

Investigating heart murmurs in neonates and children: reinvigorating the art of clinical medicine
Heart murmurs are common in neonates and children; however, it is important to differentiate between an innocent murmur and a pathological murmur. Heart murmurs can arise from abnormalities of the cardiac valves and other cardiac structures resulting in abnormal, turbulent blood flow that causes an audible extra sound. Nowadays, clinicians rely more on an echocardiogram than on their clinical skills, yet careful auscultation of heart murmurs can characterise the nature of a murmur and aid the diagnosis of many cardiac conditions. This article reviews the role of heart murmurs in congenital heart disease, and how to evaluate and characterise heart murmurs. A comparison of pathological heart murmurs is provided along with a description of investigations and suggestions for when to refer heart murmurs for detailed cardiac assessment, which includes an echocardiogram.
Vikranth Bapu Anna Venugopalan
Consultant Neonatologist with expertise in Paediatric Cardiology
Birmingham City Hospital, Sandwell and West Birmingham Hospitals NHS Trust
vikranth.venugopalan@nhs.net
Heart murmurs are very common in neonates and children but the presence of a murmur does not always mean the presence of congenital heart disease (CHD). ‘Innocent’ murmurs require no follow-up or treatment and, therefore, it is important to delineate them from pathological murmurs.1
Prior to the invention of the stethoscope by René Théophile Hyacinthe Laënnec in 1816, clinical examination of the heart was possible only by placement of the ears to the chest. Since then, there have been vast technological advances in the design and structure of stethoscopes alongside the evolution of many other modalities of cardiovascular investigations, including: chest X-rays; electrocardiogram (ECG); echocardiogram; pulse oximetry and more recently fingertip pulse oximeters; and cardiac magnetic resonance imaging (MRI).
Despite all of these technological advances, clinical examination of heart murmurs is still paramount and an important tool for making decisions as to when these technologies should be employed.
Antenatal screening
CHD is the most common congenital anomaly with an incidence of around 6-8 per 1,000 live births.2 The incidence of critical CHD is around 1-2 per 1,000 live births.3
Prenatal detection of CHD may improve the outcome of fetuses with particular types of cardiac lesions but not all heart conditions can be seen before the baby is born. The average antenatal pick-up rate of CHD in the UK is around 50% (2018-19 data)4 and prenatal detection rates vary widely. All pregnant women in the UK are offered a detailed anomaly ultrasound scan with cardiac review5 at around 20 weeks of pregnancy, however, structural cardiac anomalies are frequently missed by prenatal ultrasonography. A detailed fetal echocardiography scan should be performed if any abnormality of the heart is suspected on anomaly ultrasound or in the presence of recognised maternal risk factors (eg family history, pre-existing metabolic disease, maternal infection, teratogen exposure, maternal antibodies).6
Clinical features of CHD
Signs of CHD in babies can include: abnormal heart sounds (heart murmur or otherwise); cyanosis; weak or absent femoral pulses.
Symptoms and signs of heart failure can include: tachypnoea; flaring nostrils; chest recessions; tachycardia; tiredness and rapid breathing when the baby is feeding. Breathlessness can lead to poor feeding and poor weight gain. Signs of heart failure include hepatomegaly. Be aware of differential diagnoses due to respiratory causes or infection.
Evaluation of heart murmurs
History taking
A clinical evaluation of heart murmur begins with an assessment of the perinatal history, the family history of congenital heart disease and the mother’s clinical history. Some maternal risk factors for CHD include insulin-dependent diabetes, lupus, connective tissue disorders, rubella infection, phenylketonuria, excessive alcohol use during pregnancy and the use of antiepileptic medications. Chromosome abnormalities and genetic conditions may cause CHD. Always look for dysmorphic features – Down’s syndrome is the commonest genetic condition associated with CHD, most commonly an atrioventricular septal defect (AVSD).
Femoral pulses
Examination of the femoral pulses is a vital part of a cardiovascular examination. An absent/weak femoral pulse is a highly sensitive clinical sign and very likely to be coarctation of aorta. It may sometimes be difficult to feel the femoral pulses with gloved hands and it is worthwhile removing the gloves. Femoral pulses may also be difficult to feel if the baby/child is crying and unsettled and if they have a higher than normal muscle mass/adipose tissue. It is worth taking the time to keep the baby/child settled and feel the femoral pulses. It is also useful to measure the upper limb blood pressure as it can be associated with hypertension with coarctation of the aorta.
Localisation of the cardiac apex
The location of the cardiac apex is usually felt on the left side of the chest and if felt on the right side suggests dextrocardia or dextroposition (heart pushed to the right due to thoracic factors).
Characterising a heart murmur
A heart murmur needs to be characterised in detail regarding:
- timing of the murmur – systolic, diastolic, or both, or continuous
- grading of the murmur
- localisation and radiation of the murmur.
Timing of the murmur in the cardiac cycle
Heart murmurs are additional sounds heard between the normal heart sounds. In layman’s terms, a ‘whooshy’ noise heard between the two normal heart sounds. When listening to the heart, normally we hear the first and second heart sounds. The first heart sound (S1) is due to closing of the atrioventricular valves (AV valves). The second heart sound (S2) is due to the closure of the outflow tract valves (the semilunar valves; the pulmonary and aortic valves). S2 is usually split into two because the aortic valve (A2) closes before the pulmonary valve (P2).
A murmur heard between the first and the second heart sound is a systolic murmur (occurs during systole). A murmur heard between the second heart sound and the onset of the first heart sound is a diastolic murmur. If the murmur starts from the first heart sound and is heard throughout systole and diastole, it is known as a continuous murmur.
Systolic murmurs can be ejection systolic murmurs (ESM) or pansystolic murmurs (PSM, also known as holosystolic). In ESMs, the intensity of the murmur increases and then decreases (crescendo-decrescendo). ESMs are commonly innocent murmurs although other causes can include aortic and pulmonary stenosis.
PSMs are usually harsh sounds immediately after the onset of S1, extending to just before S2. PSMs include the murmurs of mitral regurgitation, tricuspid regurgitation and ventricular septal defects.
Diastolic murmurs are usually abnormal and may be early, mid or late in diastole. Diastolic murmurs are rare in neonates.
Grading of the murmur
Systolic murmurs are graded on a six-point scale.
Grade 1: barely audible
Grade 2: soft but easily audible
Grade 3: moderately loud, no thrill (vibration)
Grade 4: louder, with palpable thrill
Grade 5: audible with the stethoscope barely on the chest
Grade 6: audible with the stethoscope off the chest.
Localisation of the murmur
The anatomic location of the murmur is crucial in determining aetiology and any differential diagnoses of the murmur. Localisation refers to the place of maximum intensity of the murmur on the chest. It is extremely important to use the correct size of stethoscope when localising a murmur on a newborn or preterm infant (FIGURE 1).

FIGURE 1 Three different stethoscopes for size comparison. The adult stethoscope is shown on the left (blue rim). The central black rimmed stethoscope is for children and term infants. The preterm stethoscope (white rim) is much smaller and will permit more accurate localisation of murmurs.
Localisation is mainly based on valvar areas (FIGURE 2), such as the apical area for the mitral valve, the left upper sternal edge (LUSE) for the pulmonary valve, the right upper sternal edge (RUSE) for the aortic valve and the right lower sternal edge (RLSE) for the tricuspid valve. Murmur in the left lower sternal edge (LLSE) is suggestive of ventricular septal defect.
It is also important to listen to the back (the interscapular area); a murmur heard in this area can be due to coarctation of the aorta in infants/older children.
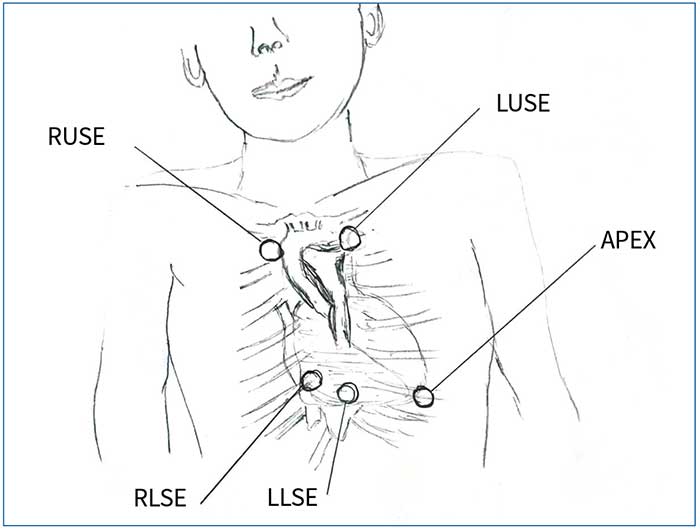
FIGURE 2 Localisation of murmurs based on valvar areas. Key: LUSE=left upper sternal edge (for the pulmonary valve); RUSE=right upper sternal edge (aortic valve); RLSE=right lower sternal edge (tricuspid area); LLSE=left lower sternal edge
Abnormal heart sounds
There are certain conditions where the heart sounds are abnormal. For example:
- a single S2 sound can be due to a transposed aorta or a single outflow tract
- a widely split S2 can be a feature of atrial septal defect or total anomalous pulmonary venous return (TAPVR)
- a loud P2 can be due to pulmonary hypertension and persistent pulmonary hypertension of the newborn (PPHN)
- muffled heart sounds are a feature of pericardial effusion/tamponade
- ejection ‘clicks’ heard in the LUSE can be caused by valvar pulmonary stenosis or in the RUSE by valvar aortic stenosis
- multiple ‘clicks’ can be heard with atrioventricular valve abnormalities and also in truncus arteriosus.
Innocent heart murmurs
Children with innocent heart murmurs7 have a normal cardiac examination, normal heart sounds and no other associated symptoms. Innocent heart murmurs include:
- systolic murmurs - Still’s murmur,8 pulmonary flow murmur, neonatal branch pulmonary artery stenosis
- continuous murmurs - venous hum.
Still’s murmur8 has a distinct vibratory/twanging/musical/buzzing quality with usually a grade 1-2 murmur, best heard between the apex and LLSE. Classical Still’s murmur is heard commonly in younger children. The murmur intensifies during fever, excitement and exercise and can have postural variation.
A pulmonary flow murmur occurs in asymptomatic children. A grade 1-2 mid-systolic murmur in the LUSE, which increases in intensity with exercise, fever or excitement. Other conditions such as anaemia and hyperthyroidism can have the same flow murmur. The differential diagnoses are due to pulmonary stenosis or an atrial septal defect.
Neonatal branch pulmonary artery stenosis murmur is more common in preterm infants, usually a grade 1-2 ESM in the LUSE. The murmur conducts to the axillae and/or back with normal femoral pulses. This is considered a physiological finding in neonates and usually resolves by six months of age.
Venous hum is typically heard in well children. A continuous murmur with maximum intensity in the supraclavicular fossa lateral to the sternocleidomastoid. The murmur varies with posture and disappears completely in supine position/occlusion of the jugular vein.
Pathological heart murmurs
Occasionally a heart murmur can be linked to a structural problem with the heart and/or the way that blood flows through the heart. A heart murmur is likely to be pathological if there are associated features suggestive of heart failure (poor feeding, cyanosis, signs of increased work of breathing, poor weight gain, etc) or if it is associated with dysmorphic features and in certain genetic/syndromic conditions such as Down’s syndrome, Noonan syndrome, DiGeorge syndrome, Williams syndrome, etc. TABLE 1 shows some common types of pathological murmurs and their associated pathologies.
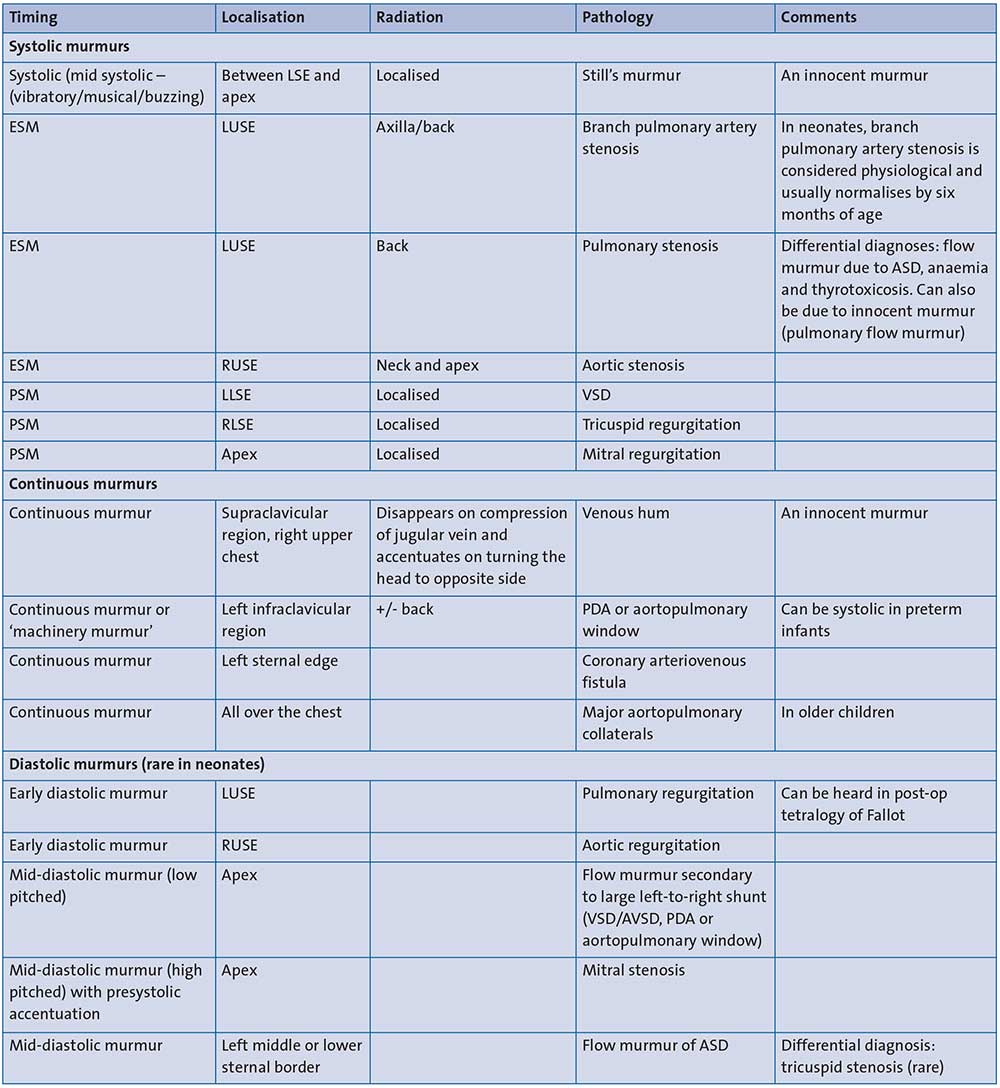
TABLE 1 Types of murmurs and possible pathologies. Key: ESM=ejection systolic murmur; PSM=pansystolic (holosystolic) murmur; LSE= lower sternal edge; LUSE=left upper sternal edge; RUSE=right upper sternal edge; RLSE=right lower sternal edge; LLSE=left lower sternal edge; AVSD=atrioventricular septal defect; PDA=patent ductus arteriosus; ASD=atrial septal defect; VSD=ventricular septal defect.
Patent ductus arteriosus (PDA) presents with continuous murmur, classically referred to as ‘machinery murmur’. In neonates with high pulmonary vascular resistance, murmur is usually a systolic murmur and best heard in the left infraclavicular region. Femoral pulses will be bounding in nature and can have a wide pulse pressure.
Ventricular septal defects (VSD) present with a PSM, best heard in the LLSE, that does not radiate. The smaller the VSD, the louder the murmur. Large VSDs can present with congestive cardiac failure due to left-to-right shunt and increased blood flow to the lungs, which happens once the pulmonary vascular resistance lowers (usually presenting at around 3-4 weeks of age, sometimes earlier).
Tricuspid regurgitation causes a PSM commonly heard in babies who are a few hours of age. These murmurs are best heard in the RLSE with normal femoral pulses. They may have differential saturations (pre-ductal > post-ductal with a difference >5%) with tachypnoea, recessions and features that lead to delayed adaptation of the neonate to extrauterine life. This murmur may be present in neonates with tricuspid regurgitation in PPHN.
Pulmonary stenosis can cause an ESM, usually > grade 2. The murmur can be heard in the LUSE and is conducted to the back. The femoral pulses are normal.
Some of these cases are associated with dysmorphic features and syndromes such as Noonan syndrome.
In aortic stenosis the murmur is of an ESM type, usually > grade 2, that is conducted to the carotids and to the apex. The femoral pulses are usually normal but with severe aortic stenosis, the femoral pulses and other peripheral pulses can be weak.
Investigations for heart murmur
Pulse oximetry
Pulse oximetry is routinely used as a screening tool for critical CHD in many hospitals in the UK; it is useful for detecting cyanosis. Based on the evidence available, both structured clinical examination (including determining presence and quality of bilateral femoral pulses) and universal use of pulse oximetry are most important in identifying CHD in asymptomatic term neonates with cardiac murmur before discharge home.9
Four limb blood pressure
Simultaneous blood pressure assessment in the four limbs of babies has poor sensiti-vity and several caveats (eg size of the cuff used, crying babies, use of oscillometry). A report by Crossland et al,10 found high false positive results of 8% (300 urgent cardiac opinions for every true diagnosis).
ECG
ECG on its own as a screening tool for murmur has poor sensitivity (40%), however, it has been shown to be a sensitive and specific screening tool for diagnosing AVSD.11 It is not useful as a screening tool in the diagnosis of other structural CHDs.12
A normal neonatal ECG shows right axis deviation because of the right ventricular dominance of the newborn heart. Left axis deviation in a newborn is a significant abnormal finding and should prompt further investigation. While an abnormal ECG should prompt further investigation, a normal ECG should not be considered reassuring if there are abnormal clinical findings or lower limb saturations of <95%.
Chest X-ray
Chest X-ray is not routinely required to diagnose CHD in neonates with murmur, but it does help to rule out respiratory or infectious causes. There are sometimes changes on a chest X-ray that might suggest specific conditions, for example:
- ‘snowman’ appearance in TAPVR
- ‘egg on its side’ appearance in transposition of the great arteries
- cardiac apex on the right in dextrocardia
- ‘boot shaped heart’ in tetralogy of Fallot/double outlet right ventricle.
Echocardiogram
An echocardiogram performed by trained personnel is the gold standard for a definitive diagnosis. The timing of the echocardiogram is best guided by the detailed cardiac examination and evaluation of the heart murmur.
Cardiac murmurs in neonates
The prevalence of cardiac murmur in neonates varies widely, from as low as 0.6% up to 77.4%.11, 13-16 Early reports (as far back as 1940) by Lyon et al17 highlighted how the detection of the murmur depends on the examiner.
In 1997, Arlettaz et al18 carried out a controlled echocardiographic study over a five-month period to analyse the natural history of innocent murmurs in newborn babies. Prevalence of murmur was noted to be 21 per 1,000 live births. Branch pulmonary artery stenosis was the commonest type; all resolved by six months of age. All babies with a small PDA were closed by six weeks. The majority of babies who had a small patent foramen ovale closed by six months.
A study by Farrer et al19 reported that with appropriate guidelines, senior house officers can make accurate assessment in 87% of cases with 71% sensitivity and 91% specificity. Karatza et al20 showed good correlation between paediatric trainees and neonatologists in accuracy of cardiac auscultation in asymptomatic neonates with heart murmurs. The aim of this study was to assess whether cardiac auscultation performed by paediatric trainees and neonatologists could reliably distinguish innocent from pathologic heart murmurs in asymptomatic neonates. The paediatric trainees had good ability in excluding CHD.
In a study by Mackie et al,21 201 neonates underwent clinical evaluation of murmurs, which were classified as ‘likely innocent’ or ‘likely pathologic’. CHD was confirmed by echocardiography in 113 out of 201 cases; a high prevalence. Features predictive of CHD were murmur quality, location and timing. The addition of an ECG did not improve these test characteristics.
Pathological murmur: when should you refer?
Many normal children have heart murmurs, but most children do not have heart disease; so when do you refer for a detailed cardiac assessment?22 The detailed clinical examination can reduce the number of unnecessary referrals for innocent murmurs and ensure that pathological murmurs can be referred for a thorough cardiac assessment at the appropriate time – either routinely, sooner or with urgency.
National guidelines developed by the PECSIG (Paediatricians with Expertise in Cardiology Special Interest Group, www.pecsig.co.uk) suggest the use of a traffic light system based on clinical examination findings (FIGURE 3). This system should help to delineate whether the murmur is innocent or pathological and this will inform a clinical judgement about referral for detailed cardiac assessment, corroborated by an echo-cardiogram to confirm the clinical diagnosis.
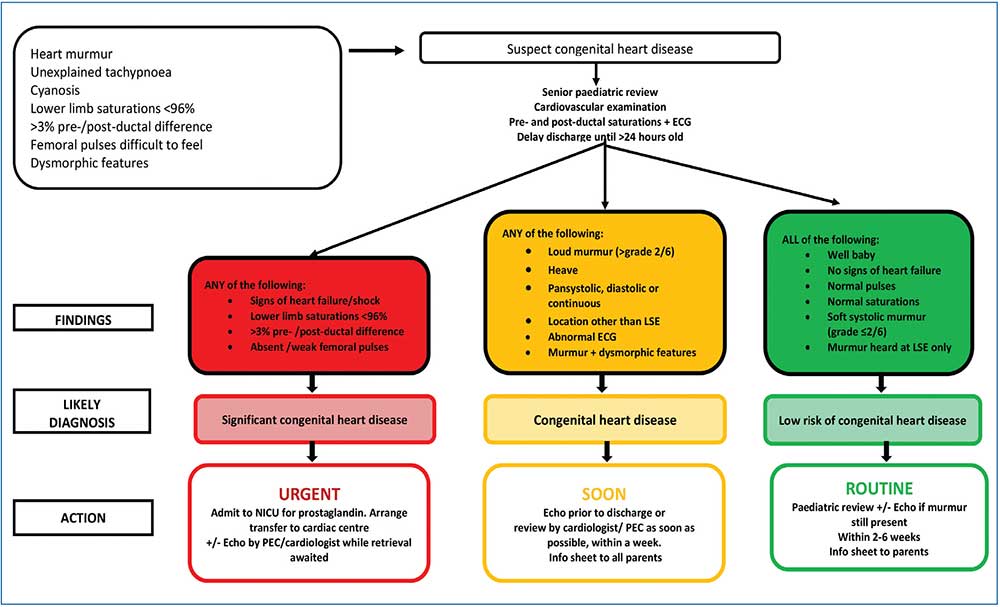
FIGURE 3 An adaptation of the PECSIG guidelines on cardiac murmurs in neonates and children. Key: NICU=neonatal intensive care unit; PEC=paediatrician with expertise in paediatric cardiology; LSE=lower sternal edge.
Conclusion
Many neonates and children have heart murmurs. A detailed clinical examination and relevant initial investigations can reduce the number of unnecessary urgent referrals for innocent murmurs and ensure that pathological murmurs can be referred for a detailed cardiac assessment (including an echocardiogram for a definitive diagnosis) at the appropriate time (routinely, sooner, with urgency).
Or read this article in our
Tablet/iPad edition
- It is important to distinguish a pathological heart murmur from an innocent murmur.
- A thorough clinical examination can identify those patients with pathological murmurs that might benefit from cardiology referral for an expedited detailed cardiac assessment, which includes an echocardiogram.
Also published in Infant:
