

Use of a novel human milk-based fortifier in a preterm baby
This article reports on the case of a premature baby with multiple complications who demonstrated poor weight gain and intolerance to bovine milk-based fortifier. A novel human milk-based fortifier (NeoKare MMF) was introduced, which was well tolerated and resulted in optimal weight gain. The course of the growth of the infant is discussed and the role of a human breast milk-derived fortifier is considered.
Pauline Adiotomre
Consultant Paediatrician
Neonatal Unit, Diana, Princess of Wales Hospital, Grimsby, Northern Lincolnshire and Goole NHS Foundation Trust
pauline.adiotomre@nhs.net
The case
Birth to day 7
A preterm baby was delivered by emergency caesarean section to his 20-year-old primigravid mother at 28+3 weeks’ gestation due to massive maternal antepartum haemorrhage. The mother received one dose of antenatal steroids and magnesium sulphate. The baby was born in good condition and received delayed cord clamping. He required continuous positive airway pressure (CPAP) with 30% oxygen via a face mask and was transferred to the neonatal unit.
The baby’s birth weight was 1.19kg (25-50th centile). He was intubated and given surfactant (Curosurf, Chiesi) via an endotracheal tube at 1.5 hours of life. He remained ventilated on assist control-pressure control, volume-guided ventilation for the first 19 hours of life and was then extubated onto bi-phasic CPAP, although during this time he had a number of reintubations due to accidental extubation. The baby’s umbilical lines were removed and a long line was inserted on day 1; total parenteral nutrition (TPN) was commenced. Trophic feeds of expressed breast milk (EBM) were started on day 3.
Soon after delivery the baby was started on (intravenous) IV benzyl penicillin and gentamicin, which were changed over the course of the following few days to flucloxacillin, gentamicin and metro-nidazole because of recurrent bradycardias, metabolic acidosis, periumbilical flare/skin infection of the abdominal wall, swelling and discharge behind the right knee and suspected necrotising enterocolitis (NEC). Because of suspected NEC, the baby was nil-by-mouth from day 6. An echocardiogram showed a small patent foramen ovale with left to right shunt and a moderately-sized patent ductus arteriosus with left to right shunt.
Day 8 to 15
The infant continued to have recurrent bradycardia, desaturation and apnoea despite being on triple antibiotics, fluconazole prophylaxis, nil-by-mouth and double-dose caffeine citrate (10mg/kg once daily). On day 8 he was reintubated and ventilated, he received a top-up transfusion due to low haemoglobin and he was transferred to the tertiary neonatal intensive care unit (NICU) at The Jessop Wing, Sheffield. At this stage, he had been ventilated for three days and received CPAP for six days. His weight on transfer was 1.19kg; he was on teicoplanin, gentamicin and acyclovir.
He was at the tertiary NICU from day 8 to day 15 and during this admission he was ventilated for four days and extubated onto bi-phasic CPAP and on CPAP/high flow therapy for four days. The gentamicin, teicoplanin and acyclovir were stopped on day 11 as blood cultures and swabs were negative. He was weaned off of TPN and onto full feeds of EBM on day 15. Half-strength bovine milk-based fortifier was started on day 15. He was repatriated back to the neonatal unit at Diana, Princess of Wales Hospital, Grimsby on day 15 of life at the corrected age of 30+4 weeks with a weight of 1.384kg (25-50th centile) on nasal high flow at 4L/min, in air. He was receiving two-hourly nasogastric tube feeds.
Day 16 to 30
On day 16/17 his nasal high flow requirement increased to 6L/min in up to 25% oxygen. He was on continuous nasogastric tube feeds due to vomiting episodes. The volume of feeds was reduced from 150mL/kg/day to 90mL/kg/day and he was also given 60mL/kg/day of intravenous fluids. His weight dropped to 1.290kg (9-25th centile) on day 17. The bovine milk-based fortifier was stopped as it appeared that the baby was not tolerating it.
On day 18 the infant was started on erythromycin and he remained on continuous nasogastric feeds of EBM. On day 21 he was screened for infection and started on IV antibiotics for five days for presumed sepsis. His dose of caffeine citrate was increased from 10mg/kg/day to 20mg/kg/day because of recurrent bradycardias and desaturations. He had poor weight gain from day 19 to day 30. On day 19 he weighed 1.29kg. On day 25 he weighed 1.34kg (2-9th centile). During this period, he was on continuous nasogastric feeds at 150mL/kg/day. He continued to have desaturations and bradycardias requiring stimulations and oxygen. On day 30 his weight remained relatively static at 1.390kg (2-9th centile).
Day 30 to 53
The infant was started on a human milk-based fortifier (NeoKare MMF) on day 30. On day 32 he weighed 1.5kg (2-9th centile). Nasal high flow therapy was stopped on day 37. Probiotic drops (Labinic, Biofloratech Ltd) were stopped on day 39 and caffeine citrate was stopped on day 40.
The baby was given another top-up blood transfusion on day 44 as his haemoglobin was 82g/L. He continued on the mother’s EBM and human milk-based fortifier. He had recurrent desaturations and bradycardia and continued with sodium and potassium supplements, lansoprazole (to reduce stomach acid), multivitamin drops (DaliVit), sodium feredetate (to prevent iron deficiency) and erythromycin. He started on some bottle feeds of EBM on day 48; he was tube and bottle fed at this stage. He developed pedal oedema and was noted to have intermittent systolic murmurs.
At 36 weeks of age, on day 53, he weighed 2.098kg (2-9th centile) and the human breast milk-derived fortifier was stopped, in line with the unit policy (breast milk fortifier is stopped when the baby reaches 2kg). A chest X-ray showed congested lungs and he was given an IV dose of the diuretic, furosemide, and later commenced on other diuretics (spironolactone and chlorothiazide).
Day 58 to 79
Infant Gaviscon was added to the baby’s treatment on day 63 as he was bringing up clear fluids and desaturating around the time of feeds. His weight was 2.13kg at 37+3 corrected weeks of age (0.4-2nd centile). As the mother’s breast milk supply was dwindling, Nutriprem 2 (Nutricia) was added to her breast milk on day 64. Following this, the infant had episodes of increasing abdominal distension. The feeds were temporarily stopped and abdominal X-rays revealed only bowel gas distension (FIGURE 1). On day 70, he weighed 2.33kg (0.4-2nd centile). The Nutriprem 2 was stopped on day 71 and Nutramigen Lipil 1 (Mead Johnson Nutrition; lactose free and used for cow’s milk intolerance) was added to the mother’s breast milk.

FIGURE 1 An abdominal X-ray showing distended bowel loops on day 66.
The infant underwent a sleep study on 0.1L/min of oxygen, which was unsatisfactory. He remained on 0.2L/min of oxygen via a nasal cannula. At this stage, it was felt that he had chronic lung disease, gastro-oesophageal reflux disease and cow’s milk protein intolerance. Screens for retinopathy of prematurity were unremarkable as were cranial ultrasound scans.
He had his first batch of immunisations on day 58 and palivizumab (for the prevention of serious respiratory tract infection caused by respiratory syncytial virus) on day 77. At 39+4 corrected weeks of age, his weight was 2.525kg (0.4-2nd centile). From day 79, he received only Nutramigen Lipil 1 by bottle as there was no EBM available.
Discharge
Upon discharge at 39+5 corrected weeks of age, he weighed 2.60kg (0.4-2nd centile). He was discharged home on: home oxygen, sodium feredetate, DaliVit, lansoprazole, erythromycin, chlorothiazide, spironolactone and Nutramigen Lipil 1 feed. Follow up arrangements were made with the community nursing team and for the baby clinic and the cardiac clinic.
Human milk-derived fortifier: observations
Recently introduced to the UK, NeoKare’s novel human milk-derived fortifier is made from human breast milk with added calcium and phosphorous. According to the manufacturer, NeoKare MMF (mother’s milk fortifier) retains the oligosaccharides, minerals, amino acids, vitamins and immunoglobulins found in human milk and helps premature and low birth weight infants fed EBM (either mother’s own or donor) to reach their unique nutritional targets.
TABLE 1 and FIGURE 2 show the timeline and growth chart of the infant. TABLE 2 summarises the results observed using fortification with NeoKare MMF in this preterm infant.
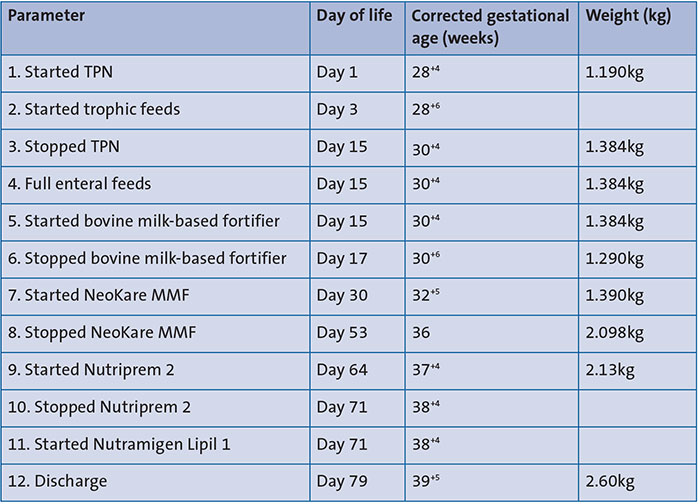
TABLE 1 The timeline of feeds and weight.
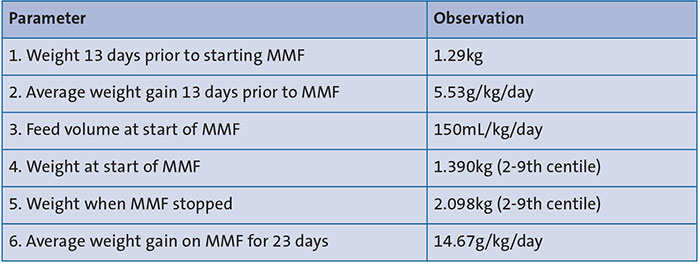
TABLE 2 Fortification with NeoKare MMF: observations.
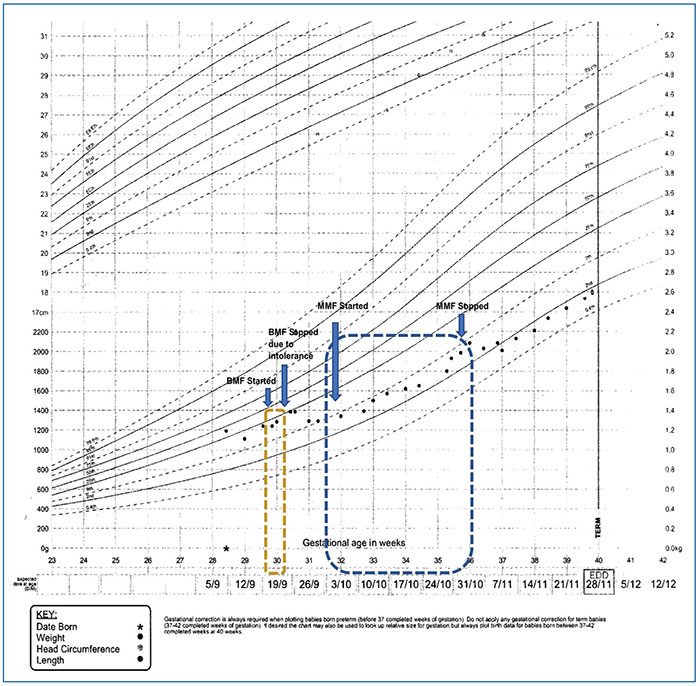
FIGURE 2 The infant’s growth chart (based on boys aged 22-42 weeks’ gestation).
Conclusion
A very premature infant born at 28+3 weeks’ gestation with a birth weight of 1.190kg was treated in the neonatal unit with multiple complications, in particular: suspected NEC, a small patent foramen ovale with left to right shunt and a moderate-sized patent ductus arteriosus with left to right shunt. The baby appeared to be intolerant of bovine milk-based fortifier and had poor weight gain (5.5g/kg/day). Hence, the bovine milk-based fortifier was stopped and a novel human milk-based fortifier was introduced, which appeared to promote optimal weight gain (14.7g/kg/day) and good feed tolerance. The human milk-based fortifier worked well as a ‘rescue fortifier’ for a preterm infant showing intolerance to bovine milk-based fortifier.
Declaration and parental consent
The author has not received any contributions (in the form of payment or free products) from any formula milk or human milk-based fortifier companies.
Verbal consent for publication was obtained from the mother of the patient.
Or read this article in our
Tablet/iPad edition
- Use of a novel human milk-based fortifier contributed towards optimal weight gain in a preterm infant with multiple complications.
- Human milk-based fortifier was used as a ‘rescue fortifier’ in a preterm infant with intolerance to bovine milk-based fortifier.
Also published in Infant:
