

Supraventricular tachycardia induced by a peripherally inserted central catheter in a preterm baby
Peripheral insertion of a central catheter is an essential procedure, which is frequently performed in extremely premature babies as well as those that are critically ill. This article reports on the case of a preterm infant who developed supraventricular tachycardia as a consequence of a malpositioned peripherally inserted central catheter in the cardiac chambers.
Ahmed Yousef
Neonatal Clinical Fellow,
Birmingham Women’s Hospital, Birmingham Women's and Children's Foundation NHS Trust
ahmed.yousef3@nhs.net
orcid.org/0000-0001-5009-1631
A 16-day-old preterm baby born at 33+5 weeks’ gestation (corrected gestational age = 36 weeks) was reviewed because of a sudden onset of tachycardia (heart rate = 250-330 beats/min). An electrocardiogram (ECG) showed supraventricular tachy-cardia (SVT) (FIGURE 1). Vasovagal manoeuvres (ice pack to the face) terminated the SVT to achieve normal sinus rhythm.
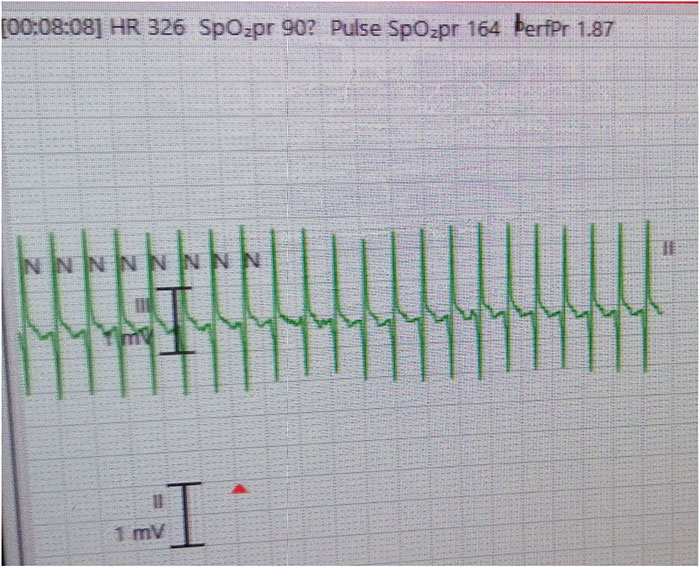
FIGURE 1 The ECG lead-II showing SVT (narrow-complex tachycardia; heart rate = 326 beats/min). No P waves can be seen.
The baby had a peripherally inserted central catheter (PICC) on day 7 of life. The insertion point was the right upper limb cephalic vein, just below the elbow joint. The chest X-ray taken at the time of insertion (at another hospital) was reviewed but the tip of the PICC line could not be visualised as there was an overlying temperature probe (FIGURE 2). Bedside targeted echocardiography was performed, which revealed the PICC line in the superior vena cava, right atrium and crossing the tricuspid valve to the right ventricle (FIGURE 3). The PICC was removed immediately. No further PICCs were inserted and the SVT did not happen again. Following removal, it was noted that the inserted length of the PICC was 16cm but the estimated length was 11cm (FIGURE 4).
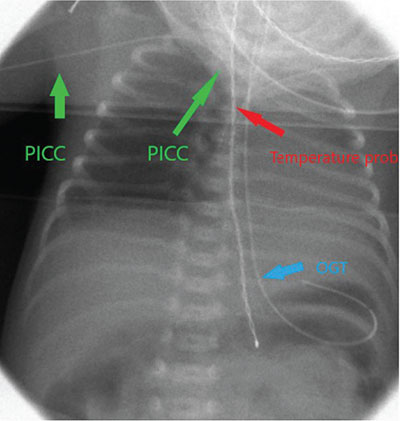
FIGURE 2 The chest X-ray taken at the time of PICC insertion. The PICC tip could not be seen due to the overlying probe. Key: OGT=orogastric tube.
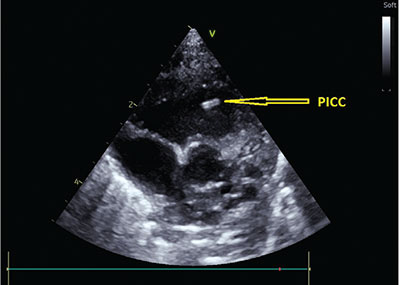
FIGURE 3 Targeted echocardiography showing the PICC (arrow) in the right ventricle (short axis view).

FIGURE 4 The PICC after removal. Note, the inserted length was 16cm but the estimated length was 11cm.
Discussion
Complications of indwelling neonatal PICCs can include central line-associated bloodstream infection, occlusions, catheter migration, catheter fracture, thrombosis, phlebitis, distal oedema, pleural or cardiac effusions, tamponade and arrhythmias.1 Cardiac arrhythmias in newborn infants are not uncommon, but they can sometimes be life-threatening. As a result, the bedside neonatologist should aim for early recognition and proper management of the condition, especially when it occurs with an indwelling central venous catheter. Even though various pieces of neonatal literature discuss the danger of arrhythmias in neonates with centrally inserted catheters, the incidence is unknown.2 There have been a few examples of arrhythmias caused by a central venous catheter, with tachy-arrhythmias being the most common. Atrial flutter and SVT have been documented as the most prevalent arrhythmias.3
The use of a PICC line is common practice in NICUs and staff must be aware of the hazards associated with their insertion and use. The optimal position for the distal tip of a PICC line is in the superior vena cava or inferior vena cava, outside of the cardiac silhouette. If the tip of the PICC cannot be clearly identified on an X-ray, repeat imaging is essential to rule out a misplacement. It is important to check catheter tip position in any infant with a PICC who suddenly develops an arrhythmia, even if the position at the time of insertion was optimal. There have been cases where the tip appears to have migrated after the initial X-ray.
Conclusion
Cardiac arrhythmias in infants with a PICC should alert clinicians to the possibility of inadvertent insertion into the heart chambers, which might provoke premature atrial and ventricular complexes and initiate SVT. In this patient, the tip of the catheter was confirmed in the right ventricle by targeted bedside echocardio-graphy. The SVT was managed conser-vatively by vasovagal manoeuvre.
Parental consent
Verbal consent for publication was obtained from the mother of the patient.
Or read this article in our
Tablet/iPad edition
- This case highlights a rare complication of upper limb PICC line insertion.
- Practitioners should be aware of correct insertion techniques and should always examine the vascular route of a PICC line and the PICC tip position to confirm correct placement.
- SVT may occur if the tip of the PICC line lies within the heart chambers.
Also published in Infant:
