

Optimising the management of respiratory distress in late preterm and early term babies
Respiratory distress is a common reason for neonatal unit admission in late preterm and early term infants. These babies are also more likely than their full-term counterparts to experience long-term respiratory problems. A lack of research in this large group of babies has led to very wide variation in clinical practice, which may affect outcomes. The SurfON multicentre trial is investigating whether early administration of surfactant, when compared to expectant management, reduces the length of neonatal hospital stay and reduces the progression to more severe respiratory illness for late preterm and early term babies with respiratory distress.
Elaine M Boyle1
Professor of Neonatal Medicine
eb124@le.ac.uk
Charles C Roehr2,3
Professor of Neonatology and Perinatal Research
On behalf of the SurfON Study co-investigators and colleagues at the National Perinatal Epidemiology Unit Clinical Trials Unit (TABLE 1)
1Department of Health Sciences, University of Leicester
2National Perinatal Epidemiology Unit, University of Oxford

TABLE 1 Members of the SurfON Study team. Key: NPEU CTU=National Perinatal Epidemiology Unit Clinical Trials Unit.
Respiratory distress is one of the most common reasons for admission to a neonatal unit (NNU) in babies born late preterm and early term. A significant number of these babies will have surfactant deficiency. In contrast to very preterm babies, there is no evidence base for optimal management of early respiratory distress in these more mature babies. The use of surfactant in this group is therefore controversial, with practice being opinion-based and extremely variable both between and within NNUs. Clinical opinion is divided: some wish to treat these babies proactively, early in the course of their disease; others prefer to adopt an expectant management approach. However, large numbers of these more mature babies exert a substantial burden for neonatal services, with significant respiratory disease likely to lead to prolonged mother-baby separation and extended hospital stay.
Optimising the management of babies with respiratory distress could lead to more rapid recovery; a reduction in the number of days of intensive care, mechanical ventilation and non-invasive respiratory support; and reduced separation time for mothers and babies, thereby increasing the likelihood of early, successful establishment of breastfeeding and fewer long-term respiratory complications.
The SurfON study is the first randomised controlled trial (RCT) specifically focused on this population and seeks to determine the most appropriate approach to management of respiratory distress in this large and important group of babies.
Late preterm and early term babies
There are around 35,000 late preterm (34-36 weeks’ gestation) and 130,000 early term (37-38 weeks’ gestation) live births per year in the UK.1 Historically, it was believed that both short- and long-term outcomes for these babies were no different from babies born at full term (39-41 weeks). However, research during the past decade shows that long-term outcomes for late preterm and early term babies are less favourable across multiple domains. From the health perspective, this is particularly the case for respiratory diseases such as asthma and respiratory infections. 2-5
A gradient of risk is now recognised, extending from the most immature infants at the margins of viability, up to the most mature post-term infants. It is no longer considered appropriate to regard gestational age as a dichotomy of term versus preterm birth. This article seeks to discuss the challenges around the management of respiratory disease in more mature babies born before full term.
A historical perspective
Advances in modern obstetric and neonatal techniques and care have led to the survival of increasingly immature preterm babies. However, it is well recognised that many of these babies have severe neonatal respiratory disease related to lung immaturity and deficiency of surfactant production, which can have long-lasting effects.6 The relatively recent advent of advanced respiratory support, exogenous surfactant and antenatal corticosteroid treatment has revolutionised the early respiratory care of very preterm babies born before 32 weeks’ gestation.
Prior to this, babies born at much later gestational ages were considered to be among the most immature and sickest. Babies born at 34-36 weeks of gestation came to be regarded as ‘near term’ and were, for many years, managed in much the same way as those born at full term. A lack of prospective research in these more mature babies has limited our understanding of this much larger group; however, recent evidence suggests that treating these babies as ‘mature’ may not always be appropriate.
Lung development and pathophysiology of respiratory distress
Preterm lung disease is generally associated with birth before 34 weeks of gestation; however, the lungs are still not fully mature, even at 34 weeks. In the third trimester, the developing lungs undergo rapid growth, and there is a transition from the fetal terminal saccular period to the alveolar period of development.7 During the late saccular phase of development, numbers of bronchi increase and the saccules begin to form alveoli.8 Surfactant production also begins at this time. Between 36 weeks and full term, the alveolar phase of lung development occurs, which does not end at the time of birth, but continues into childhood.
Early birth has the potential to interrupt these important and progressive phases of lung maturity, with resulting delay in reabsorption of lung fluid, decreased gas exchange, and decreased production of surfactant around the time of birth.9
Lung immaturity with related surfactant deficiency may be the cause of respiratory distress but this vulnerability of the immature lungs to disease processes and infection2 may also be exacerbated by other factors such as elective pre-labour caesarean section delaying clearance of lung fluid, maternal conditions such as pre-pregnancy or gestational diabetes, as well as birth through meconium-stained liquor and intrauterine or postnatal exposure to infection.10,11
Long term respiratory outcomes
Studies of long-term outcomes have shown that children born late preterm or early term experience higher rates of respiratory problems and have impaired lung function, when compared with babies born at full term.3,12 Increasingly, observational data suggest that respiratory morbidity in this group may persist into adolescence and adulthood.5,13 Recurrent respiratory health problems in large numbers of babies, even if these are not extremely severe, present an ongoing burden – not only for affected individuals with respect to their health, education and employment, but also at a population level for healthcare services.14 We do not know whether the mild degree of immaturity in these babies accounts for the longstanding adverse effects on respiratory health, or whether other factors play a part, such as the neonatal management of early breathing difficulties.
Presentation and management of early respiratory disease
Evidence for effective stabilisation, appropriate initiation of respiratory support and proactive management of respiratory disease is established for very preterm babies. 15,16 However, much greater uncertainty surrounds the management of more mature babies with signs of respiratory distress.
For the majority of late preterm and early term babies, neonatal care can be provided alongside their mothers on a normal postnatal ward. However, a substantial minority require admission to a NNU. Early respiratory disease is one of the commonest reasons for admission and respiratory distress syndrome (RDS) is a common respiratory diagnosis.17 These babies may present soon after delivery and require immediate medical support and admission for neonatal specialist care (FIGURE 1). Others will initially be cared for with their mothers but then, over a few hours, go on to develop signs of respiratory distress such as tachypnoea, grunting or increased work of breathing, prompting medical review and intervention.

FIGURE 1 A late preterm infant (35+1 weeks’ gestation) with significant respiratory distress at birth (subcostal and intercostal recessions). Written consent for publication of this image was provided by the patient’s parent.
RDS is due to lung immaturity and the associated deficiency of surfactant production. Surfactant is produced in the lungs to reduce alveolar surface tension and improve lung compliance. The treatment for RDS is exogenous surfactant, administered either via an endotracheal tube in an intubated baby or a small catheter into the lungs (less invasive surfactant administration; LISA) or, more recently, via a laryngeal mask. The risk of RDS increases with increasing prematurity and, although primarily associated with very preterm infants, RDS also occurs in late preterm and early term infants.10,11 Transient tachypnoea of the newborn, respiratory infection and meconium aspiration can also present with respiratory distress in the first hours of life and these are associated with secondary inactivation of surfactant.11,18 Surfactant therapy is most effective if given early in the course of respiratory disease.15 Very preterm infants with significant RDS are routinely treated with surfactant early.19 In contrast, for the bigger and more mature babies, it is often assumed that their lungs have reached full maturity and the possibility of surfactant deficiency may not be considered.
Many late preterm and early term infants with respiratory disease do not require urgent intubation at birth, yet have some degree of respiratory compromise. Larger, more mature infants are more likely than the most immature to cope during this period without the need for mechanical ventilation. In UK NNUs it is common to initially manage late preterm and early term babies with signs of respiratory distress but not requiring urgent intubation at birth, with non-invasive respiratory support (nasal continuous positive airway pressure, nCPAP, or high flow therapy). In some of these babies, respiratory signs resolve within an hour or two but, in a significant proportion respiratory distress worsens, oxygen requirements rise, and a prolonged period of non-invasive support, oxygen therapy or mechanical ventilation ensues. Clinically, it is often challenging to predict those babies that will recover quickly and those that will not. It is likely that either primary or secondary surfactant deficiency is present in many of these babies. However, in the absence of research evidence or clinical consensus, surfactant administration in this population is at the discretion of the clinicians based on their opinion and experience, and practice is very variable between and within NNUs.20,21
There are no universally acknowledged thresholds for intervention based on severity of respiratory distress or oxygen requirement.22 Radiological changes are often non-specific, so chest X-ray at this early stage may not contribute greatly to decision making. Some clinicians choose to treat respiratory illness early in its course to prevent deterioration, while others hope that surfactant will never be required and delay administration until the baby deteriorates to a point where the clinical condition mandates intervention. Both of these approaches constitute two ends of a spectrum, and fall within the bounds of ‘usual’ practice, but what constitutes ‘optimal’ practice is currently unknown.23 With the former strategy, it is possible that some babies who receive early surfactant would have recovered without it. With the latter ‘watch and wait’ approach, it is possible that some babies would receive surfactant too late to receive the greatest beneficial effects or might develop complications of untreated RDS, such as pneumothorax.
Surfactant is a costly drug requiring airway manipulation and as such, its judicious use should be guided by sound evidence, which is currently lacking for late preterm and early term babies. A recently published systematic review confirmed a paucity of high-quality evidence for management of respiratory distress in late preterm and term infants and widely differing thresholds for intervention with surfactant; further trials in this area were recommended.20 There is, therefore, a need to define the most clinically effective and cost-effective approach to early respiratory management in this population.
Impact on families and neonatal services
We should not underestimate the negative impact for mothers and families of having a sick baby at this gestation. Unexpected prolonged neonatal hospitalisation and separation of mothers and infants causes significant psychological distress for families. Many late preterm and early term neonates who are ‘well’ are sleepier and less eager to breastfeed than their full-term counterparts. Respiratory illness and separation make breastfeeding challenging and breastfeeding rates are low in both late preterm and early term infants.24,26 Being unable to successfully breast feed is often interpreted as a personal failure, which may affect maternal well-being.27
For NNUs, late preterm and early term births form a substantial part of the workload and can generate high costs for the NHS. If the neonatal stay is prolonged this can lead to lack of capacity for sicker or more preterm infants needing tertiary level care. Provision of neonatal care for more mature infants is spread across all levels of NNUs. Infants who become very sick and require respiratory support in a local neonatal unit often need to be transferred to a neonatal intensive care unit for ongoing management. This carries risks for the infant associated with transport and incurs high costs for the NHS and for families who have to travel to visit their baby.
Research in late preterm and early term babies
To date, there have been no RCTs of any aspect of care for babies born at late preterm and early term gestation. Increasingly, data from large observational studies are giving cause for concern about adverse long-term cognitive, behavioural, educational and health outcomes of these babies that, although not at the most severe end of the spectrum, are significant because of the numbers of individuals affected. It is not currently known whether differences in early management in the neonatal period contribute to these observed outcomes.
The SurfON Study
SurfON (Surfactant Or Not) is a multi-centre, pragmatic RCT of early surfactant therapy versus expectant management in late preterm and early term infants with respiratory distress.28 It is investigating whether the use of early surfactant reduces the progression to severe respiratory disease and reduces the length of hospital stay in babies requiring non-invasive respiratory support within a few hours of birth, compared to expectant management. SurfON aims to recruit 1,522 babies born between 34+0 and 38+6 weeks’ gestation from 45 NNUs across the UK. Mothers are also recruited as participants to assess the effects on infant feeding, length of maternal hospital stay and maternal quality of life.
Study outcomes
Primary outcomes
There are two co-primary outcomes for SurfON:
- Length of hospital stay from trial entry to discharge home
- Severity of respiratory illness.
Data from previous studies suggest that a late preterm baby with respiratory disease requiring non-invasive support stays in hospital for 10-15 days.25,29,30 A reduction in hospital stay by two or more days would therefore be beneficial for babies, families and the NHS. A decrease in the number of babies developing severe respiratory disease would reduce the need for intensive and high dependency care, pressure on neonatal services and reduce associated costs.
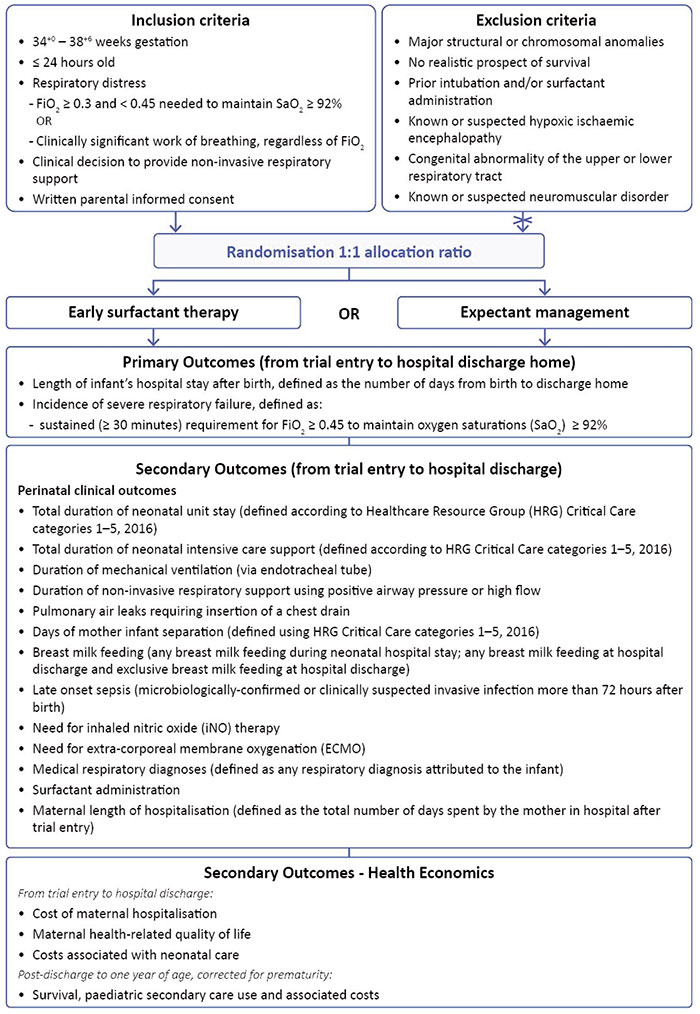
FIGURE 2 SurfON Study inclusion criteria and outcomes.
Secondary outcomes
The study assesses the effects of early surfactant administration on a large number of secondary outcomes including:
- intensive care stay
- infant morbidities
- infant feeding
- mother-baby separation (FIGURE 2).
Mothers participating in the study complete a health-related quality of life questionnaire at entry to the study and at the time of the baby’s discharge home. There is no face-to-face follow-up, but the study includes health economic analysis of post-discharge outcomes and costs of hospital admissions from discharge to up to one year of age using linked data.
Eligibility, recruitment and randomisation
Any baby where there has been a decision to provide non-invasive respiratory support (nasal CPAP or nasal high flow therapy) because of clinically significant work of breathing, with or without an oxygen requirement, is eligible to participate in the study. Ideally, to gain maximum potential benefit the babies should be recruited as soon as possible after a decision to provide respiratory support is taken, at a point where there is uncertainty about how the disease will progress. For the majority of babies, this is likely to be within 2-8 hours of birth, but babies are eligible to participate until 24 hours of age.
Study intervention
Early surfactant
The SurfON study intervention is a single dose of surfactant (Curosurf, Chiesi Farmaceutici S.p.A., Parma, Italy) given using LISA or via laryngeal mask airway. A brief period of intubation is also acceptable where this is the usual policy, with extubation following at the earliest possible opportunity.
Expectant management
Babies randomised to the expectant management group should be maintained on non-invasive respiratory support alone, at least until a more severe level of disease has been reached in order to achieve separation between the two randomised groups. Study guidance defines this as a sustained period (≥30 minutes) with a requirement of FiO2 ≥45% to maintain oxygen saturations of ≥92%. Where the baby’s condition deteriorates rapidly and sufficiently to mandate intervention before this time, the decision to intubate and/or give surfactant should be made by a senior clinician.
Conclusions
Risks associated with birth at late preterm and early term gestation have been overlooked for many years. Recent observational studies have indicated that respiratory disease is a significant problem for late preterm and early term-born infants, even into childhood, adolescence and young adulthood.2,4,11,31 Respiratory disease in the neonatal period is common and there are widely disparate opinions about how this should be managed. Currently, there is no evidence from high quality randomised trials to guide clinical practice, which has led to huge variation in practice in this group of babies. There is a need to redress the balance and determine the most clinically effective and cost-effective care to optimise early and long-term outcomes for this large group. To our knowledge, SurfON is the first large trial in the world focusing on improving respiratory health of late preterm and early term infants.
Conflicts of interest
EMB and CCR have acted as consultants for Chiesi Pharmaceutical, UK.
Funding
National Institute of Health and Care Research (NIHR): Multicentre open label, pragmatic RCT of early surfactant therapy versus expectant management in late preterm and early term infants with respiratory distress. Award ID: 17/89/07 (https://fundingawards.nihr.ac.uk/award/17/89/07). The authors would like to thank Bliss charity for its support on the trial.
Or read this article in our
Tablet/iPad edition
- Late preterm and early term babies are a large and under-researched group.
- Management of respiratory distress in mature infants born before full term varies widely.
- The SurfON Study is a large multicentre randomised controlled trial of early surfactant compared with expectant management in babies born at 34-38 weeks of gestation with respiratory distress.
Also published in Infant:
