

Neonatal staff virtual debriefs: tips and pitfalls
This article describes our experiences of running a three-month pilot programme of psychology-led virtual and hybrid debriefs (including virtual and face-to-face participants) on our tertiary neonatal unit. Challenges, successes and participant feedback are summarised. We make practical recommendations on how to successfully implement psychology-led staff debriefs using a virtual platform, and propose virtual and hybrid debriefs as potential alternatives to face-to-face neonatal unit staff debriefing.
Sarah Chan
Locum Neonatal Consultant
sarah.walton@nhs.net
Sarah-Jane Archibald
Clinical Psychologist
Cambridge University Hospitals NHS Foundation Trust
Background
Debrief is a facilitated reflection of experiential learning.1 National guidance recommends debrief is offered to neonatal staff following difficult clinical situations, for example, serious incidents or neonatal death.2,3 These debriefs should allow discussion of staff emotional response.3 Literature evidence shows lack of time for discussion of difficult cases causes distress in neonatal clinicians4 and debrief reduces burnout risk in intensive care clinicians.5 Meta-analysis suggests increased effectiveness in teams who participate in debrief.6,7
Our neonatal intensive care unit (NICU) has a strong history of providing psychology-led staff debriefs,8 however, the COVID pandemic halted face-to-face sessions and there is a lack of guidance on how to run debrief sessions online. We piloted a virtual platform to continue delivery of NICU staff psychology-led debriefs in a COVID-safe way. We gathered staff feedback, adding novel findings to the scant literature evidence on NICU staff virtual debriefs.
Our virtual debrief model
Between April and July 2021, we ran 12 debriefs with 30 staff attendees over the three-month pilot. Eight sessions ran purely virtually and, as COVID restrictions eased, four sessions ran with a mixture of face-to-face and virtual attendees (hybrid sessions). Attendees included:
- 16 neonatal medical staff
- 7 neonatal nurses
- 7 allied health professionals, including midwives, obstetric theatre staff, paediatric anaesthetics and chaplaincy.
We use the following model for our debrief programme:
Posters advertising/explaining the virtual debrief session’s aims are placed in communal staff areas (FIGURE 1) and staff are invited to email cases requiring debrief.
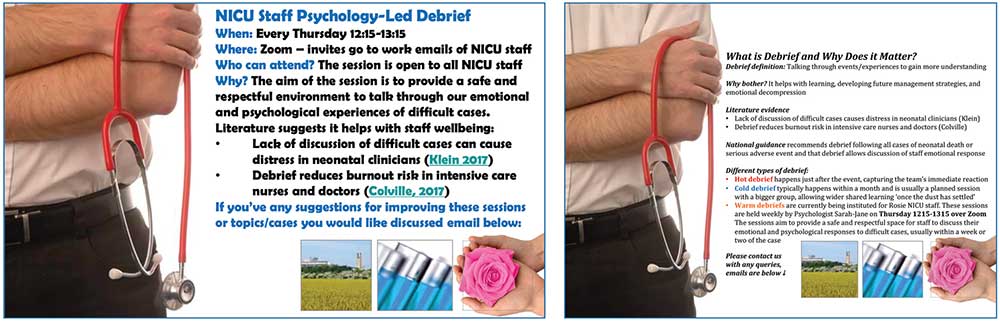
FIGURE 1 The virtual debrief posters encouraging staff to participate.
Each debrief session focuses on a particular case with the majority focusing on cases of neonatal death.
Zoom invitations are emailed to all NICU clinical staff and focused emails are sent to staff directly involved in the case.
Regular, hour-long, lunchtime debrief sessions are offered weekly within one to two weeks of the clinical case.
Our NICU’s clinical psychologist chairs the meeting, the neonatal consultant cofacilitates, and our assistant psychologist monitors the Zoom chat.
An adaptation of Archibald and O’Curry’s prebrief/debrief model is employed:8
- Ground rules are set, for example: ‘This is a safe space for us to consider the emotional and psychological impact of clinical cases on us as individuals and as a team. It is not the forum for us to review clinical management of the case. Please be sensitive and respect each other’s feelings and viewpoints.’
- Technical aspects of the debrief session are highlighted, for example, virtual attendees can have their cameras on or off, the Zoom chat function can be used for virtual attendees to express them-selves. Chat comments are monitored and brought into the conversation by our assistant psychologist.
- A brief initial summary of the case is presented by the neonatal consultant (up to five minutes) and the clinical psychologist asks each attendee to introduce themselves and describe their involvement in the case.
- The session is run as an informal conversation using Hobfoll’s trauma intervention principles.9 Staff are asked to share their experiences, feelings and connections to one another from working through the case.
- Our clinical psychologist concludes the session, summarising the main discussion points, drawing attention to learning points, and highlighting strengths of the team from their work on the case. Self-care strategies, signs of traumatic stress and additional staff support services are described.
A follow-up email is sent immediately after the session. This acknowledges the emotional/psychological challenges of the case and includes safety-netting on warning signs for traumatic stress, signposting to additional staff support services. A link to an anonymous feedback questionnaire is attached.
Lessons learnt
Through our experience of running the virtual and hybrid debrief sessions during the three-month pilot, we made the following three observations and recommendations:
Staff feedback themes
During the pilot, 19 staff attended virtually and 11 staff attended face-to-face. All attendees were emailed a questionnaire to capture their debrief experience. The response rate was limited: 37% for virtual attendees and 64% for face-to-face attendees. Despite this suboptimal response rate, there were evolving themes from the feedback received:
Theme 1: Virtual and face-to-face debrief attendance had similar staff psychological safety and impact profiles (TABLE 1).
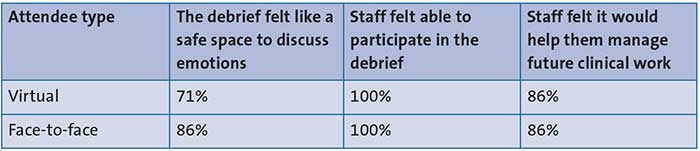
TABLE 1 Staff questionnaire feedback results.
Theme 2: Advantages of virtual debriefs for staff included accessibility, comfort and ease of ‘walking in’ late. Disadvantages included difficulty in sharing and reading emotional reactions, lack of physical contact, potential lack of emotional support afterwards, and computer sound/camera malfunction. Barriers to attending virtually included wanting to switch-off from work on days off and having other personal commitments.
Theme 3: Face-to-face debrief advantages included a more ‘personal’ feel, being able to read body language, increased interactivity/spontaneity, and cookies/brownies. Disadvantages of face-to-face debrief attendance included feeling there was nowhere to hide, having difficulties being heard in a big group, and finding it difficult to speak.
Conclusions
Our pilot suggests that virtual debriefs for neonatal staff can be offered as an alternative to face-to-face debrief sessions, or in combination with face-to-face sessions (hybrid debriefs). Our pilot study findings were presented locally and it was agreed that our NICU would continue to offer regular co-facilitated debriefs, both face-to-face and virtually.
Virtual debriefs pose unique challenges that should be addressed by careful design of the session to ensure psychological safety for staff. Specific considerations for instituting virtual debrief on your neonatal unit are provided in FIGURE 2. Our study is limited by its small size and suboptimal questionnaire feedback response rate. Larger studies are needed to create a reliable body of evidence on the impact of virtual and hybrid debrief for staff.
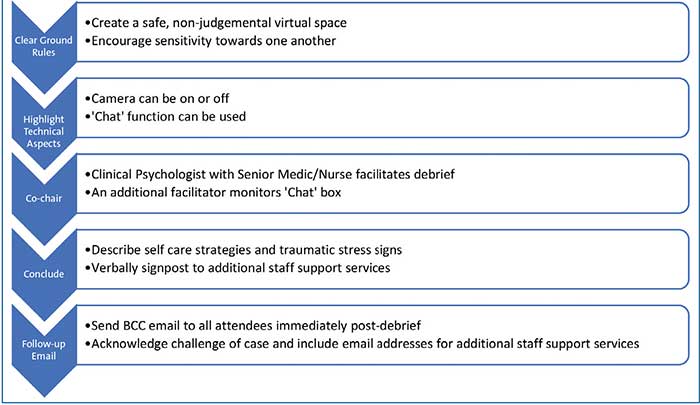
FIGURE 2 Specific considerations for instituting virtual debrief on your NICU.
Author contributions
SC: jointly planned and ran debrief sessions, processed feedback data, first author manuscript.
SJA: jointly planned and ran debrief sessions, processed feedback data, edited manuscript.
Or read this article in our
Tablet/iPad edition
- Literature evidence and national guidance recommends neonatal staff debrief following distressing clinical cases.
- There is scant evidence on holding virtual debriefs and their impact on staff attendees.
- We ran a virtual debrief pilot programme on our NICU for neonatal and associated specialty staff. The sessions were co-chaired by the NICU’s clinical psychologist and a neonatal consultant.
Also published in Infant:
