

The impact of cognitive ergonomics in everyday clinical decision making and frontline tasks
Performing healthcare tasks relies on cognitive function involving mental processes such as perception, attention, memory, learning, information processing and decision making. However, the conditions of the healthcare environment can make it challenging for a human to perform cognitively demanding work tasks. This article considers the impact of cognitive ergonomics on everyday clinical tasks and decision making and asks, is it time to employ human factor ergonomic experts within clinical and governance teams?
Claudia Chetcuti Ganado
Consultant in Neonatal Medicine, Neonatal Intensive Care Unit, Luton and Dunstable Hospital
claudia.chetcutiganado@ldh.nhs.uk
The healthcare environment is a complex system where the consequences of error can be catastrophic. Working in health care requires a high degree of situational awareness. Frontline staff constantly process multiple sensory stimuli, including changes in the patient’s condition, verbally received information from team members and data from various pieces of high-tech equipment. Decision making can be compromised due to the stress associated with making life-or-death decisions within a short time frame, often in a state of fatigue. As with other big teams that work collaboratively, clinicians in different hospitals and in primary care need to access timely information that depends on the interoperability of data storage, flow and transfer among the different teams. Clinicians with varying levels of training, knowledge and familiarity with equipment also present likely sources of error.
Situational awareness involves being able to predict future states to plan the right action. The unpredictability of the human body makes it even more important for a clinician to be able to continually reassess a patient for newly emerging information and match whether the evolution of information agrees with the clinician’s prediction.1
Cognitive ergonomics
Cognitive ergonomics is the field of study that focuses on how well the use of a product matches the cognitive capabilities of its users. According to the International Ergonomics Association: “Cognitive ergonomics is concerned with mental processes, such as perception, memory, reasoning and motor response, as they affect interactions among humans and other elements of a system. The relevant topics include mental workload, decision-making, skilled performance, human-computer interaction, human reliability, work stress and training as these may relate to human-system design.”2 The first domains investigated by cognitive ergonomics were nuclear power plants and air traffic control systems.3 Cognitive ergonomics are particularly relevant in complex environments where significant focus is required to make life-or-death decisions.4
Impact of cognitive ergonomics on frontline decision making and tasks
Performing healthcare tasks relies on cognitive function and an analysis of the features of cognitive ergonomics can improve the interaction between the healthcare professional and other elements of the system (eg medical devices, working environment). Examples of mechanisms by which cognitive ergonomics impact on frontline decision making and tasks include: perception; comprehension and anticipation; and memory and learning.
Perception
The human brain can filter sensory information such that focus is selective, particularly during a task that requires sustained attention.5 In an intensive care setting the number of sensory stimuli can be huge. Oxygen monitors are constantly alarming and at times record small drops or rises in oxygen due to poor sensor pickup. Additionally, there are ventilator alarms and pump alarms that become background noise and may be subconsciously ignored, consciously ignored (through pattern recognition ability that they are due to sensor pickup) and even purposely disabled, with the potential for patient deterioration going unnoticed.
‘What you see’ is also a potential source of error when interpreting results. For example, a chest radiograph for a patient with respiratory symptoms likely directs attention to the lung fields such that the clinician may miss important information, for example a heart enlargement.
According to Ulrich Neisser’s model (1976), perception requires perceptual exploration taking into consideration sensory input from various sensory experiences. Perception is also influenced by a cognitive mapping process, which is dependent on how we perceive things.3 Humans are a visually oriented species; additionally, memory capacity can be increased by an individual’s ability to apply context in a particular situation.6 The ability to memorise is also dependent on an individual’s preferred method of learning, which is particularly relevant in maintaining situational awareness during clinical decision making.
The importance of perceptual exploration is relevant when a consultant is on call and receives phone calls about a patient. Despite attempts at ensuring the correct information exchange there is a significant sensory input that the clinician is missing. Awareness of this helps individual clinicians make informed decisions about whether they need to be on site to get a better grasp of what is happening. In this setting there may also be impaired cognitive processing, influenced by the stage of sleep the clinician is in when called.7,8
Comprehension and anticipation
The process of comprehension and anticipation depends on the mental models and schemas originating from the person leading a particular clinical setting. Mental models are formed by memorising previous positive interactions and experiences. Through mapping a situation to a particular mental model, the brain can generate schemas allowing us to take mental short cuts.9 It allows us to be able to process the vast amount of information around us in a fast and efficient way, but can cause us to exclude pertinent information and confirm our pre-existing beliefs. Mental models are often based on incomplete facts and intuitive perceptions; they can be further influenced by stereotypes and help shape our action and behaviour in a particular situation.
Consider a clinician working in the A&E department reviewing a patient with chest pain. The patient is 55 years old and a heavy smoker. The clinician interprets the symptoms of chest pain in the context of age and smoking practice is likely a heart attack. The clinician may unintentionally elicit the wrong information through ‘leading’ questions. The patient himself is prone to bias in memory recall as eyewitness testimony suggests that questions can influence memory recall. The patient may volunteer symptom description in line with the working diagnosis of a heart attack. This leads the clinician to confirm his existing belief that the patient has had a heart attack and potentially miss another diagnosis by failing to investigate accordingly.
This processing efficiency ability of the brain can also give rise to ‘automaticity’ errors.10,11 Paradoxically, these types of automaticity errors are potentially more likely with increasing experience as once a task is fully rehearsed, it requires less conscious effort to execute it.
While facilitating a simulation session of a baby with a team of four staff members with different levels of expertise, the author could recognise the mental models that emerged from the different individuals. The scenario setting was of a baby stable on external respiratory support who suddenly deteriorated. The senior clinician’s immediate action was to escalate respiratory support and request a chest radiograph. The senior nurse performed suctioning. The youngest and most junior nurse used the most scientific approach and followed a set protocol checking the disconnected equipment.
It was clear in this task that the generic error modelling system was at play and each member’s decision was dependent on other similar situations that offered the most likely action needed. Human factor science can help these life-or-death situations from being prone to automaticity errors by creating algorithms (such as exists in the newborn life support algorithm), planning the appropriate skill mix and empowering staff to contribute.
Memory and learning
Memorising depends on the human ability to encode, store, retain and retrieve information. Short-term memory capacity can be increased by chunking and coding. Healthcare staff constantly rely on the ability to learn and recall important facts that enable them to treat patients.
Human factor specialists
A human factor ergonomic specialist typically uses a holistic, systems approach to apply theory, principles and data to the design and evaluation of tasks, jobs, products, environments and systems. This takes into account the physical, cognitive, sociotechnical, organisational and environmental factors, as well as the complex interactions between the healthcare professional and other humans, the environment, tools, products, equipment and technology.2 The following sections give some examples of problematic scenarios on the neonatal unit and how the application of cognitive ergonomics might help.
Guidelines: the problem
Guidelines are used in clinical practice as a store of evidence-based information. Guidelines are often wordy, lengthy and difficult to memorise. They are often not available at the point of care and difficult to access during time-critical emergencies. Different guidelines can have conflicting information, which makes it difficult for the human brain to store the details.
Failure of memory recall can result from interference – where a new memory competes with an old memory for storage. In situations where guidelines are not consistent or even conflicting between different departments, it will be much harder for clinicians to be able to recall the right information at the right time.
How can cognitive ergonomics help? Formulating guidelines in a way that helps encode information, such as using categories and colour, can help clinicians to better translate information and retrieve it. Displaying important content at the point of care in a way that allows recognition, rather than recall, using cognitive aids can also reduce errors. A quality improvement initiative describing the impact of conflicting wordy guidelines showed how implementation of cognitive aids reduced the admission rate of babies with hypoglycaemia by half through correct management of infants at risk.12
Human errors in prescriptions: the problem
Prescription mistakes and errors are very frequent in healthcare settings. The commonest errors are mistakes with timing or missed doses (lapses), writing milligrams instead of micrograms (slips), and incorrect dosages prescribed (knowledge-based and rule-based mistakes).11 Despite training and frequent reminders, prescription errors continue to persist.
Often clinicians are approached ad hoc by nursing members to complete a prescription. The complexity of the prescribing process, unavailability of the right design systems, multi-tasking and the significant distractions from a noisy environment can predispose to error through cognitive overload (FIGURE 1).

FIGURE 1 Several doctors preparing several prescriptions while attending different patients in the ward round.
Knowledge-based mistakes can occur due to inability to recall the correct dose. Although this is often circumvented using electronic drug calculators, asking the doctor to multi-task during a ward round results in the clinician relying on memory to write the prescription. The formulary, or the calculator itself, on the computer desktop may be difficult to find due to a multitude of folders on the desktop (FIGURE 2).
FIGURE 2 Confusing documents on the computer desktop make it harder to spot the drug calculator (arrow).
A frequent recurring mistake is prescribing the dose in milligrams versus micrograms. This can result from a knowledge-based error, a slip or unclear documentation. To circumvent the problem with clarity, doctors are often asked to write milligrams and micrograms in full (rather than mg or µg). However, the design of the chart does not permit this (FIGURE 3).
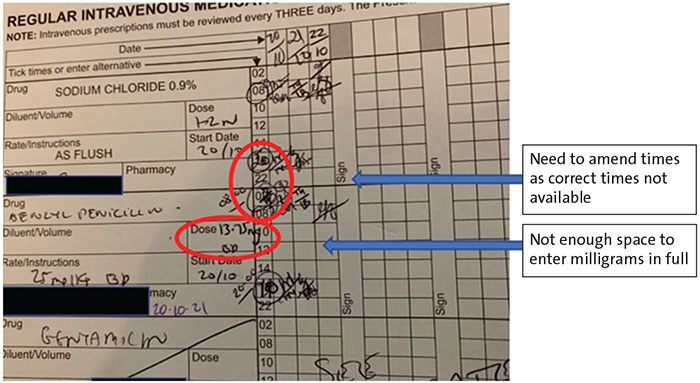
FIGURE 3 This drug chart design is not human centred.
Missed or late doses are one of the commonest errors. Drugs are given at timed intervals and the doctor is required to circle the times the baby needs to have medication. The clock hours on the chart do not support all timed administrations. This means that the chart needs to be physically amended, leading to potential error from recognition by the person administering the drug and also by the prescriber circling the wrong times (slips) in the expectation that the times displayed on the chart are appropriate.
Each baby has its own 24-hour clock for drug administration. The nurse needs to remember the timing of every single baby through continuous situational awareness. The grouping of similar medications that are not time sensitive could potentially reduce error through reduction of cognitive overload.13
How can cognitive ergonomics help? Although training and reminders are essential, relying on the human brain is the least effective method to prevent errors. Action planning should focus on human-centred design of prescription charts and an environment that will minimise the potential for cognitive overload. It also ensures the clarity and availability of the right tools at the point of care.
The hand hygiene saga: the problem
Hand hygiene has long been shown to prevent cross infection yet performance fluctuates despite frequent reminders. There are several posters aimed at human emotion, often misguidedly placed on sinks. There is no doubt that appealing to the human emotion will increase compliance of visitors but for the staff who work there daily, this may not be as effective as might be hoped. For an understaffed workforce tending to several competing tasks by the bedside, the poster near the sink can be invisible. In fact, it is likely that the poster will only be noticed if that member of staff approaches the sink to wash their hands (FIGURE 4).
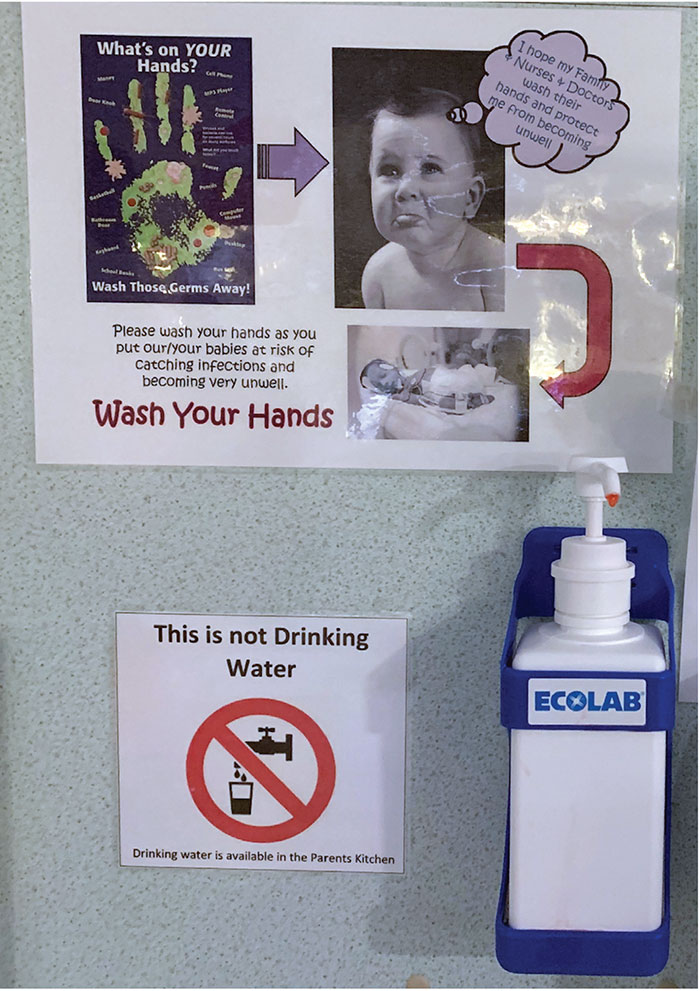
FIGURE 4 A hand washing poster misguidedly situated on the sink, which is behind the area where the cots are located.
How can cognitive ergonomics help? Posters with a human emotional element will work more consistently if they are strategically placed to attract attention at a critical timepoint in the patient-staff encounter. In the neonatal unit, a simple reminder such as ‘have you washed your hands to protect me?’ on the lock of the portholes, is probably much more effective than a poster on the sink.14
Simulation: the problem
Simulation has been imported into health care from aviation. In contrast to a flight simulator, the simulation doll provides no visual or tactile sensory input that clinicians learn to decipher through their patient encounters. The mental model that emerges will only be based on partial information processing. Currently, within the healthcare setting, scenarios are often based on the trainee establishing a diagnosis. Debrief often focuses around clinical performance dependent on the scenario diagnosis, which is withheld at the start.
How can cognitive ergonomics help? Simulation scenarios should assess whether trainees maintain situational awareness in a critical situation rather than attempt to formulate the diagnosis. Formulating a diagnosis without the ability of full perceptual exploration is very prone to error. Debrief in simulation should focus on: the ability of the team to communicate and maintain situational awareness; knowledge of when and how to escalate, and availability and use of the right equipment. Situational awareness measurement needs the trainee to take the facilitator through the cognitive thinking process, often lacking in clinical simulation settings. Recording or transcribing simulation is rare, thus limiting its effectiveness.
Forcing functions: the problem
Forcing functions can be very effective in preventing serious errors. Forcing functions include the inability to connect an intravenous syringe to an intrathecal needle or a nasogastric syringe to an intravenous cannula. These straightforward equipment design technologies are very effective as one element relies directly on the other.
Other forcing functions are less effective, especially those associated with information technology, leading to workers bypassing the system. Violations of this type occur if the staff member does not think that the function is necessary or if they think it feels safe to override it. It may also be perceived as slowing down the task. Commonly the staff member has seen several peers bypassing this ‘hindrance’.
How can cognitive ergonomics help? It is clear that if a forcing function is going to be implemented, the frontline users need to be convinced of the benefits of the intervention as well as the potential consequences of violation. Thus, getting their ‘buy in’ right at the start of their training is important. In addition, any forcing function should be tested for its frontline usability. A common problem seen on neonatal units is overriding the forcing function of the blood gas machine. In neonatal intensive care, a blood gas is often the first crucial investigation in planning the management of a critically unwell baby. The blood gas machine will only give a result if the baby’s hospital number is entered but having a hospital number requires the midwife to register the birth on a different system. This can be delayed if the midwife is attending to the mother. However, the neonatal team needs the blood gas result urgently so the neonatal nurse enters a random number and delivers the crucial blood gas result. Clearly here, frontline usability has not been well thought out.
Checklists: the problem
Checklists and care bundles are so-called cognitive aids. They are methods by which staff can minimise recall and act ‘SMART’ (in goal setting, SMART stands for specific, measurable, achievable, relevant and timely). Checklists are particularly effective in aviation. There are several checklists within health care that have been shown to be effective, such as the World Health Organization surgical checklists. These are evidence-based and their design, clarity, usability and effectiveness have been investigated. Checklists are very effective and straightforward for equipment checks. However, checklists produced by clinical staff with little or no human factor knowledge abound in health care. These documents often combine the function of a checklist, a care bundle and an algorithm. These are important factors when designing a cognitive support tool but it is very important that the user is aware what parts of the list are for ‘action’.
How can cognitive ergonomics help? When considering an algorithm where one action follows another, due importance needs to be given to the human perceptual and processing ability. An effective design will have a clear, less complex layout. It may involve function grouping and use of colour and familiar icons. This can only be achieved using expert design input, which is then thoroughly tested with frontline users.
Discussion
Cognitive ergonomics plays a major role in the clinical setting. Day-to-day clinical work and patient safety are prone to several potential sources of errors. Cognitive overload is likely as several stimuli compete passively for attention. The human ability to selectively filter information can itself lead to errors arising from unintentionally missing important information. High levels of stress can further predispose life-or-death decision-making errors. Senior clinicians are often called at irregular hours when complex emergencies require input and their decision making can be influenced by sleepiness and automaticity errors. More junior teams covering 24/7 shifts are more likely to be involved in knowledge and rule-based mistakes, that are potentially made worse by fatigue.
Even when equipment is professionally ergonomically designed, the environment in which it is used is often poorly designed, leading to potential for error. However, this poor design encountered with everyday paperwork, computer systems and cot spaces, can be remedied with little or no monetary requirement but through SMART action planning using cognitive ergonomics concepts.
Forcing measures that are not aligned with other processes often lead to workarounds, which may predispose to errors. Safety systems within a fast paced, understaffed environment can also lead to risk compensation and violation of policies where the safe systems are perceived to make tasks slower to complete.
Although well-embedded in many clinical settings, simulation can be limited in its effectiveness unless undertaken by knowledgeable staff who are aware of the potential pitfalls while training. Although cognitive aids such as checklists are common in the healthcare setting, they are often designed by clinicians with no human factor expertise and therefore content, design, clarity and usability are not appropriately tested.
Recommendations in response to incidents focus largely on training and awareness – the least effective action in the human factor hierarchy of controls. Training and awareness are necessary but will fail to achieve the intended outcome unless considered within the bigger scheme of things. Health care human factor training largely focuses on improving team functioning through the use of communication tools and the setting of psychological safety and this is certainly a very important element in health care.
Conclusion: the time is right for employing human factor specialists
Cognitively demanding work involving information overload, multi-tasking, disruptions and interruptions can have harmful consequences. It is unlikely that health care can ever aspire to be risk free but it is time for health care to invest in ergonomic safety experts within clinical and governance teams or working alongside clinicians. Only in this way can latent conditions that lead to human error be recognised and evidence-based design solutions used to support staff and reduce potentially harmful mistakes.
Or read this article in our
Tablet/iPad edition
- Healthcare professionals constantly process multiple sensory stimuli, making quick life-or-death decisions, often in a state of fatigue.
- Human factor ergonomic experts could decrease the harmful consequences of potential sources of error in day-to-day clinical work and patient safety.
