specific HMOs and offer these as a supplement to infants, which could be given regardless of the type of milk the infant was on. Ideally this would be in powder form, since displacement of volumes of MOM is a theoretical disadvantage. Synthesis of HMOs is possible, and is currently undertaken, but some, including DSLNT are difficult to produce, and only small quantities are available. Current quantities would not allow for widespread supplementation, even if restricted to extremely preterm infants (TABLE 2).30
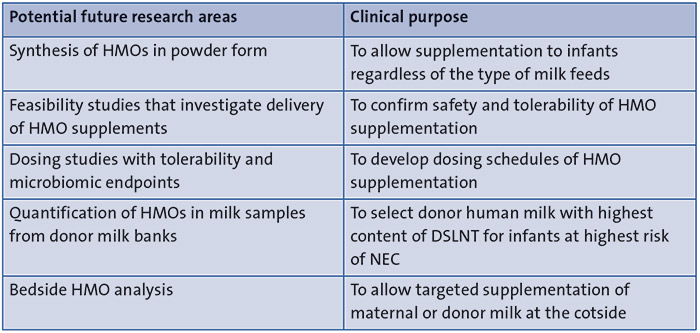
TABLE 2 Potential areas for further studies.
Summary
NEC is a serious disease with a high mortality and morbidity rate in preterm infants. Several factors modifying incidence of NEC are identified, among which maternal breast milk has significant role. HMOs are complex sugars found in breast milk that might play an important role in NEC prevention, through modulation of the gut bacteria or direct effect on the gut cells (FIGURE 3). Great variability in HMO profiles relates to structure modifications; these are genetically determined by the individual abilities of women to produce fucosyltransferases. DSLNT is an HMO that has been observed in higher levels in the breast milk of infants who do not develop NEC and additionally is associated with more mature community structures of gut bacteria. Clinical trials in term infants show that HMO supplementation is safe, well tolerated and linked to a shift in gut bacteria patterns. Supplementing preterm infants is theoretically possible. The impact of HMOs on gut microbiome, supplementation and synthesis possibilities are potential areas for future research.
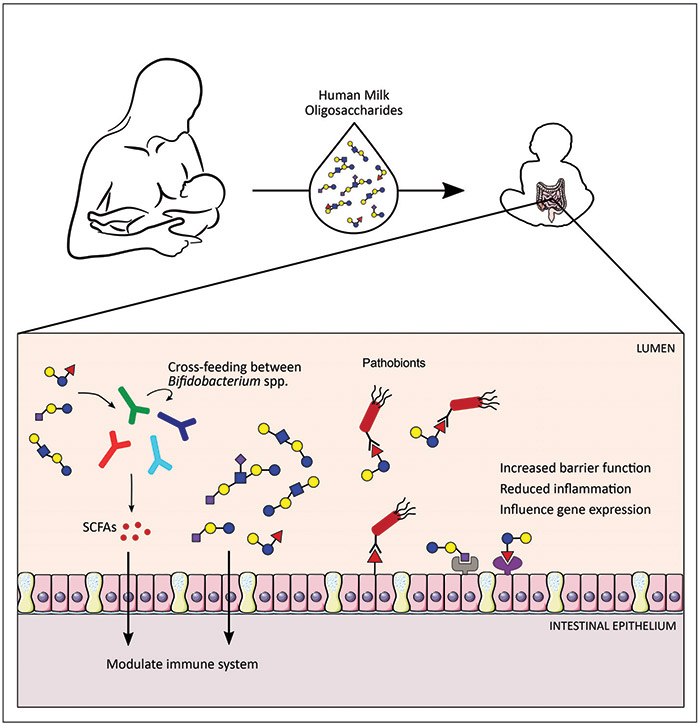
FIGURE 3 HMOs play a key role in modulation of the infant’s intestinal epithelium, immune system and gut microbiome. Key: SCFAs=short chain fatty acids. Adapted from Masi et al.31
Contributions
JEB had original idea for the article. JEB and KC co-wrote the manuscript. ACM provided figures related to HMOs. All authors contributed to manuscript alterations and approved final submission. JEB guided and supervised the writing process.
Acknowledgement
The authors gratefully acknowledge the work of the Newcastle Neonatal Nutrition and NEC Research Group (N4).
Or read this article in our
Tablet/iPad edition
- Although NEC is a major cause of mortality and morbidity in preterm infants, its pathogenesis remains unclear.
- HMOs are complex sugars in breast milk that cannot be digested by humans. Their composition varies widely from woman to woman.
- DSLNT is one HMO that may protect against NEC.
- Supplementation and synthesis of HMOs are subjects for future research.
Also published in Infant:
